Article Text

Abstract
Background In patients treated for advanced ovarian cancer not suitable for complete primary surgery, interval surgery after three courses of neoadjuvant chemotherapy has been considered standard management since the EORTC randomized trial published in 2010. An alternative approach with delayed surgery after six courses of neoadjuvant chemotherapy was reported in retrospective series.
Primary Objectives To assess the efficacy on progression free survival of interval cytoreduction surgery after three cycles of neoadjuvant chemotherapy compared with delayed surgery after six cycles of neoadjuvant chemotherapy.
Study Hypothesis In women with ovarian cancer not suitable for primary surgical cytoreduction, surgery after six cycles of neoadjuvant chemotherapy will prove better disease-free survival than cytoreductive surgery after only three cycles.
Trial Design CHRONO is a multicenter, randomized phase III trial. After three courses of neoadjuvant chemotherapy, eligible patients will be randomized (1:1) to either completion surgery followed by an additional five cycles of chemotherapy (control arm) or an additional three cycles of neoadjuvant chemotherapy followed by completion surgery and then two additional cycles of chemotherapy (experimental arm). Patients in both groups will receive eight total cycles of chemotherapy.
Major Inclusion/Exclusion Criteria The main inclusion criteria are histologically confirmed epithelial high-grade serous or endometrioid ovarian cancer, documented FIGO stage IIIB–IVA unsuitable for complete primary surgery but considered resectable after three courses of neoadjuvant chemotherapy. The main exclusion criteria are mucinous, clear cell, carcinosarcoma, or low-grade serous histologies.
Primary Endpoint The primary endpoint is progression-free survival.
Sample Size 210 eligible patients
Estimated Dates for Completing Accrual and Presenting Results The estimated date for completing accrual will be Q2 2023. The estimated date for presentation of the first results is Q3 2028.
Trial Registration Number NCT03579394.
- Surgery
- Ovarian Cancer
- Gynecologic Surgical Procedures
Data availability statement
All data relevant to the study are included in the article.
Statistics from Altmetric.com
INTRODUCTION
Ovarian cancer is the leading cause of death from gynecological malignancies and, in most cases, is diagnosed at an advanced stage. Currently, the standard treatment is based on complete surgery, with no gross residual, and six courses of platinum and paclitaxel adjuvant chemotherapy.1 For patients whose tumors cannot be debulked optimally without residual disease and for those who have a poor performance status or other morbidity, performing comprehensive upfront surgery may be contraindicated. Neoadjuvant chemotherapy may decrease the peritoneal disease burden thereby making it possible to obtain complete cytoreduction.
Four randomized trials have defined the number of neoadjuvant chemotherapy courses before interval surgery as either three or four cycles. Authors have compared patients with FIGO III–IV ovarian cancer, treated randomly with primary surgery followed by adjuvant chemotherapy, with patients treated with three courses,2 or three to four3 courses of neoadjuvant chemotherapy followed by interval surgery and the last courses of chemotherapy. However, it appears that for different reasons—logistic, or due to the patient or the disease—the number of surgeries performed after more than four courses of neoadjuvant chemotherapy is increasing. Luykx et al reported that the number of surgeries after more than six courses of neoadjuvant chemotherapy was 13%, and recently Delga et al showed that the rate was 33%.4 5 A prospective assessment of the impact of complete surgery on survival after six cycles of neoadjuvant chemotherapy courses for patients not initially suited to complete primary surgery has not been performed.
In advanced ovarian cancer, interval surgery is performed between three courses of neoadjuvant chemotherapy and three courses of adjuvant chemotherapy, while in other cancer sites such as breast cancer6 or high-risk soft tissue sarcoma,7 when neoadjuvant chemotherapy is given, surgery is performed at the end of chemotherapy and a post-operative adjuvant course of chemotherapy is not given. In order to adapt this concept to advanced ovarian cancer, the authors put the case for performing complete surgery after the six neoadjuvant chemotherapy courses.8 Delaying surgery to after six neoadjuvant chemotherapy courses could reduce surgical complexity, reduce post-operative mortality/morbidity, increase the rate of complete surgery, and increase the rate of pathological complete response. Until now, the outcomes for delayed surgery after six neoadjuvant chemotherapy courses have been described only in mainly retrospective, mono-institutional, non-randomized series with small numbers of patients, heterogeneous inclusion parameters, and a variety of reasons for delaying surgery.8–10
CHRONO is an ongoing, prospective, multicenter, randomized phase III trial aimed at assessing the impact of delayed surgery after six courses of neoadjuvant chemotherapy in patients treated for advanced ovarian cancer and not initially a candidate for complete primary surgery, followed by the standard of care, including maintenance with bevacizumab, poly-ADP ribose polymerase (PARP) inhibitors, or both.
