Article Text

Abstract
Introduction/Background*The tumour microenvironment (TME) in metastatic high grade serous ovarian cancer (HGSOC) is not well described. We present a multimodal characterisation of intraepitelial TILs (iTILS) and stromal TILs (sTILS) using flow cytometry (FACS) immunohistochemistry (IHC) in matched primary and metastatic HGSOC samples.
Methodology FACs and IHC for CD4 and CD8 were performed on 26 samples from seven women with HGSOC. Tissue samples, labelled with fluorescent antibodies against CD3, CD4, CD8, checkpoints TIGIT, PD1 and cytokine IFN-γ also were analysed with a FACS Fortessa (BD Biosciences). IHC was performed on samples and images annotated to assess intra-epithelial and stromal CD4 and CD8 expression using ImageScope (Aperio), and analysed using the Aperio Nuclear Algorithm v9 (figure 1). Statistical analysis was performed using IBM SPSS 24 or Prism Graph Pad. Quantitative variables were assessed with one way ANOVA and Mann Whitney test.
Result(s)*FACs demonstrated that, compared to primary samples, the frequency of CD8+ TILs(p= 0.017) , TIGIT (p=0.013) and PD1 (p=0.017) expression was reduced in matched metastatic sites. CD4+ TILs levels were unchanged between primary and metastatic samples. Consistent with a reduced level of cytotoxic activity, IFN-γ on CD8+ TILs was reduced in the metastatic TME (p=0.034).
IHC demonstrated that the majority of primary samples (5/7 (71.4%) showed a higher proportion of CD8+ sTILs compared to iTILs (figure 3b). In the one BRCA mutated patient, the CD8 iTILs were higher than sTILs (figure 4a). In FACs, this sample also had the highest frequency of CD8+ TILs within the ovarian tumour (figure 4b).
