Article Text

Abstract
Objective Because elderly patients with ovarian cancer are underrepresented in randomized studies, this study aimed to expand our knowledge on the safety and effectiveness of frontline treatment with bevacizumab in combination with standard carboplatin and paclitaxel chemotherapy in patients aged 70 years and older with a diagnosis of Federation of Gynecology and Obstetrics (FIGO) stage IV ovarian cancer in routine clinical practice in Belgium.
Methods Patients aged 70 years and older with FIGO stage IV ovarian cancer were included in a multicenter, non-interventional prospective study
to evaluate the safety and effectiveness of treatment with bevacizumab in combination with frontline carboplatin and paclitaxel chemotherapy. Comprehensive geriatric assessments were performed at baseline and during treatment.
Results The most frequently reported adverse events for bevacizumab were hypertension (55%), epistaxis (32%) and proteinuria (21%). The Kaplan-Meier estimate of progression-free survival was 14.5 months. The results of the comprehensive geriatric assessments during treatment indicated a slight improvement in the geriatric eight health status screening tool score for general health status and the mini-nutritional assessment score for nutritional status. The median change from baseline score was close to zero for the instruments measuring independency, activity of daily living and instrumental activities of daily living, and for the mobility-tiredness test measuring self-perceived fatigue.
Conclusions No new safety signals were registered in this study in patients aged 70 years and older treated with bevacizumab and frontline carboplatin and paclitaxel for FIGO stage IV ovarian cancer. Elderly patients should not be excluded from treatment for advanced ovarian cancer based on age alone.
EU PAS register ENCEPP/SDPP/13849.
ClinicalTrials.gov identifier NCT02393898.
- ovarian cancer
Data availability statement
Data are available upon reasonable request.
Statistics from Altmetric.com
HIGHLIGHTS
Elderly patients with ovarian cancer are underrepresented in randomized studies.
No new safety signals were reported in this study in elderly patients treated with bevacizumab and chemotherapy.
Extensive geriatric assessment showed favorable tolerability of the treatment in this population.
Introduction
Ovarian cancer is the fifth leading cause of death from cancer in European and Belgian women.1 2 In Belgium, 25% of ovarian cancers are International Federation of Gynecology and Obstetrics (FIGO) stage IV at diagnosis3 4 and 46% of patients with newly diagnosed ovarian cancer are aged 70 years or older.5 Five-year survival in this group of patients is only 30%.3 The progression-free survival benefit of adding the antiangiogenic agent bevacizumab to frontline carboplatin and paclitaxel chemotherapy has been investigated in two large, randomized phase III studies, GOG-0218 and ICON7.6 7
Patients aged 70 years and older were underrepresented in both studies: 17% in GOG-0218 and 10% in ICON7. Subgroup analysis of GOG-0218 and ICON7 showed similar progression-free survival benefit in patients aged 70 years and older compared with the entire study population. However, for GOG-0218 and ICON7, no specific safety results in the subgroup of elderly patients were reported.6 7 Age-related physiological changes after the age of 70 increase the risk of toxicity with systemic cancer therapy and the age of 70 is widely accepted as a cut-off for ‘older’ specific analyses.8 Data on the safety outcomes of frontline chemotherapy for ovarian cancer in elderly patients are scarce, making treatment decisions challenging. Comprehensive geriatric assessment provides an overview of the general health status of older individuals and determines the functional and physiological age.9 The International Society of Geriatric Oncology 2014 task force recommended evaluating the following domains: functional status, comorbidity, cognition, mental health status, fatigue, social status and support, nutrition, and presence of geriatric syndromes.10
This national, multicenter, non-interventional, prospective study aimed to expand knowledge on the safety and effectiveness of frontline treatment with bevacizumab in combination with standard carboplatin and paclitaxel chemotherapy in patients aged 70 years and older with a diagnosis of FIGO stage IV epithelial ovarian, fallopian tube or primary peritoneal cancer in routine clinical practice in Belgium. We restricted this study to patients with FIGO stage IV ovarian cancer because in Belgium bevacizumab is only reimbursed for stage IV disease. Study-specific data were collected using comprehensive geriatric assessment.
Methods
Participants
Patients aged 70 years and older with an initial diagnosis of FIGO stage IV epithelial ovarian, fallopian tube or primary peritoneal cancer for whom it was decided to administer frontline bevacizumab with carboplatin and paclitaxel chemotherapy according to the European Union bevacizumab label11 could be included in this real world study in Belgium.