METHODS AND ANALYSIS
Trial Design
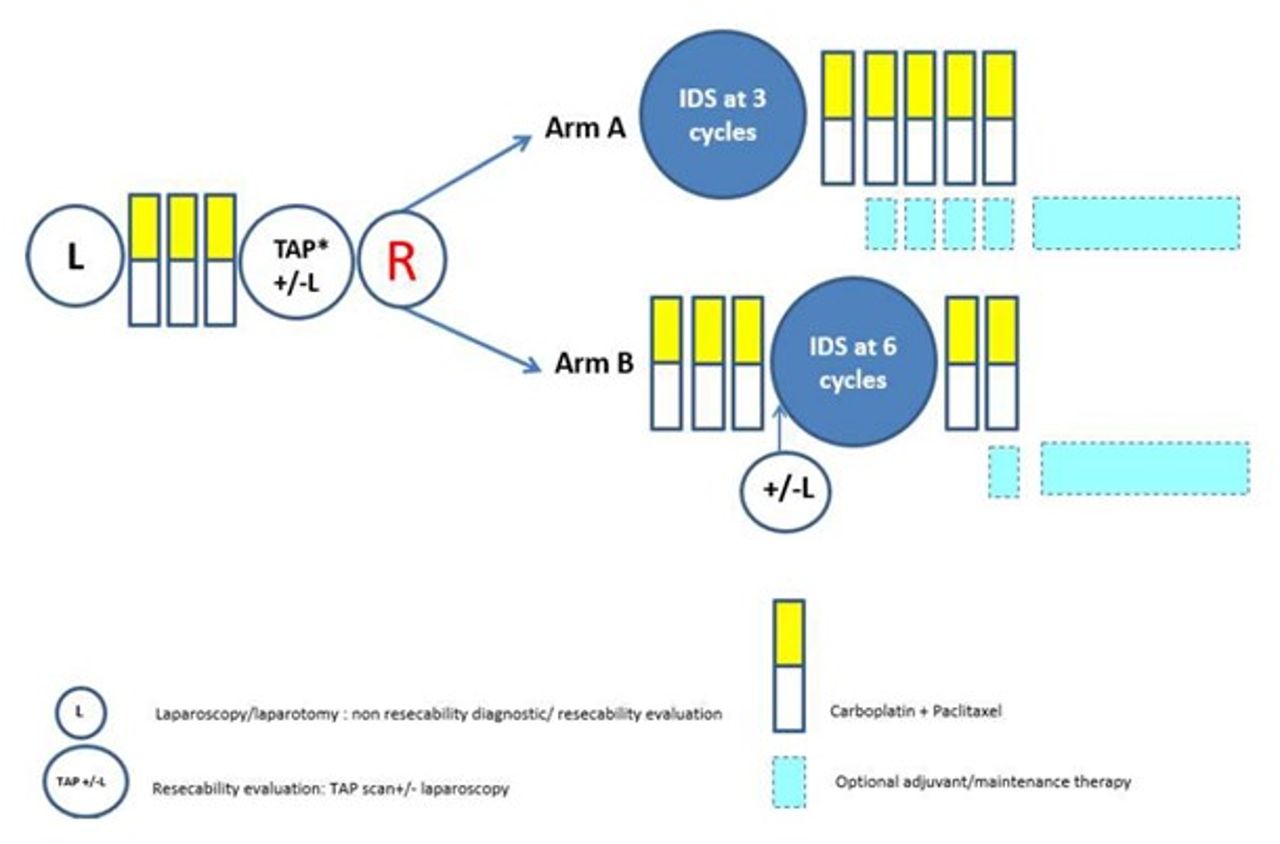
This is a multicenter, ranodmized phase III trial. All patients will be registered on site, and eligible patients will undergo randomization into the following groups: interval surgery (surgery after three courses of neoadjuvant chemotherapy), designed as control arm A, or delayed surgery (surgery after six courses of neoadjuvant chemotherapy), designed as experimental arm B (Figure 1) in a 1:1 ratio. Both randomized groups will be treated with surgery for complete cytoreduction according to current guideline recommendations.1 Complete cytoreduction surgery will be performed by midline laparotomy, or laparoscopy if exploration of the abdominal cavity reveals a peritoneal cancer index of no more than 10 and a residual pelvic mass of no more than 10 cm after the three courses of neoadjuvant chemotherapy. Cytoreductive surgery will include hysterectomy, bilateral salpingo-oophorectomy, omentectomy, as well as peritonectomy, when necessary, and resection of the affected organs—for example, partial resection of the small or large bowel, spleen, pancreas caudal, partial resection of the urinary tract, as well as pelvic and para-aortic lymphadenectomy in the presence of bulky lymph nodes in the analogy of the LION trial.11

{kind=link}
Study scheme of the CHRONO trial. IDS, interval debulking surgery; L, laparoscopy; R, randomization; TAP, CT scan thorax abdomen pelvis.
