Article Text

Statistics from Altmetric.com
Serous endometrial cancer represents a relatively rare entity, accounting for about 10% of all diagnosed endometrial cancer, but it is responsible for 40% of endometrial cancer-related deaths. Patients with serous endometrial cancer have a higher risk of recurrence and poorer prognosis when compared stage-for-stage with endometrioid endometrial cancer. Serous endometrial cancer shows an aggressive behavior and shares most of its molecular features with high-grade serous ovarian cancer, such as the occurrence of BRCA mutations, whose role in this setting is still not completely understood. 1 2 Moreover, the role of secondary cytoreductive surgery for recurrent disease has not been standardized.3 4
This video shows the surgical management of a young BRCA1-mutated woman affected by a recurrence of serous endometrial cancer. The aim of this film is to show how a minimally invasive surgical approach is safe and feasible in selected patients.
We present the case of a hepato-renal recess isolated recurrence of serous endometrial cancer. Patient positioning and port placement were critical to achieve an optimal exposure of the liver sixth segment and the Morison’s pouch. An extensive adhesiolysis was performed and the metastasis was then exposed. The tumor infiltrated the liver parenchyma for <2 cm, thus a superficial wedge resection was executed. The procedure was performed in 90 min. The post-operative course was unremarkable; the patient was discharged on post-operative day 3 and she resumed her oral poly ADP ribose polymerase (PARP) inhibitor after 15 days. The histopathology report confirmed the localization of a high-grade serous cancer.
{kind=link}
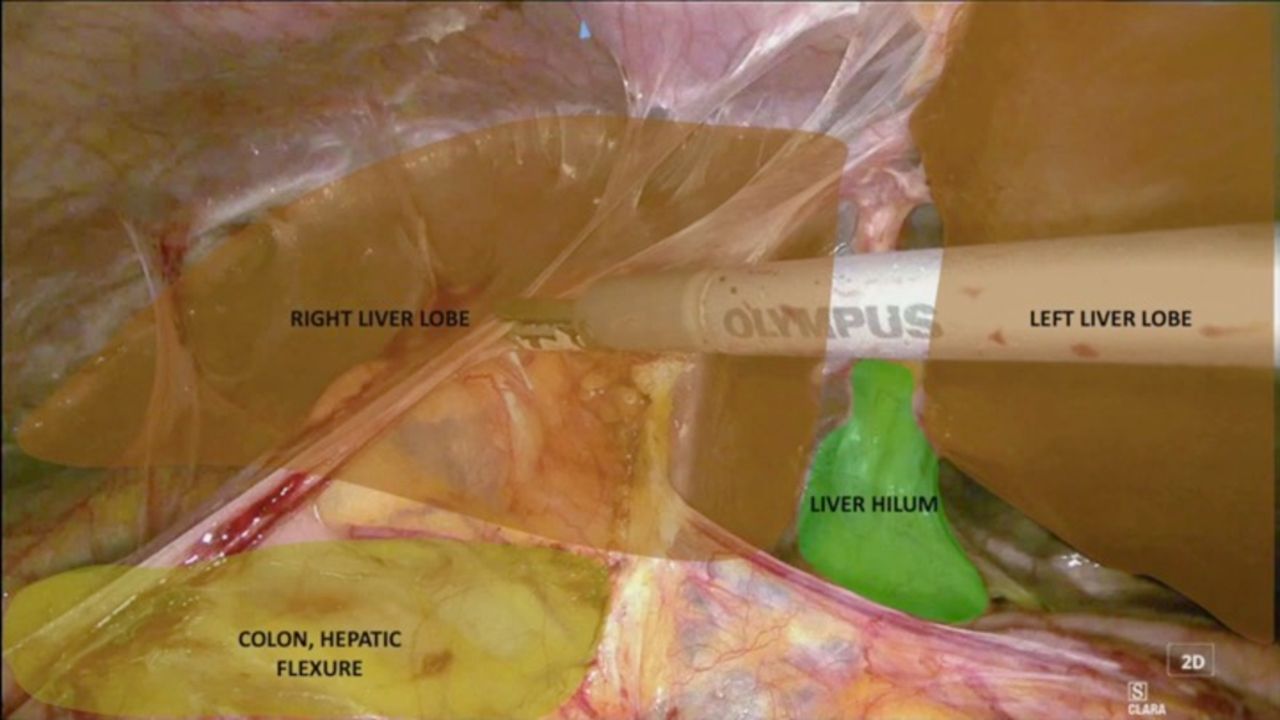