Study Design
BGOG-ov16/BELOVA is a prospective, single-arm, national, multicenter, non-interventional, post-authorization study that collected safety and effectiveness data in routine clinical practice. Patients were followed from the start of bevacizumab treatment until progression or death. No study-specific visits were required in the protocol. Data were collected during treatment at regular visits according to routine clinical practice and during follow-up at 6 and 12 months after the end of bevacizumab administration. Study-specific data were collected using comprehensive geriatric assessment at baseline and limited comprehensive geriatric assessment during treatment to assess the evolution over time. The recruitment period of the study was from April 2015 to July 2019.
Treatment
Dosing and treatment duration of bevacizumab and chemotherapy were at the discretion of the investigator, in accordance with local labeling and criteria for bevacizumab reimbursement.11 12 The recommended dose of bevacizumab is 15 mg/kg every 3 weeks in addition to carboplatin and paclitaxel for up to six cycles followed by continued use as single agent for a maximum of 15 months.11
Data Collection
The primary endpoint of the study was safety and tolerability in routine clinical practice of bevacizumab in combination with standard carboplatin and paclitaxel chemotherapy in elderly patients. At baseline, key demographic characteristics and medical history were recorded. Patients with at least one administration of bevacizumab were included in the safety population. During treatment, all adverse events were collected at routine clinical visits. Adverse events occurring until at least 28 days after the last administration of bevacizumab were considered as treatment-emergent adverse events. During follow-up, patients were actively monitored for serious adverse events and adverse events of special interest until at least 6 months after the last administration of bevacizumab.
The adverse events of special interest for bevacizumab were defined as cases of potential medicine-induced liver injury, suspected transmission of an infectious agent by the study medicine, hypertension, proteinuria, gastrointestinal perforation, wound healing complications, arterial or venous thromboembolic events, bleeding, congestive heart failure, fistulae and reversible posterior leukoencephalopathy syndrome. Severity was graded using the National Cancer Institute Common Terminology Criteria for Adverse Events v4.0 in oncology studies.13
Study-specific data collection was comprehensive geriatric assessment at baseline and limited comprehensive geriatric assessment during treatment and follow-up at months 3, 6, 10, 12, 15, 18, 24, 36 and 48. The comprehensive geriatric assessment at baseline consisted of different evaluation instruments (Online supplemental table 1). General health status and identification of a geriatric risk profile were assessed by the geriatric eight health status screening tool questionnaire (score from 0 to 17, ≤14 abnormal) and the geriatric risk profile questionnaire (out of 6, ≥1 geriatric risk). Pain was evaluated with a pain visual analog scale from 0 to 10 (0 no pain, 1– 3 mild pain, >3 pain to treat). Functional status was assessed with the activity of daily living (total scores from 6 to 24, ≥7 dependent), the instrumental activities of daily living (for women out of 8, <8 dependent), the falls question (yes/no), and falls related injury (yes/no). Self-perceived fatigue was measured with the mobility-tiredness test (from 0 to 10, ≥3 tired). Cognition was assessed with the mini-mental state examination (out of 30, 23–18 mild cognitive decline, ≤17 severe cognitive decline). Mood was evaluated with the 15-item geriatric depression scale (0–15, ≥5 at risk for depression). Nutritional status was assessed with the mini-nutritional assessment (out of 30, 23–17 at risk for malnutrition, <17 malnourished). The Charlson comorbidity index assesses comorbidity level by considering both the number and severity of 19 predefined comorbid conditions (no comorbidities=0; presence of comorbidities≥1). Patients were scored for the Eastern Cooperative Oncology Group (ECOG) performance status (out of 5).14–16 Limited comprehensive geriatric assessment included the geriatric eight health status screening tool, pain visual analog scale, activity of daily living, instrumental activities of daily living, mobility-tiredness test and mini-nutritional assessment questionnaires.
Supplemental material
Disease progression was assessed according to routine clinical practice in every center, radiographic assessment through Response Evaluation Criteria in Solid Tumors.17 Progression-free survival was defined as time from start of bevacizumab treatment until progression or death from any cause, whichever came first. Overall survival was defined as time from start of bevacizumab treatment until death from any cause.