The treatment received in each arm will be as follows
Control arm A: patients will receive three courses of intravenous carboplatin and paclitaxel every 3 weeks, followed by interval cytoreductive surgery within 6 weeks of the last cycle of chemotherapy. After interval cytoreductive surgery, patients will undergo five more courses of carboplatin and paclitaxel chemotherapy. Interval cytoreductive surgery is defined as cytoreductive surgery after three courses of neoadjuvant chemotherapy .
Experimental arm B: patients will receive six courses of intravenous carboplatin and paclitaxel every 3 weeks, followed by delayed cytoreductive surgery within 6 weeks of the last cycle of chemotherapy. After delayed cytoreductive surgery, patients will undergo two more courses of carboplatin and paclitaxel chemotherapy. Delayed cytoreductive surgery is defined as cytoreductive surgery after six courses of neoadjuvant chemotherapy .
Treatment accepted according to international recommendations:
Paclitaxel at 175 mg/m² + carboplatin area under the curve (AUC) 5–6 every 3 weeks;
Paclitaxel at 60 mg/m² (days 1, 8, and 15), and carboplatin AUC 2 (days 1, 8, and 15) every 3 weeks;
Paclitaxel at dense dose 80 mg/m² (days 1, 8, and 15) and carboplatin AUC 5–6 (day 1) every 3 weeks.
In both groups the total number of courses of chemotherapy will be eight. Hyperthermic intraperitoneal chemotherapy after courses of neoadjuvant chemotherapy is a valid option in the CHRONO trial with respect to the OVHIPEC trial.12 Maintenance/consolidation therapy according to national standard treatments is allowed, such as for example PARP inhibitors or bevacizumab. The setting of the trial is tertiary gynecological cancer centers. Currently, 27 French centers are open for CHRONO trial inclusion of patients and 20 have already started recruiting. The trial is supported by internal resources from the ARCAGY-GINECO cooperative group. The trial was approved by an ethics committee and is registered on the clinicaltrials.gov registry (NCT03579394).
Participants
The main inclusion and exclusion criteria are summarized in Table 1.
Key eligibility criteria
Supplemental material
All patients with histologically confirmed advanced ovarian cancer that is not suitable for complete primary surgery can undergo screening for the CHRONO trial.
Outcomes
The primary study objective is to assess the efficacy on progression-free survival of interval surgery after three courses of neoadjuvant chemotherapy compared with delayed surgery after six courses of neoadjuvant chemotherapy in patients with advanced ovarian cancer. Secondary objectives are health-related quality of life (the EORTC QLQ-C30, QLQ-OV28 questionnaires), pathological complete response rate, overall survival, time to first subsequent treatment, post-operative mortality, post-operative morbidity in accordance with Clavien-Dindo scoring, Fagotti scoring assessment, neoadjuvant therapy, interval surgery and adjuvant therapy tolerance. Ancillary objectives are peritoneal cancer index assessment, completeness of cytoreductive surgery scoring, CA125 evolution during neoadjuvant treatment, vulnerability assessment, laparoscopic interval, or delayed surgery. To monitor patient safety and supervise the progress of the CHRONO trial, an independent data monitoring committee has been established.
Sample Size
For power and sample size calculation, a HR of 0.59 (corresponding to a prolongation of median progression-free survival from 10 months in the interval cytoreductive surgery arm to 17 months in the delayed cytoreductive surgery arm as observed in previous trials). With an assumed accrual period of 2 years, and follow-up of at least 5 years for each patient, we will need 131 events to obtain a power of 85%. We expect that 20% of consented patients will have ineligible stage or histologies found at the time of cytoreductive surgery. In addition, we estimate 2.5% of patients who complete surgery and chemotherapy will be lost to follow-up. With those losses in mind, we estimate we will need to randomize 210 patients.
