Article Text

Abstract
Introduction/Background The Peritoneal Carcinomatosis Index (PCI) and the Intra-operative Mapping for Ovarian cancer (IMO) to a lesser extent have been universally validated in advanced-stage epithelial ovarian cancer (EOC) to describe the extent of peritoneal dissemination and proven powerful predictors of the surgical outcome with an added sensitivity of assessment at laparotomy around 70%. This leaves room for improvement because the two-dimensional anatomic model for scoring fails to reflect the patient’s real anatomy, as seen by the surgeon.
Methodology We analyzed prospectively collected data from 508 patients with FIGO stage IIIB to IVB EOC who underwent cytoreductive surgery between January 2014 and December 2019 in a UK tertiary center. We adapted the structured ESGO ovarian cancer report to provide detailed information on the patterns of tumor dissemination (cancer anatomic fingerprints). We applied the Shapley Additive Explanations (SHAP) framework to support the feature selection of the narrated cancer fingerprints. We employed the eXtreme Gradient Boost (XGBoost) to model only variables referring to the tumor disseminated patterns, to create an intra-operative score, and to judge the predictive power of the score alone for complete cytoreduction (CC0). Receiver operating characteristic (ROC) curves were then used for performance comparison between the new score, and the existing PCI and IMO tools.
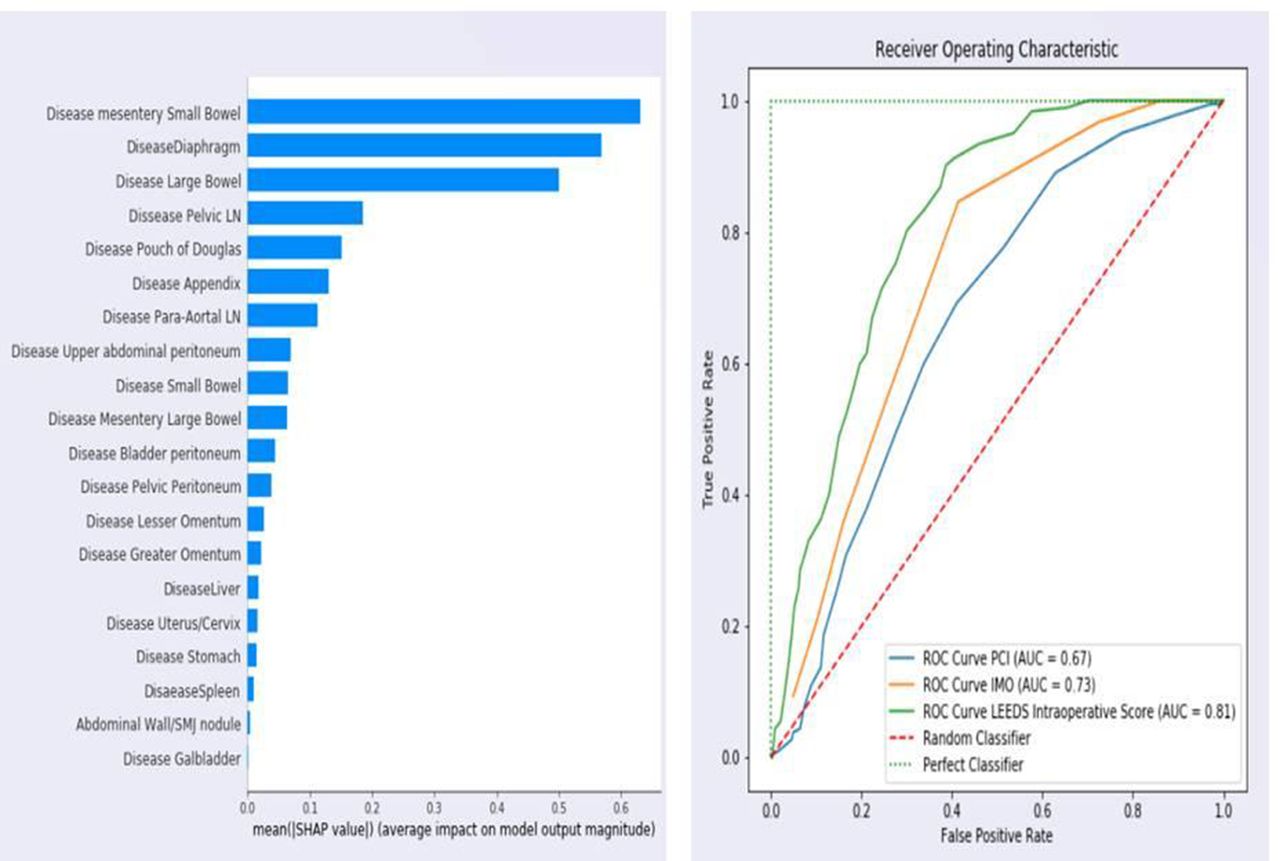
Results An intra-operative disease score was created based on specific weights allocated to the cancer anatomic fingerprints (figure 1a). The score ranged from 0 to 39. The new score was not inferior to PCI and IMO for the prediction of CC0 (AUC: 0.81 vs 0.73 vs 0.67, p: NS) (figure 1b).

{kind=link}
Conclusion The presence of cancer dissemination collectively in specific anatomical sites, including small bowel mesentery, diaphragmatic peritoneum, and large bowel may be more predictive of CC0 than the entire PCI and IMO. Early intra-operative assessment of these areas may reveal whether CC0 is achievable.