Statistical Methods
Descriptive statistical methods were used to analyze the results of this single-arm study. Sample size was not based on a formal calculation but driven by feasibility. To limit potential bias, centers were selected based on their experience in treating elderly patients with ovarian cancer, Belgium and Luxembourg Gynecological Oncology Group membership, experience with bevacizumab for this indication, and the availability of site personnel to perform comprehensive geriatric assessment.
Ethical Considerations
The study was conducted in full conformance with the Guidelines for Good Pharmacoepidemiology Practices published by the International Society of Pharmacoepidemiology and Belgium laws and regulations. The study complied with national and European Union requirements for ensuring the well-being and rights of participants in non-interventional post-authorization safety studies. The study was reviewed by the Central Belgian Ethics Committee of the Catholic University of Leuven and by the Local Ethics Committees of the participating centers. All patients gave informed consent before enrolment in the study. The Scientific Committee of the study with members of the Belgium and Luxembourg Gynecological Oncology Group was involved in the development of the protocol, design of the study, analysis and disclosing of the results to maintain ethical and scientific standards. The study was performed according to the European Network of Gynecological Oncological Trial Groups Model C.18
Results
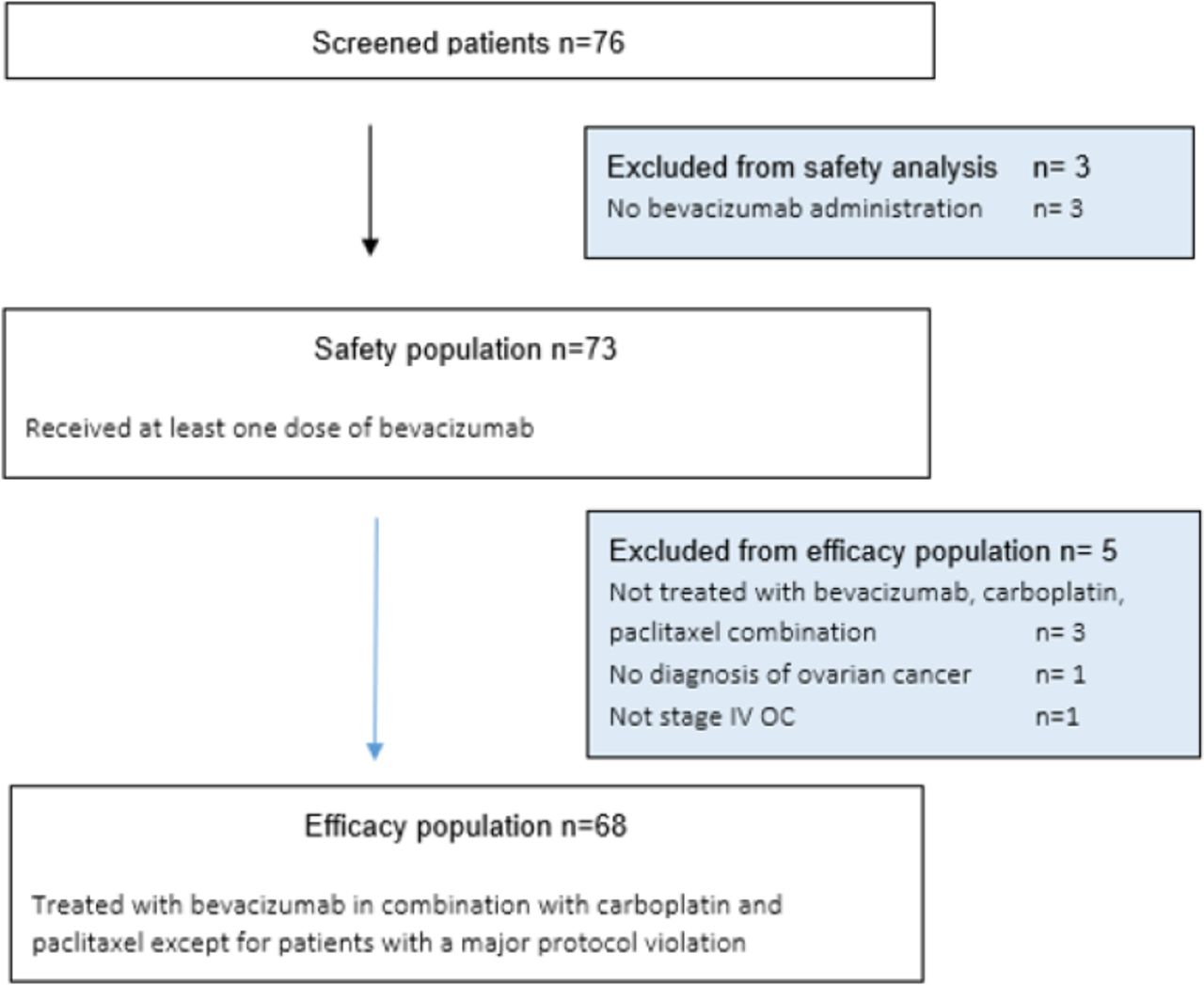
Seventy-six patients were considered for enrollment. Seventy-three patients received at least one bevacizumab administration and were included in the safety population. Five patients with major protocol violations were excluded from the efficacy population (Figure 1).