Randomization and Blinding
After verification of eligibility criteria, patients will be randomized to interval cytoreductive surgery or delayed cytoreductive surgery in a 1:1 proportion (Figure 1). Randomization will automatically be processed using the CS online randomization module. Data of patients will be documented remotely with an electronic data capture system which is hosted in France. Randomization is performed by minimization and stratified by center, screening in internal or external institutions, laparoscopy used or not during baseline screening, laparoscopy or laparotomy used for interval or delayed surgery, the use of hyperthermic intraperitoneal chemotherapy, and treatments received.
Statistical Methods
The aim is to increase median progression-free survival from 10 months (surgery after three courses of neoadjuvant chemotherapy)13 to 17 months (surgery after six courses of neoadjuvant chemotherapy),8 corresponding to a HR of 0.59. With a two-sided type 1 error of 5% and a statistical power of 85% it is necessary to randomize 210 patients and to observe 131 events. The primary endpoint is progression-free survival. Secondary endpoints are overall survival; time until second progression or death; time to first and second subsequent anti-cancer therapies or death; quality of life as measured by the EORTC QLQ-C30, QLQ-OV28, and EQ-5D-3L questionnaires (targeted dimensions: physical functioning and fatigue in the QLQ-C30, abdominal/gastro-intestinal of the QLQ-OV28), and safety. All time-to-event endpoints are calculated from the date of randomization until the event of interest. Stratification will be used to adjust for randomization strata. Additionally, Kaplan-Meier estimates for the distribution of overall survival in each treatment group, a point estimate, and 95% CI of the HR between treatment groups will be given.
DISCUSSION
The optimal number of courses of neoadjuvant chemotherapy before complete surgery in patients with advanced ovarian cancer not suitable for complete primary surgery is still controversial. The CHRONO trial aims to assess the superiority of delayed surgery after six courses of neoadjuvant chemotherapy compared with interval surgery after three courses of neoadjuvant chemotherapy for progression-free survival. In the CHRONO trial, only patients with a clear contraindication for primary surgery are included prospectively. All patients included in the CHRONO trial will be treated with at least three courses of platinum-based neoadjuvant chemotherapy . In order to compare groups with the same number of courses, in the CHRONO trial, all patients are treated with a total number of eight courses of chemotherapy. In series published in the field of delayed surgery after five or six courses of neoadjuvant chemotherapy, two more courses of adjuvant chemotherapy were often proposed.10 Increasing the number of neoadjuvant chemotherapy courses before surgery may improve the effects of neoadjuvant chemotherapy on the efficacy of surgery, with more complete surgery. Considering the impact of the number of courses of neoadjuvant chemotherapy on the rate of complete surgery, published results are conflicting. For Phillips et al,9 the rate of complete surgery decreased in the group treated with five or more courses of neoadjuvant chemotherapy, for Colombo et al,10 it increased in the group of patients receiving more than four courses of neoadjuvant chemotherapy and for Liu et al,14 the rate of complete surgery was not affected by the number of neoadjuvant chemotherapy courses. Increasing the number of neoadjuvant chemotherapy courses before surgery may also improve the results of pathological complete response. It was not studied in the series by Phillips et al or Liu et al.9 14 In the series by Colombo et al, increasing the number of neoadjuvant chemotherapy courses increased the rate of pathological complete response.10 In the CHRONO trial, the completeness of surgery is assessed using the completeness cytoreductive surgery score, and pathological response is assessed using the pathological response score.15
Delaying surgery until after six courses of neoadjuvant chemotherapy may decrease surgical complexity, decreasing the rate of severe post-operative morbidity, and thus improving patients’ quality of life. To our knowledge, the impact of delaying surgery after neoadjuvant chemotherapy on patients’ quality of life has never been studied. Post-operative morbidity and patients’ quality of life are important secondary objectives in the CHRONO trial. Finally, we assume that the CHRONO randomized trial will make possible a clear comparison between performing interval surgery, after three courses of neoadjuvant chemotherapy, or delayed surgery, after six courses of neoadjuvant chemotherapy, in patients treated for advanced ovarian cancer that is not suitable for primary surgery.
Data availability statement
All data relevant to the study are included in the article.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Comité de Protection des PersonnesTOURS - Région Centre - Ouest 1. Participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors J-MC takes responsibility for the integrity of this manuscript. J-MC, AA: study concept, and design. The manuscript has been read and approved by all authors, and all have been involved in drafting the article, critically revising it, and approving its final version. J-MC study supervision. J-MC is the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests J-MC: lectures/other education events from Astra Zeneca, GSK, and Clovis.
Provenance and peer review Commissioned; internally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.