Article Text

Statistics from Altmetric.com
The duplication of the inferior vena cava (IVC) is a rare anomaly, present in 1–3% of the general population. It is important to identify this anomaly to avoid uncontrollable bleeding in surgeries involving the main abdominal vessels.1
The IVC system begins its embryonic development at the 6th to 8th week of gestation, and after multiple anastomoses and regressions it concludes with the conformation of its four segments (intra-hepatic, supra-renal, renal, and infra-renal).2
Double IVC variants include retro-aortic renal vein (prevalence 2.1%), IVC interruption with azygos/hemi-azygos continuation (prevalence 0.6%), and IVC duplication (prevalence 0.2–3%).2 There are other variants (circum-aortic renal vein, left IVC, multiple renal veins, etc) that have an even lower reported prevalence in the global population.
These variants can be silent, diagnosed as an incidental finding after pre-operative imaging studies, or have hemodynamic repercussion. They can be a risk factor for deep vein thrombosis (predisposing to venous stasis even in the presence of a compensatory collateral system) and sometimes they are associated with congenital malformations (cardiac, splenic, renal).2 3
There are few reports on retroperitoneal lymphadenectomy in patients with double IVC anomaly.
Pre-operative imaging techniques make it possible to plan surgeries and avoid possible confusions of the IVC variants with false diagnoses of masses, retroperitoneal lymph nodes, or with other vessels such as a dilated ovarian vein.
The major goal is the prevention of iatrogenic vascular injury.3 4
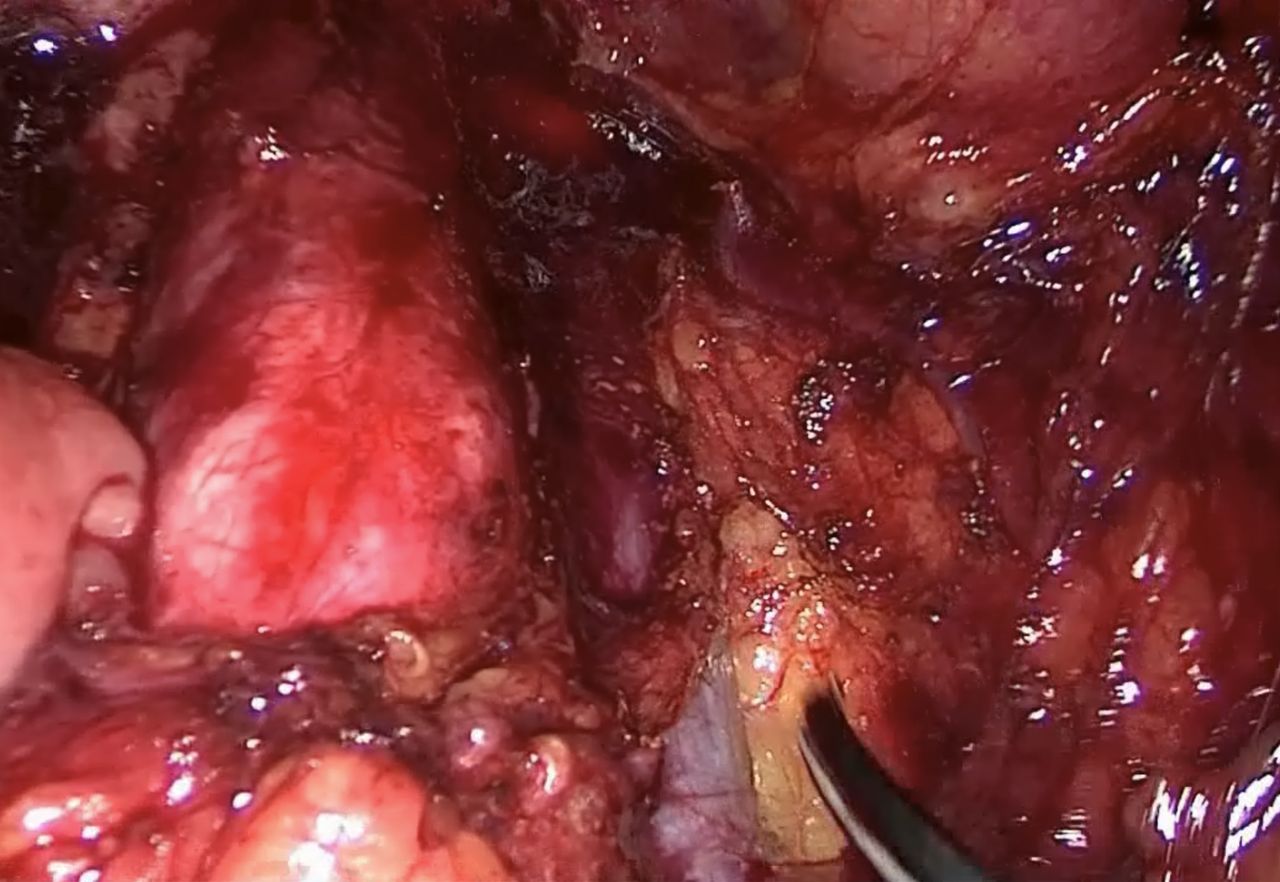
Through a laparoscopic transperitoneal para-aortic lymphadenectomy approach we performed an anatomical dissection focusing on abnormalities of the IVC, regarding the challenging anatomy seen in two operation fields.
Pre-operative enhanced CT revealed a double IVC flow pattern. This was essential not only to determine the local tumor extension and detection of distant disease, but also to plan and guide interventions without major bleeding complications.
Conclusions
It is important to obtain a detailed pre-operative imaging diagnosis that allows surgical planning to avoid major complications.
For intra-operative management we recommend performing an accurate dissection, to achieve exposure and gain knowledge on how to repair vascular structures.
Nowadays, the incidence of iatrogenic vascular injury in cases of IVC variants is not reported. Further data collection is suggested.

Duplicated inferior vena cava in front of the aorta in a laparoscopic transperitoneal para-aortic lymphadenectomy in a patient with uterine carcinosarcoma.

{kind=link}
{kind=link}
Data availability statement
Data are available upon request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants. The project is registered in accordance with the provisions of Foral Law 17/2010, of November 8, on Rights and Duties of people in matters of health in the Autonomous Community of Navarra, Spain, which guarantees the right to privacy and confidentiality in any activity of biomedical research and in teaching projects and also regulates the access and uses of the clinical history and the obligation to preserve the personal identification data of the patient separated from those of a clinical-assistance nature, so that anonymity is ensured, except that patients themselves have given their consent. Participants gave informed consent to participate in the study before taking part.
Footnotes
Contributors No conflict of interest. We wish to provide an educational video article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.