Article Text

Statistics from Altmetric.com
Case Presentation
A 49-year-old woman presented with a 2 week history of presumed menorrhagia and pelvic pain. She presented in the context of being on rivaroxaban treatment (20 mg daily) following a diagnosis of a partially occlusive left lower leg deep vein thrombosis 5 months earlier. The deep vein thrombosis occurred after a period of immobilization following excision of an infected sebaceous cyst on her back. On abdominal examination by the primary care physician, a palpable mass was noted below the level of the umbilicus. Computed tomography (CT) of the chest, abdomen, and pelvis was subsequently ordered. This showed an ill defined, large hypodense uterine mass and multiple scattered well defined nodules in the lungs. Of note, a CT pulmonary angiogram performed 4 months prior in the context of working up her deep vein thrombosis, showed no pulmonary emboli and no lung nodules. At this point, she was referred to our gynecology oncology unit for further evaluation.
Apart from significantly increasing pelvic pain requiring opioid analgesia and ongoing bleeding, the patient complained of a 2 week history of frequent aura without headache. Her medical history was significant for psoriasis not requiring current treatment, infrequent migraines, and a pulmonary embolus 20 years prior, presumed provoked by use of the combined contraceptive pill. She had no additional surgical history, took no medications other than rivaroxaban, and had no known drug allergies. She worked full time in administration, was fit and active, with an Eastern Cooperative Oncology Group (ECOG) score of 0.