In IHC from 4/6 different metastatic sites (omentum, vagina, spleen and peritoneum) the density of CD8+ sTILs was higher than iTILs, demonstrating these tumours were immune excluded. Serosal liver and diaphragmatic metastases demonstrated increased CD8+ iTILs compared with primary tumours. Although not as marked, this pattern was replicated in CD4 sTILs (figure 5b, c).

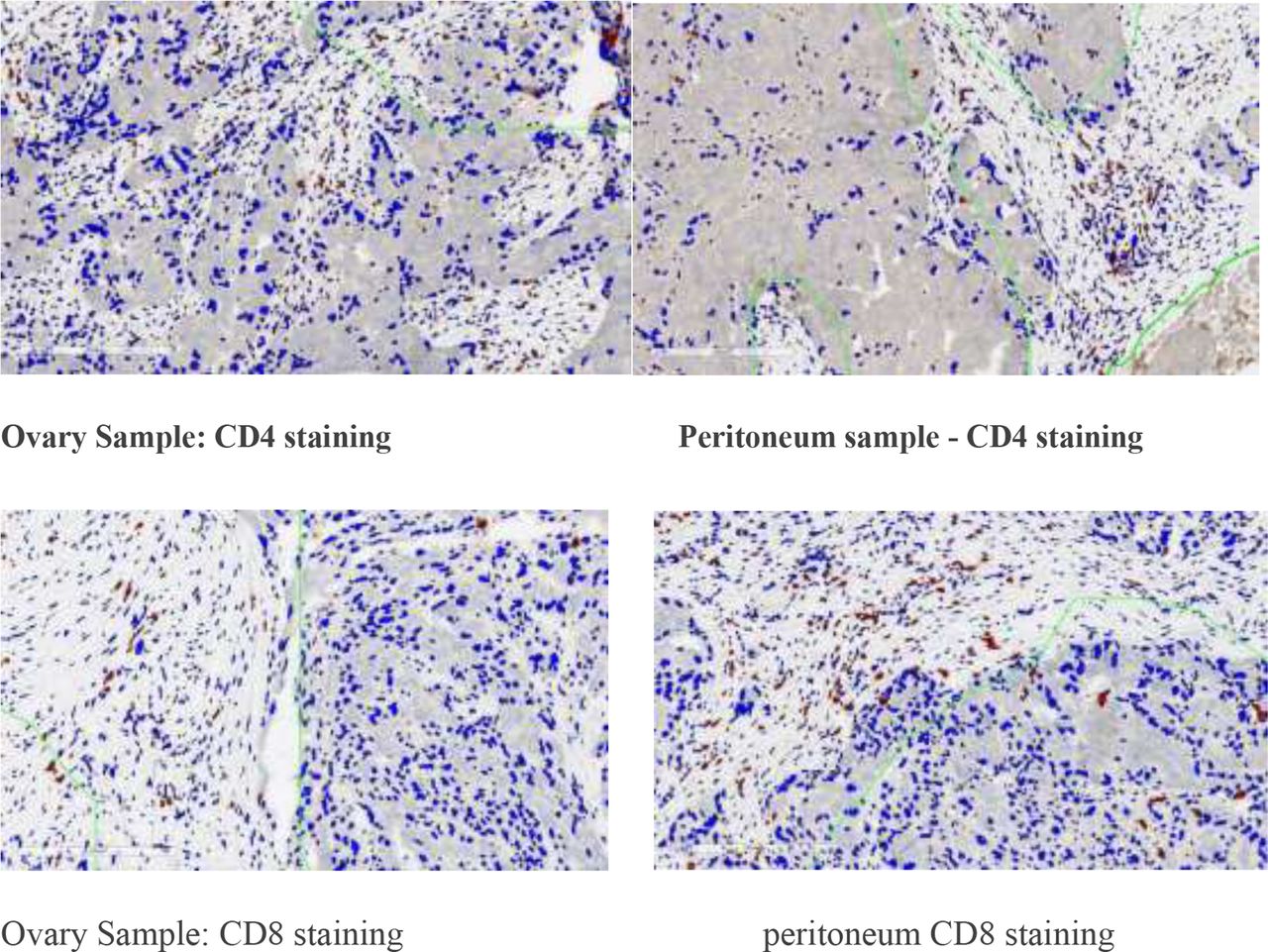
Immunohistochemistry of primary ovarian HGSOC stained for CD4 and CD8 Demonstration of presence of CD4+ and CD8+ TILS in stroma and ovarian tissue. TIL expression was calculated as the number of cells/mm2
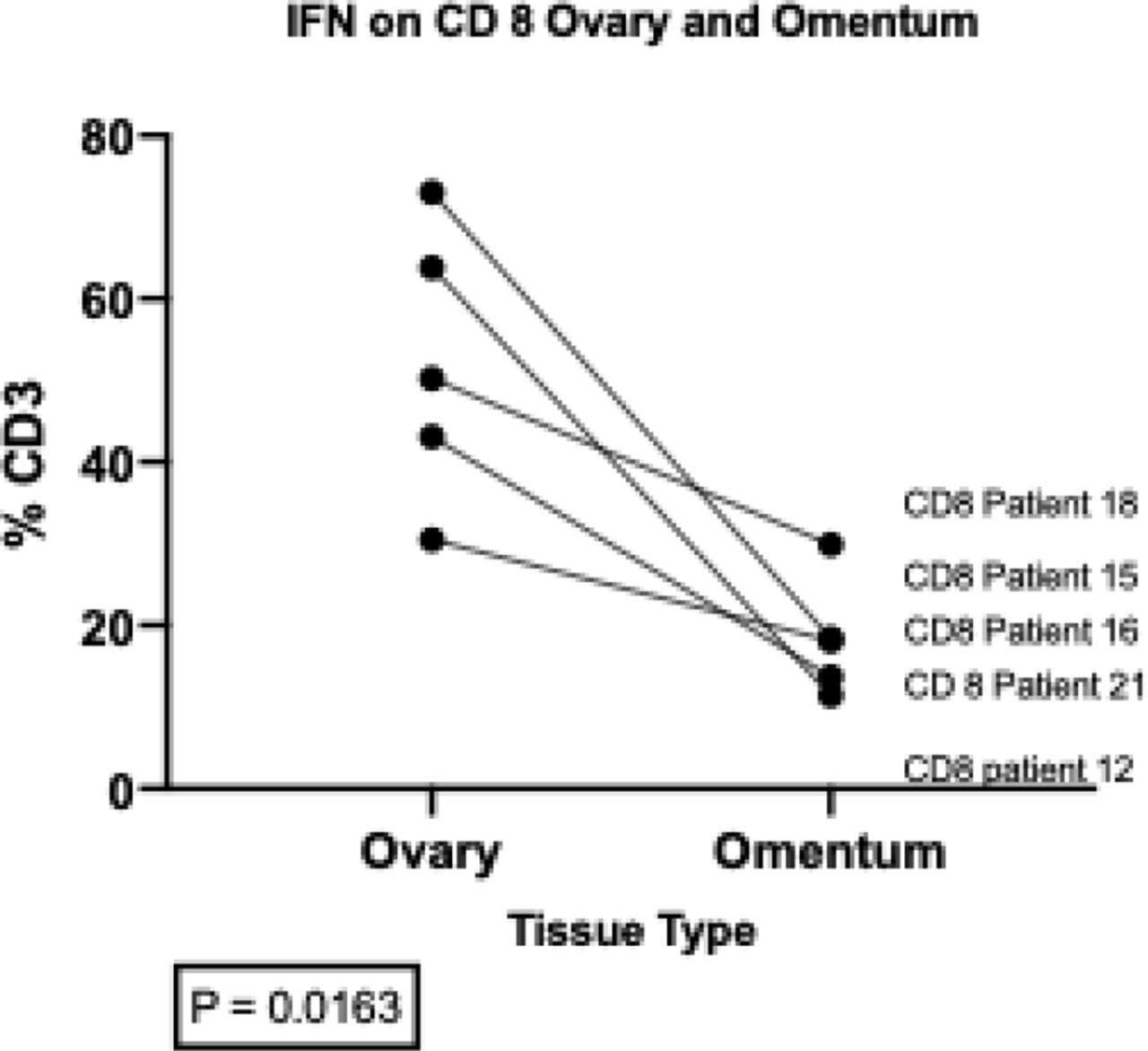
Flow cytometry IFN-γ expression in Primary ovary and metastatic samples
Fig 2a FACs analysis of IFNg expression on CD8+ T cells from primary HGSOC samples in primary ovary, metastatic omental samples. This graph demonstrates that the proportion of IFNg decreases in CD8+ T cells on metastatic T cells when compared to primary ovarian samples

Immunohistochemistry results of CD4+ T cells and CD8+ TILs in ovarian tumour and stroma
3a This graph shows that in 5/7 (71.4%) of ovarian tumour samples the number of cells per mm2 of CD4+ T cells was increased in the surrounding stroma compared to the tumour itself. The black dots represent those patients in whom the tumor showed a lower number of CD4+ T cells per mm2; 3b This graph shows in 5/7 (71.4%) of patients the number of cells per mm2 of CD8+ TILs was greater in the stroma. Therefore these tumours could be considered ‘cold’ or ‘immune excluded’

BRAC status and IHC
