Article Text

Statistics from Altmetric.com
Summary
Radical hysterectomy is the gold standard to treat early stage cervical cancer. Recently published studies have shown that minimally invasive surgery might have lower survival rates than classic open surgery.1 In their trial, the authors compared minimally invasive surgery (laparoscopy and robot assisted surgery) with open surgery, but they did not use the classical vaginal approach first described by Schuchardt in 1893 and further developed by Schauta in 1902, and improved by others over time.2 Current studies have performed this approach to avoid the use of a uterine manipulator, which with routine use might increase the propensity for tumor spillage, according to some trials.1 3
There are three variations of the Schauta approach: Schauta–Amreich, Schauta–Stoeckel, and Coelio–Schauta or laparoscopically assisted radical vaginal hysterectomy,2 recently described by Torné et al,4 demonstrating high disease free survival and overall survival in a retrospective cohort of patients with early stage cervical cancer.
Our video shows the performance of a modification of the technique, combining the full Schauta operation with endoscopic lymphadenectomy, published in 1995 by Dargent et al.2
{kind=link}
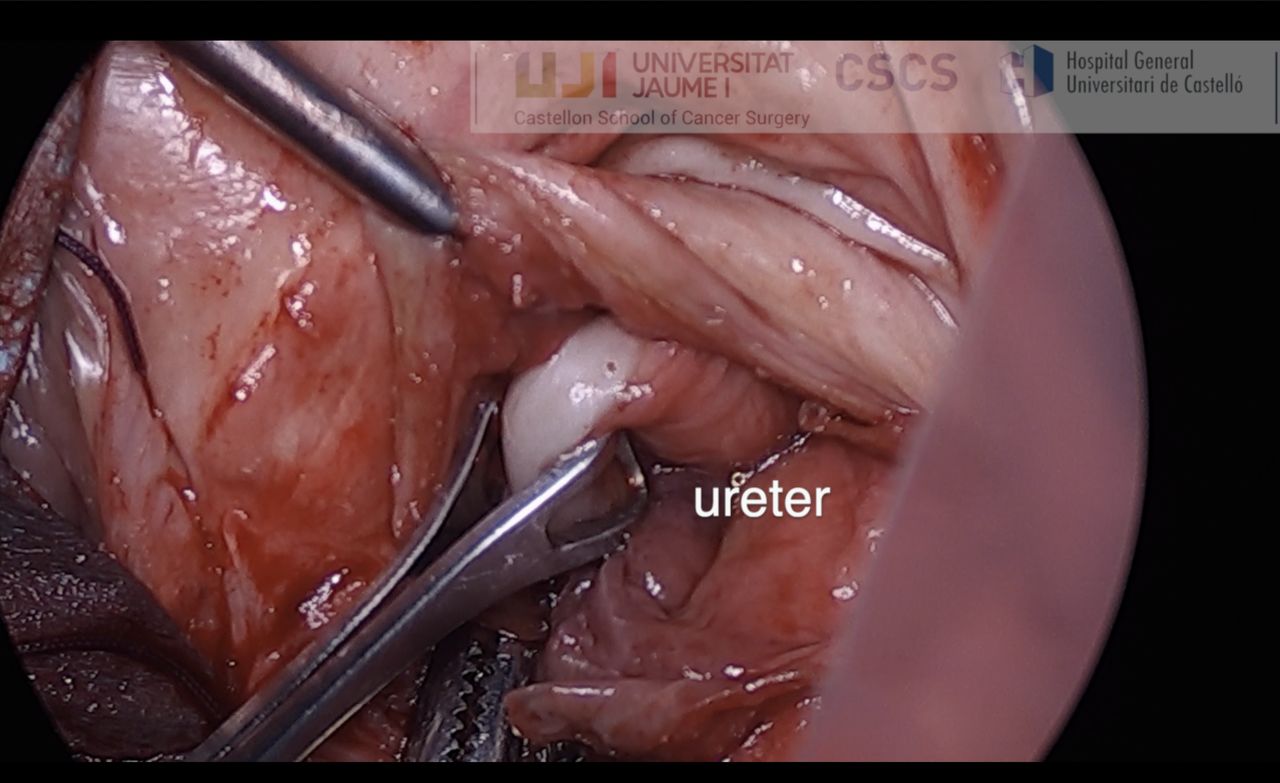
Identification of the ureter: after dissection of the bladder pillar, we can reference the ureters with Babcock forceps to mobilize them cranially to avoid injuries.
Data availability statement
There are no data in this work.
Ethics statements
Patient consent for publication
Footnotes
Twitter @annaserrix
Contributors ASR: conception and design, writing of the manuscript, and video editing. ALA and MTC: acquisition of the data and revision of the manuscript for important intellectual content.
Funding This study was funded by Medtronic University Chair for Training and Surgical Research, University Jaume I (UJI), Castellón, Spain.
Competing interests The authors declare no competing interests.
Provenance and peer review Not commissioned; externally peer reviewed.