On examination, body mass index was 33 kg/m2. Neurological examination was unremarkable (and subsequent CT of the head was normal). There was no appreciable lymphadenopathy on systematic examination. A uterine mass was palpable to the umbilicus. On speculum and vaginal examination, the cervix was distended by a tumor pushing down from the uterus, but was not itself involved. There was no vaginal involvement. The uterus was not fixed to surrounding structures. On rectal examination there was no parametrial involvement and no rectal invasion or nodularity in the pouch of Douglas.
Dr Wastney: What are the Salient Features on Imaging?
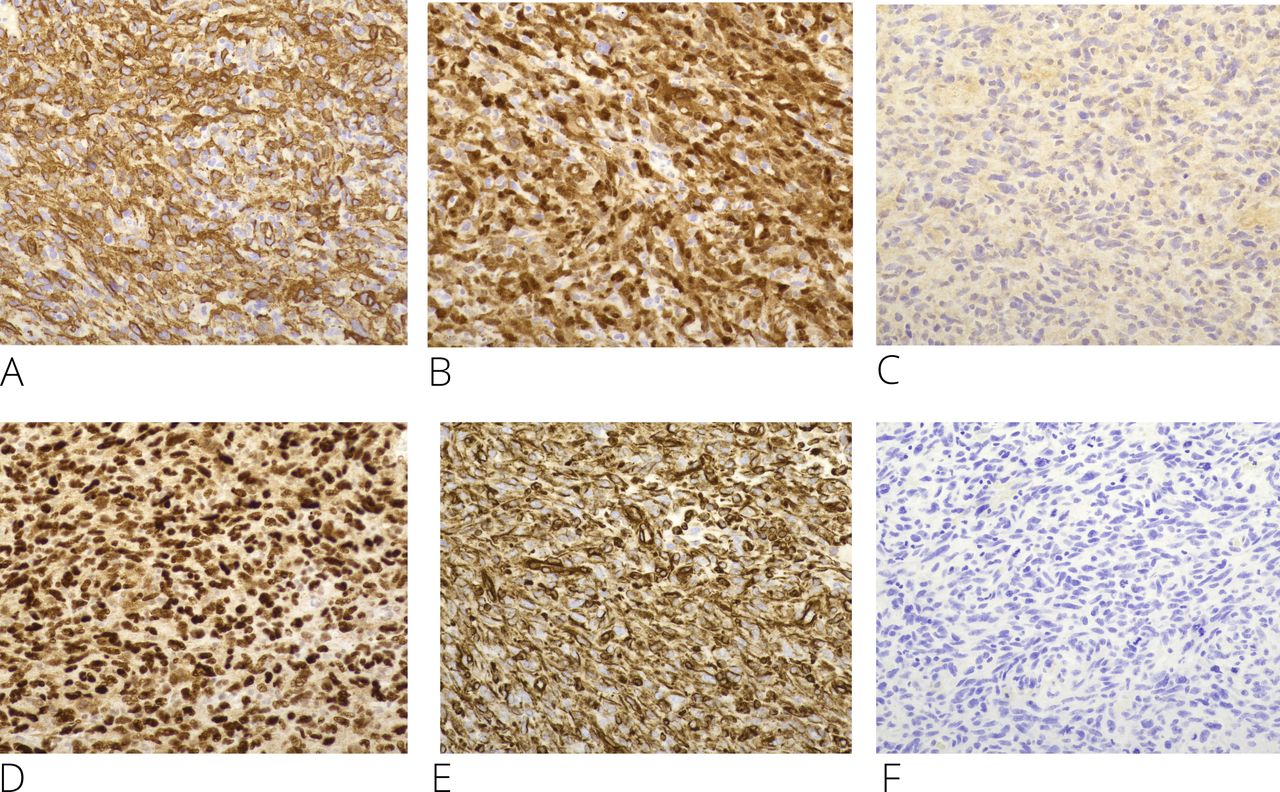
The two most salient features of this CT scan are those in the chest and uterus (Figure 1). In the chest, there are multiple scattered well defined nodules which are in keeping with metastatic deposits. In the uterus, there is an ill defined hypodense mass within the body and fundus, measuring 10×8×11 cm. Of note, and relevant to later in the case, there is no evidence of thrombus in the pulmonary veins.

Initial CT images showing (A) a sagittal image of the enlarged uterus, (B) an axial chest view of a clear pulmonary vein, and (C) an axial chest view of scattered lung nodules.
A biopsy was taken per vaginal, demonstrating an undifferentiated sarcoma.
Dr Cummings: What are the Pathological and Immunohistochemical Features of the Tumor and What are the Diagnostic Challenges in Uterine Sarcoma?
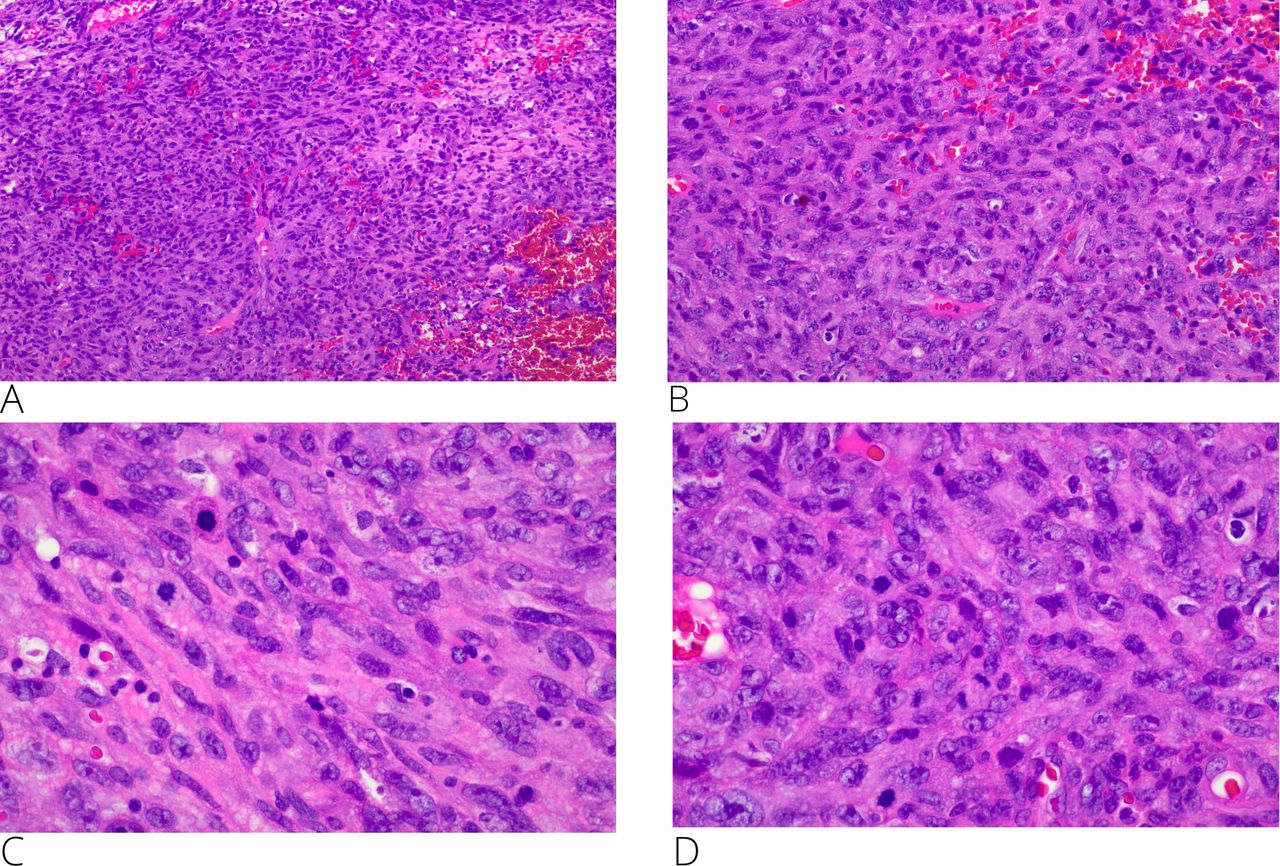