4b: Flow cytometry from primary ovarian cancer tissue samples; 4a BRCA mutation was known in three patients. One (1/3, 33.3%) was BRCA1 mutated (p16) and this patient sample showed an increased proportion of CD8+ TILs in the tumour compared to the surrounding stromal tissue4b Flow cytometry: This demonstrates the levels of CD8+ T cells within the primary ovarian tumour from our patient cohort. The BRCA1 mutation on P16 showed the highest number of CD8+ T cells, correlating with the IHC data.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Immunohistochemistry of CD4+ and CD8+ TILs in tumour and stroma HGSOC primary samples
5a Immunohistochemistry reveals the number of CD4+ and CD8+ T cells per mm2 within the ovarian tumour. A higher proportion of CD8+ TILs was noted within the tumour tissue; Fig 5b A representation of the CD4+ T cells in the HGSOC metastatic samples. For metastatic samples in the omentum(3/5) vagina, spleen and peritoneum, the stroma had a greater proportion of CD4+ T cells than the tumour. In the diaphragm and in serosal liver deposits, the tumour was enriched with CD4+ T cells. The difference was less marked than in the CD8+ TILs (see fig 5c); 5c A representation of the CD8+ TILs in the HGSOC metastatic samples. For the majority of metastatic samples, the presences of CD8+ TILs in the metastatic cancer samples was lower in the tumour sample than within the stromal tissue
Conclusion*Using a multimodal approach, including IHC and FACs, we demonstrate that the metastatic TME in HGSOC is significantly different to the primary TME. These findings provide an initial explanation as to why immune checkpoint inhibitors have failed in HGSOC and warrant further investigation.