{kind=link}
Patient CONSORT diagram. OC, ovarian cancer.
Baseline Results
Baseline results in the safety population are presented in Table 1. The age of patients at inclusion ranged from 70 to 88 years and mean age was 76 years. Median geriatric risk profile questionnaire score was 1 (IQR (Q1–Q3) 1–2) and median geriatric eight health status screening tool score was 11 (IQR 9–13), suggesting that most patients had a geriatric risk profile. At least half of the patients were independent regarding basic self-care tasks as suggested by the median activity of daily living score of 6 (IQR 6–7). For more complex tasks, at least 75% of patients were dependent as indicated by the median instrumental activities of daily living score of 7 (IQR 5–8). Median mini-mental state examination score of 28 (IQR 27–29) indicates that cognition was normal in more than 75% of patients. Most patients were not at risk of depression as indicated by the median 15-item geriatric depression scale score of 3 (IQR 2–5) but felt tired as shown by the median mobility-tiredness test score of 5 (IQR 3–6). Most patients were at risk of malnutrition as reflected by the median total mini-nutritional assessment score of 22 (IQR 20–26). Median Charlson comorbidity index was 1 (IQR 0–2) and the most common comorbidity was hypertension reported in 40/73 (55%) of patients at baseline.
Baseline characteristics of safety population. Data are numbers (%) unless indicated otherwise
Safety
During treatment, 71 out of 73 patients (97%) reported at least one adverse event. Table 2 shows the adverse events reported in more than 15% of patients. At least one adverse event related to bevacizumab was reported in 60 (82%) patients and at least one adverse event related to chemotherapy in 61 (84%) patients. During treatment at least one serious adverse event was reported in 36 (49%) patients; in 16 (22%) patients the serious adverse event was considered to be related to bevacizumab and in 17 (23%) related to chemotherapy.
Adverse events in safety population. Data are numbers (%) unless indicated otherwise
There were three deaths due to an adverse event; none of these events were considered to be related to treatment. One patient died of cachexia, one patient of bowel obstruction and cardiac arrest, and one patient following cardiac arrest. At least one adverse event for bevacizumab was reported in 58 (80%) patients. The adverse events for bevacizumab reported in more than 15% of patients were hypertension (55%), epistaxis (32%) and proteinuria (21%) (Table 2). Serious adverse events observed in 14 (19%) patients are presented in Online supplemental table 2.
In 17 (23%) patients, at least one adverse event was reported during the 6-month follow-up after the last administration of bevacizumab. In six patients the adverse event was serious. One fatal small bowel perforation occurring at least 28 days after the last bevacizumab administration was related to bevacizumab (Table 2). Forty-seven patients (64%) did not complete bevacizumab treatment (Online supplemental table 3). In 20 patients, treatment discontinuation was due to the decision of the physician. In six patients treatment discontinuation was due to an adverse event, and in four patients due to a serious adverse event. Adverse events leading to bevacizumab interruption were hypertension in four patients, gastrointestinal bleeding in one patient, and posterior reversible leukoencephalopathy syndrome in one patient. Serious adverse events leading to bevacizumab treatment interruption were two bleeding events (epistaxis and stomach hemangioma), one gastrointestinal perforation, and one pleural effusion. Twelve patients (16%) did not complete carboplatin treatment and 14 (19%) discontinued paclitaxel treatment (Online supplemental table 3). For 68 patients included in the efficacy population, median bevacizumab treatment duration was 9.3 months and median treatment duration of chemotherapy was 5.1 months. At the time the study was terminated, two patients were still treated with bevacizumab. Consequently, the follow-up of these patients was terminated prematurely.