This tumor was largely hemorrhagic and necrotic. Where there was viable tumor, there were diffuse sheets of cells, with indistinct cell boundaries, ovoid pleomorphic nuclei, prominent nucleoli, and frequent mitoses (>50 per high power field) (Figure 2). No epithelial differentiation was seen. Immunostaining was undertaken, and the tumor was positive for p53 (mutant pattern), vimentin, desmin, actin, and cyclin D1 (Figure 3). There was a very high proliferation rate with Ki67. Staining for progesterone receptors was weakly positive in 40% of the cells. No immunostaining was seen for H-Caldesmon, CD10, WT1, ER, p40, EMA, MNF116, p16, Melan A, or c-kit.
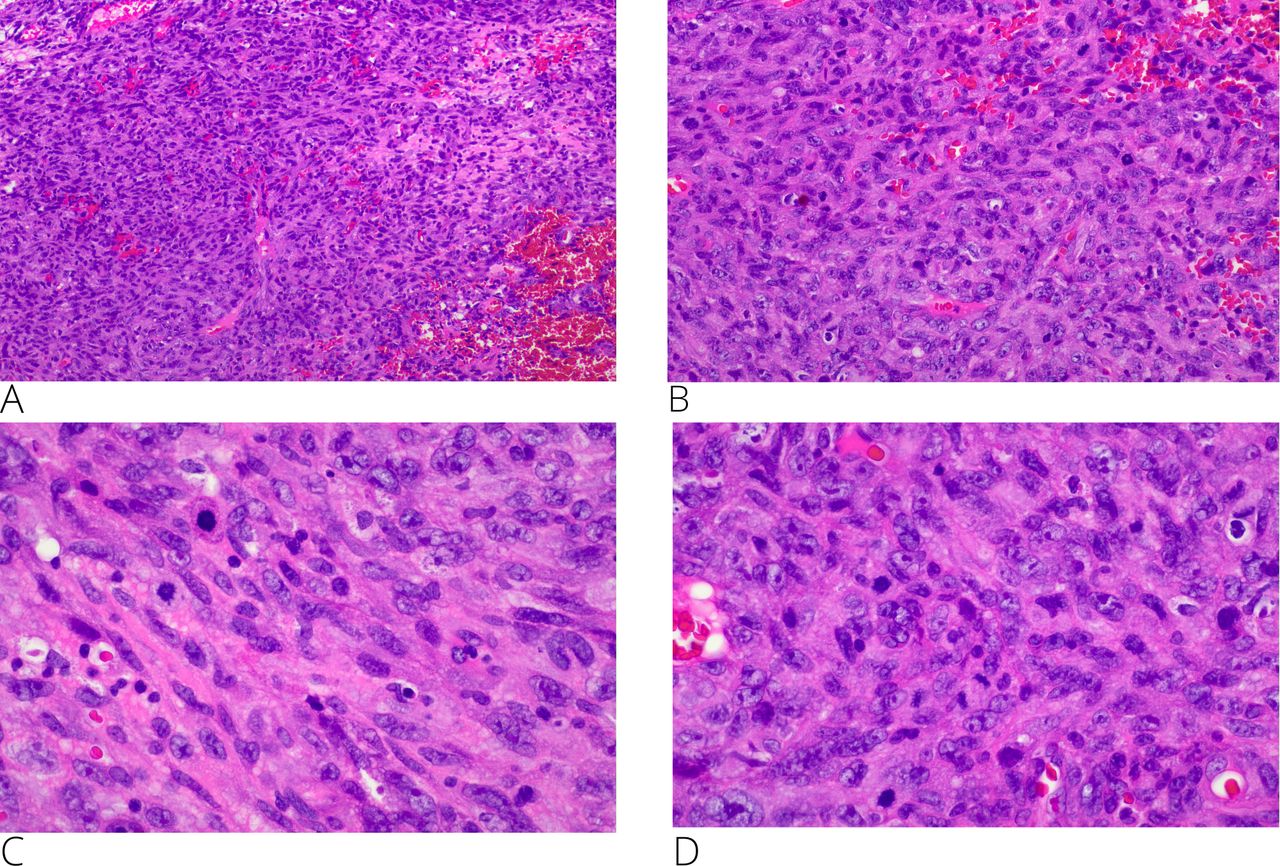
Hematoxylin and eosin staining. (A) Low, (B) medium, and (C, D) high power hematoxylin and eosin images showing diffuse sheets of cells, with indistinct cell boundaries, ovoid pleomorphic nuclei, prominent nucleioli, and frequent mitoses.

Immunohistochemistry images showing positive staining for (A) actin, (B) cyclin D1, (C) desmin, (D) p53 (mutant pattern), and (E) vimentin. (F) Negative staining for MNF116.
Ultimately, undifferentiated uterine sarcoma is a diagnosis we can arrive at after examination of the morphology, immunohistochemistry, and molecular profile does not result in the classification of the tumor into a known category.1 As the name suggests, the features of the morphology and the immunostaining are defined by their lack of evidence for any cell differentiation.2 Pathologists should be mindful of the true rarity of the diagnosis, and that rates of undifferentiated uterine sarcoma in the literature may not be truly representative, given the likely inclusion in reported series of other sarcoma subtypes.3
Dr Nicklin: What Options for Management Would You Discuss With the Patient at This Point?
These cases present a clinical challenge. At the outset, it is important that the patient and her family understand the poor prognosis related to the pathology and presentation of International Federation of Gynecology and Obstetrics stage IVB disease. There are potential roles for surgery, radiotherapy, and chemotherapy in this case (or combinations thereof), and the risks and benefits of each approach needs to be discussed with the patient. In this case, the advanced stage of disease and the palliative nature of all of the options, in addition to the role of and need for palliative care, must be made clear from the beginning.
While hysterectomy in early stage disease appears to be associated with a survival benefit in these patients,4 I would consider the role of hysterectomy in this case as beneficial only for palliation to give symptom control of both pain and bleeding. Again, while in early stage disease the addition of adjuvant therapy after optimal surgical cytoreduction may add a survival benefit (accepting the very limited data in undifferentiated uterine sarcomas5), here the role would be palliative, in an attempt to control symptoms and possibly stall progression of disease.
Ultimately, this is a patient who is otherwise well, with an ECOG of 0, and with pelvic disease amenable to resection based on clinical findings. I would offer her a palliative hysterectomy for symptom control with a view to considering palliative systemic therapy thereafter.
