Article Text

Statistics from Altmetric.com
Summary
Since the initial description of extended pelvic surgery for gynecological cancer recurrences, lateral involvement of the pelvic side wall has been considered an absolute contraindication for pelvic exenteration. Previous irradiation of the pelvis, and involvement of major vascular structures, nerves, or pelvic bones impacted the success of the surgery and resulted in a poor oncological outcome.
In 1999, Höckel focused his interest on a pelvic side wall resection technique and provided a thorough description of laterally extended endopelvic resection with a curative intent.1 This newly developed concept was adopted by most surgical teams and rebranded as laterally extended pelvic resection. This en bloc pelvic resection allows tumor free margins to be obtained in the case of lateral pelvic side wall involvement, with acceptable mortality rates and improved overall survival in a selected group of patients for whom palliative therapy would be the only alternative. This complex and ultraradical surgical technique allows negative margins to be achieved in more than 75% of patients when it is performed by expert teams in highly selected patients. However, these procedures are associated with a high rate of postoperative complications.2
In this video, we present an open anterior pelvic exenteration and a laterally extended pelvic resection performed by a senior oncological surgeon in a referral cancer center. The surgery was performed in a 52-year-old patient diagnosed with squamous cell cervical cancer involving the right pelvic wall and previously treated with concomitant chemoradiotherapy. At the end of this treatment, she presented a large symptomatic vesicovaginal fistula with residual tumor. The reconstructive surgery was carried out, performing a continent urinary diversion with a Miami pouch3 and deep inferior epigastric perforator flap for vaginal reconstruction.4

{kind=link}
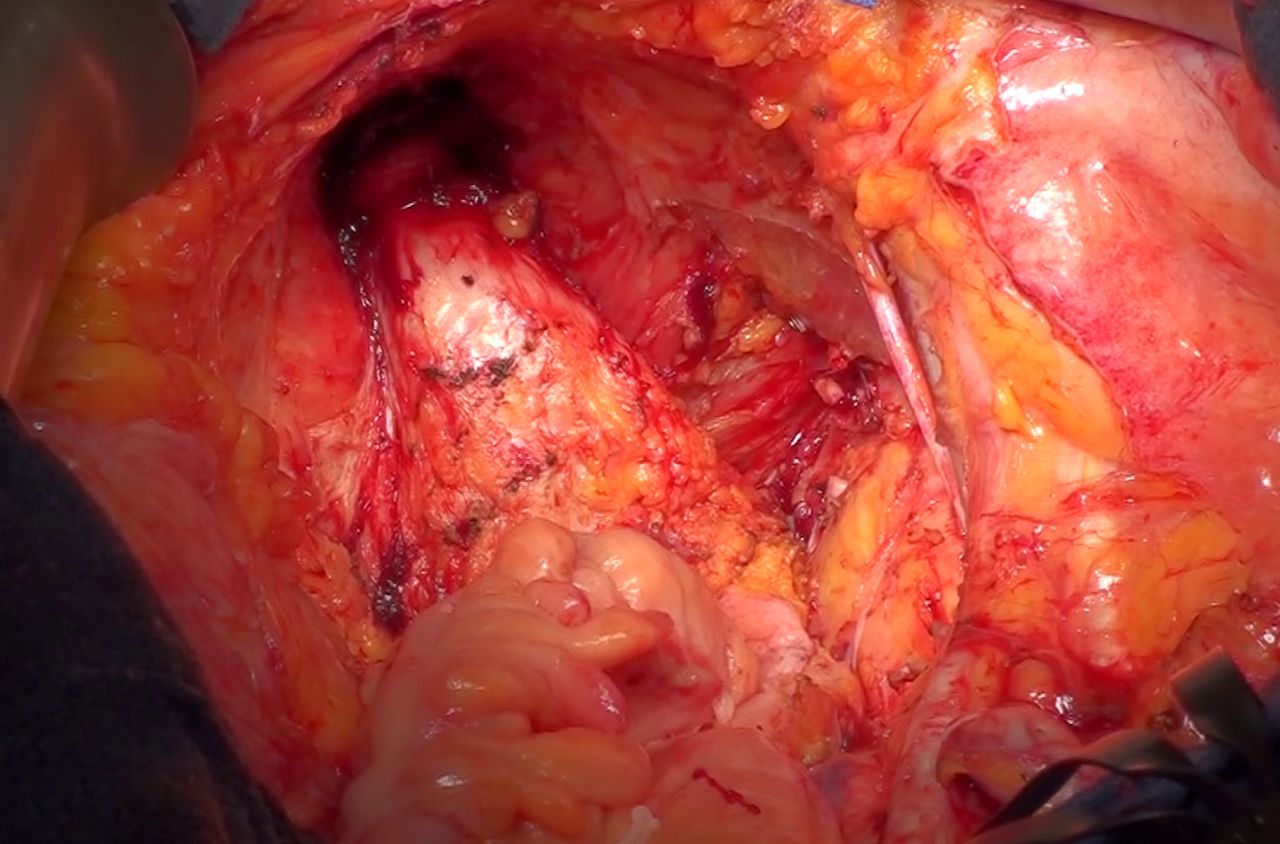
Final view after anterior pelvic exenteration and laterally extended pelvic exenteration for cervical cancer involving the right pelvic wall.
Data availability statement
There are no data in this work.
Ethics statements
Patient consent for publication
Footnotes
Twitter @manon_daix, @AngelesFite, @Alejandra
Contributors MD, MAA, HL, and KV: conceptualization, video editing, and writing-original draft. AM: conceptualization, project administration, supervision, and writing-review. GF: conceptualization, project administration, surgery and video recording, supervision, and writing-review.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.