Comprehensive Geriatric Assessment
From 69 patients with comprehensive geriatric assessment results at baseline, the number of patients with post-baseline results for the limited comprehensive geriatric assessment is variable, from 33 patients at month 10 to two patients at month 18, or five patients at month 12. For the geriatric eight health status screening tool score, most patients with available data showed an increase in score that suggested a slight improvement in their health status. Most patients also showed an increase in total mini-nutritional assessment score, indicating an improvement of their nutritional status. Median change from baseline scores remained close to zero for the activity of daily living, instrumental activities of daily living, and mobility-tiredness test at all time points, suggesting no change in independency or tiredness during treatment (Online supplemental figure 1, Online supplemental table 4).
Survival
The Kaplan-Meier estimated median progression-free survival from first bevacizumab administration was 14.5 months in the efficacy population (Online supplemental figure 2). The follow-up of patients was too immature to estimate overall survival.
Discussion
Summary of Main Results
The BGOG-ov16/BELOVA study is a prospective study evaluating the safety and effectiveness in routine clinical practice of bevacizumab added to frontline standard chemotherapy of advanced ovarian cancer in women aged 70 years and older. Baseline hypertension was present in 55% of patients. During treatment, a higher proportion of all grade hypertension (55%), grade ≥3 hypertension (33%) and all grade proteinuria (21%) was reported compared with the safety results of the phase III studies.6 7 All other safety outcomes or adverse events of special interest, such as all grade fistula (3%), gastrointestinal perforation (3%), wound healing complications (1%), deep venous thrombosis (4%), bleeding (37%) or posterior reversible encephalopathy (1%), are in line with the safety profile observed in the two phase III studies.6 7 In the BGOG-ov16/BELOVA study including only patients aged 70 years and older, the Kaplan-Meier estimate for progression-free survival was 14.5 months, within the expectations for FIGO stage IV ovarian cancer in the general population.
Results in the Context of Published Literature
The results of two large phase three studies, GOG-0218 and ICON7, indicate that the addition of bevacizumab to frontline standard chemotherapy increases the progression-free survival in advanced ovarian cancer.6 7 However, patients aged 70 years and older were underrepresented in these pivotal phase III studies. There is no specific clinical research to guide the complex treatment decisions for this important group of patients. The scarcity of data might lead to undertreatment of older women. In a French retrospective, multicenter, observational study, women aged 75 years and older were treated less often with bevacizumab compared with women aged 70–74 years (8.9% vs 31.5%, p=0.003).19 Subgroup analysis in elderly patients of GOG-0218 and ICON7 showed similar progression-free survival benefit in woman aged 70 years and older compared with the overall study population when bevacizumab was added to carboplatin and paclitaxel chemotherapy.6 7 In the German non-interventional real-world OTILIA study in primary ovarian cancer with 40% of patients aged 70 years and older, age was not a significant prognostic factor for progression-free survival.20 The single-arm ROSiA study explored extended duration of frontline bevacizumab-containing therapy for ovarian cancer and included 12% of patients aged 70 years and older. Post-hoc analysis to explore efficacy according to age showed no striking difference between patients aged 70 years and older and younger patients, despite the worse prognosis in elderly patients.21
No specific safety analyses were done in GOG-0218 and ICON7 for the subgroup of elderly patients.6 7 In OTILIA, more patients aged 70 years and older compared with those younger than 70 years had comorbidities at baseline (73% vs 57%), mainly driven by the higher proportion of elderly patients with hypertension (54% vs 31%). Exploratory analysis of OTILIA showed no evidence that age is associated with worse safety outcome during treatment with bevacizumab combined with carboplatin and paclitaxel chemotherapy.20
In the single-arm ROSiA study, baseline hypertension was observed in 70% of patients aged 70 years and older compared with 28% in patients younger than 70 years. During extended frontline bevacizumab-containing therapy, the incidence of asthenia, low-grade diarrhea, anemia, grade ≥3 hypertension (41% vs 22%) and thromboembolic events (14% vs 6%) were higher in patients aged 70 years and older than in those younger than 70 years.21
Strengths and Weaknesses
The comprehensive geriatric assessment scores did not deteriorate during treatment. However, due to the very low proportion of patients with available data after baseline, comprehensive geriatric assessment results should be judged with caution. Although most patients were at geriatric risk and 17% of patients had ECOG ≥2 at baseline, selection bias to include the more fit patients with ovarian cancer in this real-world study cannot be excluded. The absence of a control arm is an additional limitation.