Dr Kuchel: What Evidence do we Have for Systemic Chemotherapy Options in These Patients?
Owing to the rarity of undifferentiated uterine sarcoma, there is no prospective evidence specific to the disease to guide systemic treatment of these patients. We do know, however, that there were small numbers of undifferentiated uterine sarcomas in the prospective trials on sarcoma more broadly, and certainly we extrapolate from these trials in cases such as this. Overall, there is no standardized chemotherapy regimen for systemic therapy in either completely resected disease or in advanced/metastatic disease, largely owing to the limited number of clinical trials, the rarity of the disease to recruit for those trials, and the overall poor prognosis and aggressive nature of these cases.6 Based on small, mostly non-randomized trials (largely including leiomyosarcomas; exploring various regimens, including gemcitabine, docetaxel, doxorubicin, cyclophosphamide, and vincristine), adjuvant chemotherapy may be associated with improved progression free survival in patients with completely resected uterine sarcoma. However, the results were not consistent, and in the randomized studies there was no improvement in overall survival.5
There is an also an absence of prospective evidence to recommend the benefit of systemic therapy in advanced undifferentiated uterine sarcoma, however expert opinion generally guides its use in this scenario, owing to a lack of other options and the certainty of rapid progression with no treatment. Discussion around potential risks and benefits of treatment is therefore central to patient decision making. Commonly used chemotherapy options in metastatic or advanced undifferentiated uterine sarcoma include doxorubicin or gemcitabine and docetaxel. The GeDDiS trial published in 2017 randomized 257 patients with locally advanced or metastatic soft tissue sarcoma to these two treatment options, finding similar outcomes with either regimen, with patients in both arms having a median progression free survival of 23 weeks.7 As before, GeDDiS recruited most of the common subtypes of soft tissue sarcoma (uterine and non-uterine) and there were only small numbers of non-leiomyosarcoma uterine sarcomas included. Overall, most medical oncologists would favor single agent doxorubicin in this scenario to limit potential toxicity, reserving combination therapy for second line or subsequent line treatment. A further option is the multitargeted tyrosine kinase inhibitor, pazopanib, investigated in the PALETTE (pazopanib for metastatic soft tissue sarcoma) trial.8 This showed improved progression free survival but not overall survival compared with placebo in soft tissue sarcomas following anthracycline based chemotherapy.
The case was discussed at the gynecology oncology multidisciplinary team meeting and a consensus was made to proceed with palliative hysterectomy 8 days later, with lower limb Dopplers prior to surgery and consideration of placement of an inferior vena cava filter if persistent lower limb clot remained. Four days later the patient presented following lower limb Dopplers, confirming a deep vein thrombosis. Alongside this, her pain was rapidly escalating since her previous review, to the point of pain crisis. She was admitted for pain management, and a CT pulmonary angiogram and CT abdomen and pelvis were undertaken given the potential for progressive embolic and malignant disease.
Dr Wastney: What are the Salient Changes on This Imaging? Also, I Note the Tumor Deposit in the Pulmonary Vein; How do we Distinguish Between Tumor Emboli and Hematogenous Emboli?