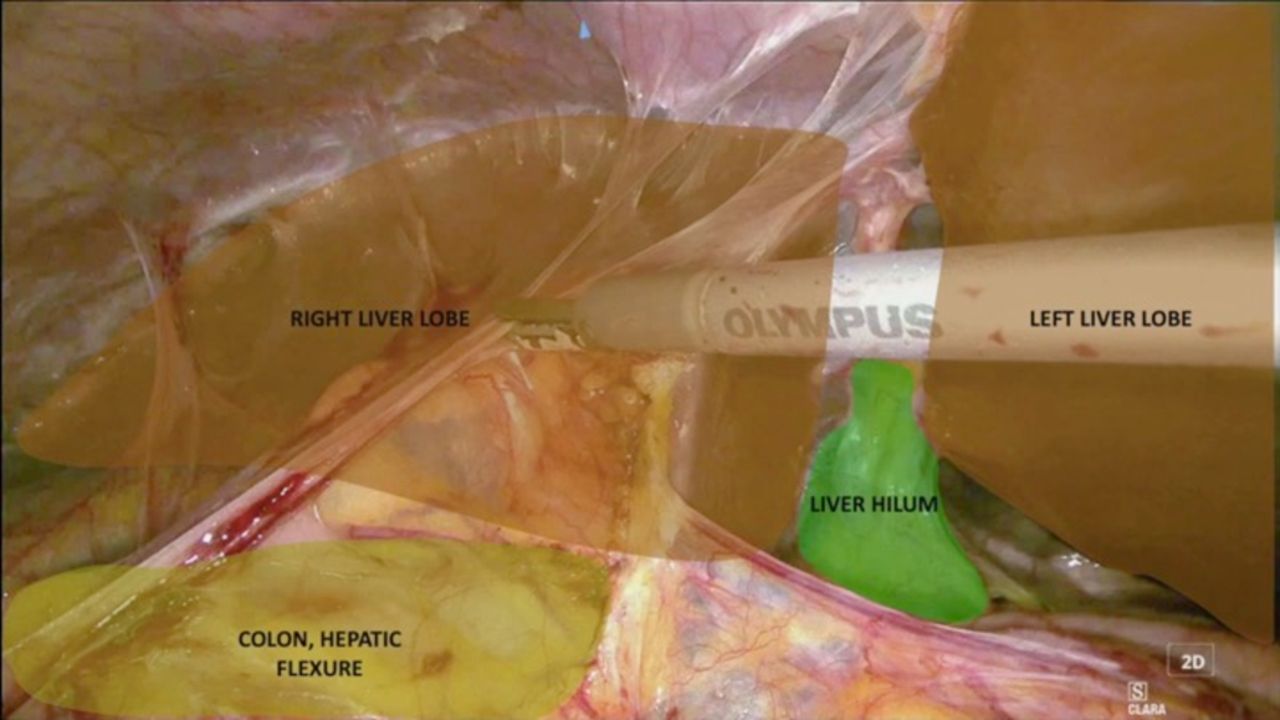
Still image of the video showing and pointing out the anatomical structures involved in the surgery: laparoscopic access to the hepato-renal recess.
Minimally invasive surgery for recurrent endometrial cancer is achievable and beneficial in selected patients. Indeed, potential benefits include reduced blood loss, less pain, faster recovery, and a short interval to adjuvant chemotherapy. The personalized treatment of recurrent endometrial serous cancer should be guided by the molecular pattern of the disease and by the surgical skills with a multidisciplinary approach.
Disclaimer: this video summarises a scientific article published by BMJ Publishing Group Limited (BMJ). The content of this video has not been peer-reviewed and does not constitute medical advice. Any opinions expressed are solely those of the contributors. Viewers should be aware that professionals in the field may have different opinions. BMJ does not endorse any opinions expressed or recommendations discussed. Viewers should not use the content of the video as the basis for any medical treatment. BMJ disclaims all liability and responsibility arising from any reliance placed on the content.
Data availability statement
All data relevant to the study are included in the article.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Protocol number DIPUSVSP-PD-03-2211. Participants gave informed consent to participate in the study before taking part.
Footnotes
Twitter @frafanfani
Contributors VG, FG and FF contributed to the design and the surgical part of the study, VI and FT created the video. GS contributed as a guarantor. All authors provided critical feedback and helped shape the video and the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.