Implications for Practice and Future Research
WHO defines elderly patients as those aged 65 and older and oldest-old as those aged 80 and older.22 The term elderly is culture specific, and aging is a heterogenic process.22 Chronological age is a poor marker of the health impact of aging.23 The European Organization for Research and Treatment, the International Society of Geriatric Oncology, the Alliance for Clinical Trials in Oncology, the American Society of Clinical Oncology, and the Cancer and Leukemia Group B all recommend the integration of comprehensive geriatric assessment in future studies.24–27 At the time of the GOG-02186 and ICON77 publications, implementation of comprehensive geriatric assessment in clinical trial design was unusual. In the current study the comprehensive geriatric assessment performed at baseline indicated a geriatric risk profile and a risk for malnutrition in most patients with first-line ovarian cancer. Results of this real-life prospective study in women aged 70 years and older adds knowledge to the growing evidence that elderly patients should not be excluded from bevacizumab as frontline treatment for advanced ovarian cancer based on age only.
Conclusions
The results of the current study confirm the safety and tolerability of bevacizumab in frontline treatment of advanced ovarian cancer in patients aged 70 years and older. No new major safety signals were recorded during this real-world study in this specific population. Safety and effectiveness outcomes suggest that the large group of elderly patients can be safely treated with bevacizumab for advanced ovarian cancer.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was was reviewed by the Central Belgian Ethics Committee of the Catholic University of Leuven and by the Local Ethics Committees of the participating centres. EU PAS Register: ENCEPP/SDPP/13849; ClinicalTrials.gov Identifier: NCT02393898. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We would like to thank all the patients, their families, doctors, and nurses who participated in the BGOG-ov16/BELOVA study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @CVulsteke
Contributors IV, HD, CG, TvG, EVN, DV, and PV are members of the Scientific Committee of the study and were involved in the development of the protocol, design of the study, analysis and disclosing of the results and maintaining ethical and scientific standards. All authors critically revised the manuscript and approved the version to be published. All authors agree to be accountable for all the aspects of the publication of the study results. IV is responsible for the overall content as guarantor.
Funding This work was supported by F. Hoffmann-La Roche Ltd.
Competing interests IV reports consulting: for Agenus (2021), Aksebio (2021), Amgen (Europe) GmbH (2019), AstraZeneca (2019-2022), Bristol Myers Squibb (2021), Clovis Oncology Inc. (2019-2019), Carrick Therapeutics (2019), Deciphera Pharmaceuticals (2020-2021), Eisai (2021), Elevar Therapeutics (2020), F. Hoffmann-La Roche Ltd (2019-2021), Genmab (2019-2021), GSK (2019-2021), Immunogen Inc. (2019-2022), Jazzpharma (2021-2022), Karyopharm (2021), Mersana (2020), Millennium Pharmaceuticals (2019), MSD (2019-2022), Novocure (2020-2022), Novartis (2021), Octimet Oncology NV (2019), Oncoinvent AS (2019-2022), Seagen (2021), Sotio a.s. (2019-2022), Verastem Oncology (2020), Zentalis (2020); Contracted Research (via KU Leuven) from Oncoinvent AS (2019-2020) and Genmab (2019); Grant or corporate sponsored research from Amgen (2019-2020) and Roche (2019); Accomodations, travel expenses (2019-2020) from Amgen, MSD, Tesaro, AstraZeneca and Roche. CV reports for the present publication study funding from Roche and support from Lutgart Opstaele from ANZ Medical Writing; Institutional Grant from MSD/Merck, Consultancy for Janssen-Cilag, Roche, GSK, Atheneum Partners, Astellas Pharma, MSD, BMS and Leo-Pharma, Presentation and advisory Boards: Janssens Cilag, Leo Pharma, Presentation: Bayer; Advisory Board: Merck MSD, GSK, Astrazeneca; Travel support from Roche and Pfizer. PV reports for the present publication support from Roche (medical writing and article processing charges; consulting fees from Astrazeneca and Roche, Participation on a data safety monitoring board or advisory board: Astrazeneca and Roche; unpaid leadership or fiduciary role: BSMO president 2019. MVS is employee of Roche NV. All other authors declared no conflicts of interest.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.