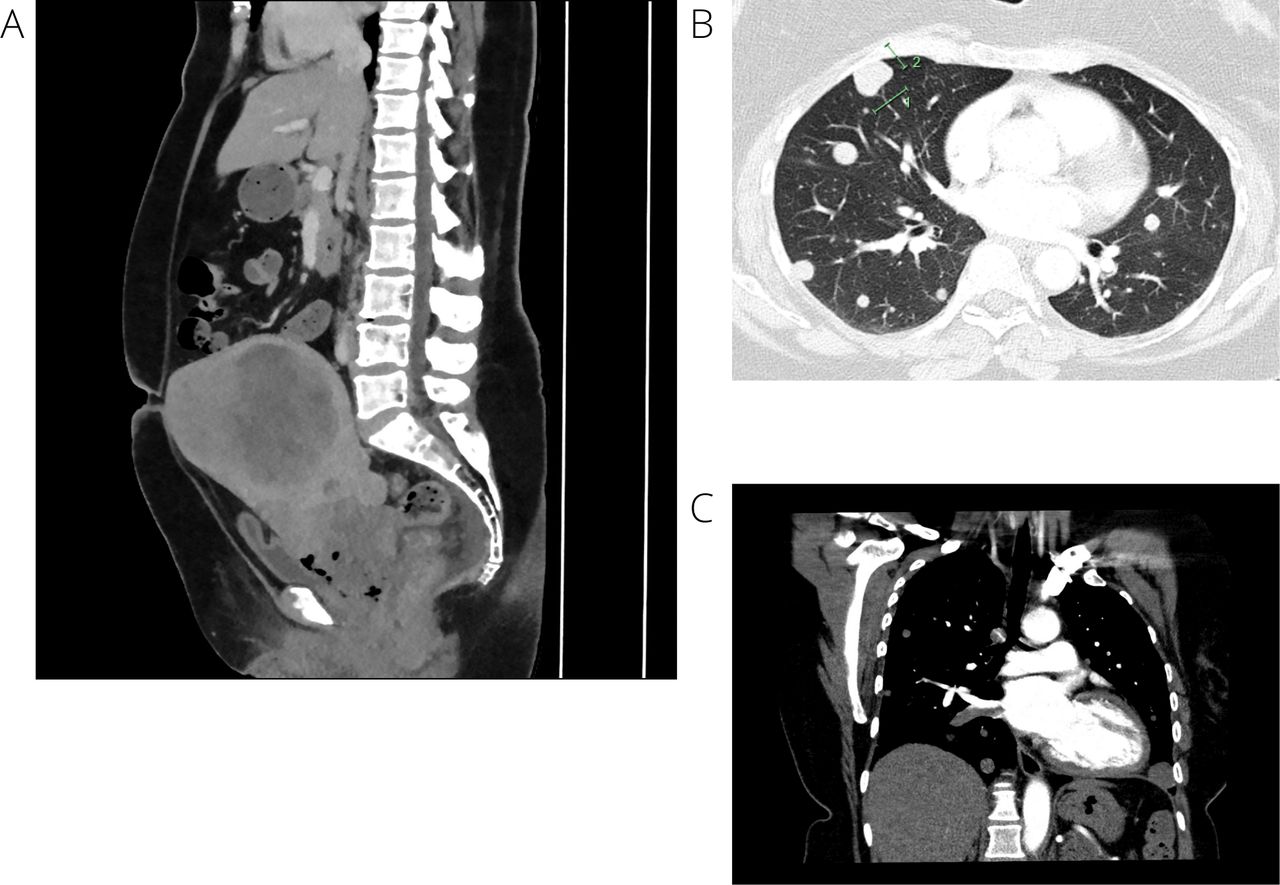
This CT, done less than 2 weeks after the previous imaging, shows significantly progressive disease (Figure 4). There were innumerable metastatic lesions in the chest, having progressed in both size as well as number. Furthermore, there were hepatic metastases, as well as progression in the size of the uterine mass, at that time measuring 16×11×17 cm, with gas and fluid present in the region of the cervix and vagina, possibly representing necrosis. The tumor contacted the rectum and small bowel, with loss of the fat plane between the uterus and rectum.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Follow-up CT imaging showing (A) progressive uterine disease in sagittal image, (B) an axial chest view of progressive pulmonary metastases, and (C) a coronal chest view of the pulmonary vein thrombus.
There were new sub-segmental pulmonary emboli bilaterally and tumor thrombus in the right lower pulmonary vein. While this was not present on the previous CT, it was possible to see a pulmonary nodule contacting a vein in that location, which had now progressed. The involved pulmonary vein was now expanded and filled with soft tissue density material along the wall that could be traced back to the pulmonary nodule. The density of the material in the vein, its location within a pulmonary vein, position along the wall, and the continuity with the pulmonary nodule were all in keeping with tumor thrombus, rather than bland/hematogenous thrombus.
Dr Nicklin: What Options for Treatment Would You Now Offer the Patient?
It is clear that this patient had rapidly progressive disease with an aggressive histology. The role of palliative hysterectomy was no longer of benefit, given the extent of the surgery that would be required for resection in the setting of a rapidly changing and progressive palliative clinical picture.
Palliative care engagement was critical and the mainstay of the treatment moving forward. Unfortunately, chemotherapy was likely to be of little benefit here, given the general non-responsiveness of undifferentiated sarcoma to systemic therapy, especially one where tumor biology was declaring itself as so aggressive. Radiotherapy might play a role in symptom relief.
Closing Summary
Uterine sarcoma represents a rare and challenging clinical presentation. Much of the data when it comes to managing these patients arise from single center case series and consensus opinions. Even more challenging is that within this group of tumors (which represent <10% of all uterine malignancies), exists the rarer group of undifferentiated sarcoma, which are aggressive, present most often at a late stage, and are associated with a very poor prognosis.9 These tumors present a radiological, pathological, surgical, adjuvant therapy, and palliative care challenge for all physicians involved in the management of these patients.
Pathologists must be aware of the need to exclude other sarcomas as the diagnosis, and be aware that these tumors may mimic other pathologies, such as high grade endometrial stromal sarcoma.2 3 While the recommended management is hysterectomy, bilateral salpingoophorectomy, and adjuvant radiotherapy and/or chemotherapy,9 the impact on overall survival of these interventions may be limited. Given the aggressive nature of undifferentiated sarcoma, the poor prognosis, and the high rate of relapse of disease, an intensive multimodal approach to therapy must be considered, particularly in patients with disease apparently confined to the pelvis.
Systemic therapy should be considered for undifferentiated uterine sarcoma. Extrapolating from soft tissue sarcoma trials, which included uterine sarcomas in only small numbers, the main option is chemotherapy, with consideration of targeted therapy with tyrosine kinase inhibitors. In the upfront setting, options include gemcitabine and docetaxel, or doxorubicin alone, in order that toxicity can be limited and combination therapy can be reserved for subsequent lines of treatment. This is supported by the findings of the GeDDiS trial, whereby median progression free survival in patients treated for unresectable or metastatic sarcoma was 23.3 weeks (95% confidence interval (CI) 19.6 to 30.4) in the doxorubicin group and 23.7 weeks (95% CI 18.1 to 20.0) in the gemcitabine and docetaxel group. While we generally favor doxorubicin alone in patients where treatment intent is palliative, consideration in otherwise very well patients in whom tumor shrinkage is paramount can be given to doxorubicin and ifosfamide. This is based on the findings of the EORTC 62012 trial, in which patients with advanced or metastatic disease treated with the combination chemotherapy compared with doxorubicin alone had a median progression free survival of 7.4 months versus 4.6 months (hazard ratio (HR) 0.74, 95% CI 0.60 to 0.90, p=0.003) and higher overall response rate (26.5% vs 13.6%), but with increased toxicity and no significant improvement in overall survival.10 In recurrent or progressive disease, the tyrosine kinase inhibitor pazopanib was shown as a single agent in the PALETTE trial to result in a median progression free survival of 4.6 months compared with 1.6 months in the placebo group in patients with progressive disease despite standard chemotherapy (HR 0.31, 95% CI 0.24 to 0.40, p<0.0001).8 Hormonal therapy is generally not considered, given the frequent absence of hormone receptors, which also explains the absence of prospective clinical trials for this treatment.6 Adjuvant radiotherapy in patients who have undergone surgical resection should be considered to achieve locoregional control,11 however this approach is of less clear benefit in patients with disease outside of the pelvis at the time of diagnosis. Given the generally limited options for treatment, patients with sarcoma should be considered for enrollment in clinical trials. Palliative care services should be engaged early, particularly in patients with metastatic disease at diagnosis.
Ethics statements
Patient consent for publication
Footnotes
Twitter @Jim Nicklin
Contributors All authors conceived of, contributed to, and approved the final version of the case study.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Commissioned; internally peer reviewed.