Article Text

Statistics from Altmetric.com
Retroperitoneal sarcoma is a rare malignancy arising from mesenchymal cells.1 Surgical resection with wide negative margins remains the cornerstone of treatment as it decreases the risk of recurrence.2 The proximity to critical abdominal structures makes a total resection with nerve and vascular preservation a challenge.3 The case described concerns a 33-year-old nulliparous patient with severe sciatic pain radiating into the genital and gluteal regions and urethral obstruction due to a paravaginal mass bulging into the mucosa and attached to the pelvic floor. Pelvic magnetic resonance imaging (MRI) showed a well-defined solid formation measuring 6.7×5.5×5.2 cm between the bladder and the rectum, extending to the lateral vaginal wall. A biopsy showed a mesenchymal neoplasm originating in the soft muscle tissue with atypical nuclei.
Anatomical and functional damage is a concern for fertility and nerve sparing surgery, so we developed the following strategy to approach the mass:4 (1) surgical team positioning and trocar placement; (2) bladder and right ureter mobilization: the dissection and mobilization were performed to avoid post-operative complications; (3) prophylactic control of bleeding by vascular dissection: temporary vessel ligation; (4) somatic and autonomic nerve exposure: recognition and dissection of the route of the sacral nerve were undertaken because of the patient’s symptoms; (5) mass resection: a laparoscopic resection for surgery-free margins and complete mass mobilization that allowed the procedure to be finished vaginally. The surgery lasted 5 hours.
Pathological analysis showed a conventional soft tissue leiomyosarcoma, histological grade G1, 6.9 cm, with free surgical margins. The patient experienced a significant improvement in the pain and was discharged from hospital on the second day after surgery with no need for opioids or blood transfusion and no signs of recurrence of disease in the latest MRI scan at 1-year follow-up.
We conclude that it is possible to perform a successful retroperitoneal approach to soft tissue sarcoma on the pelvic floor, aimed at nerve preservation, vascular control, and fertility preservation.

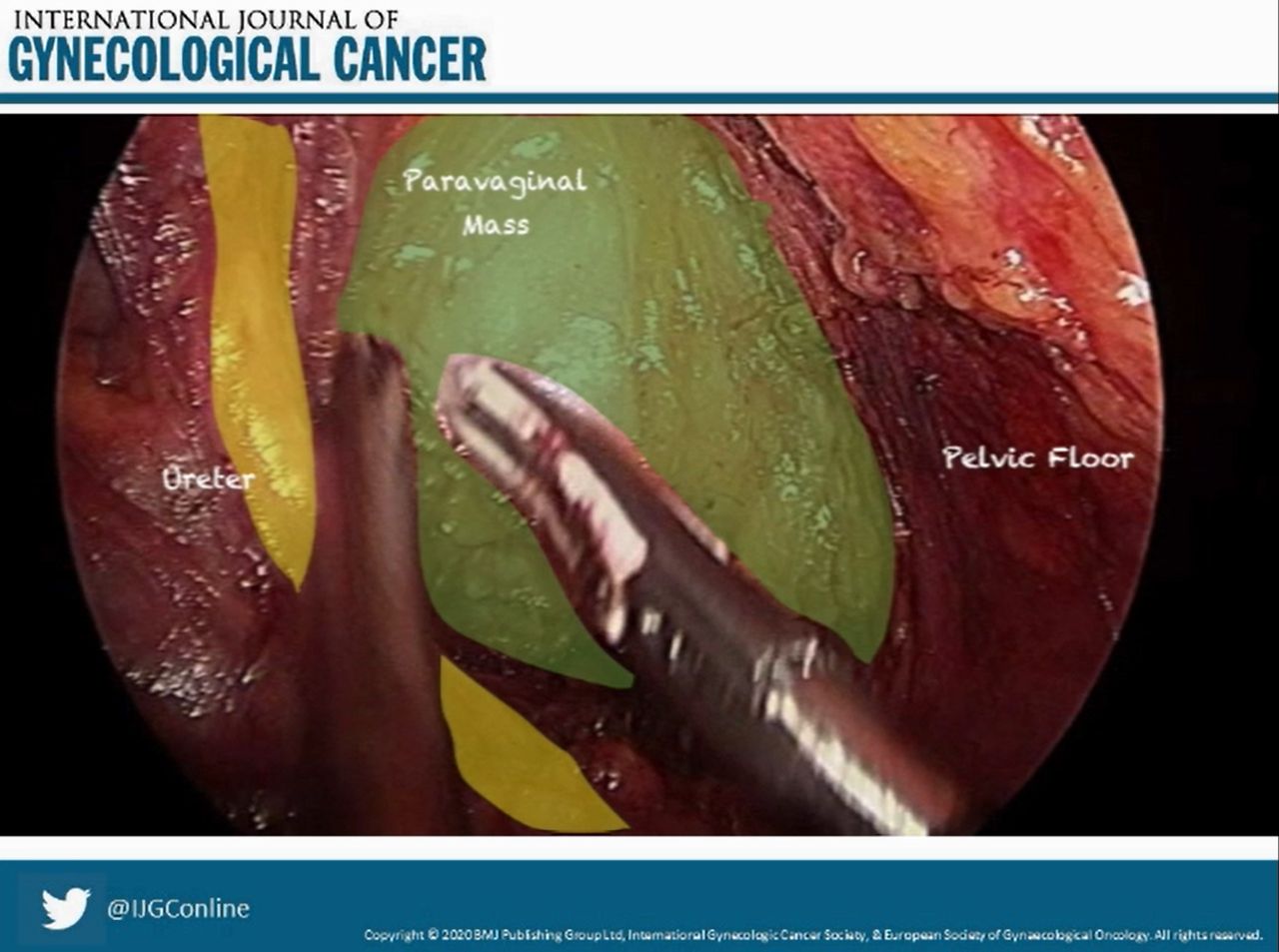
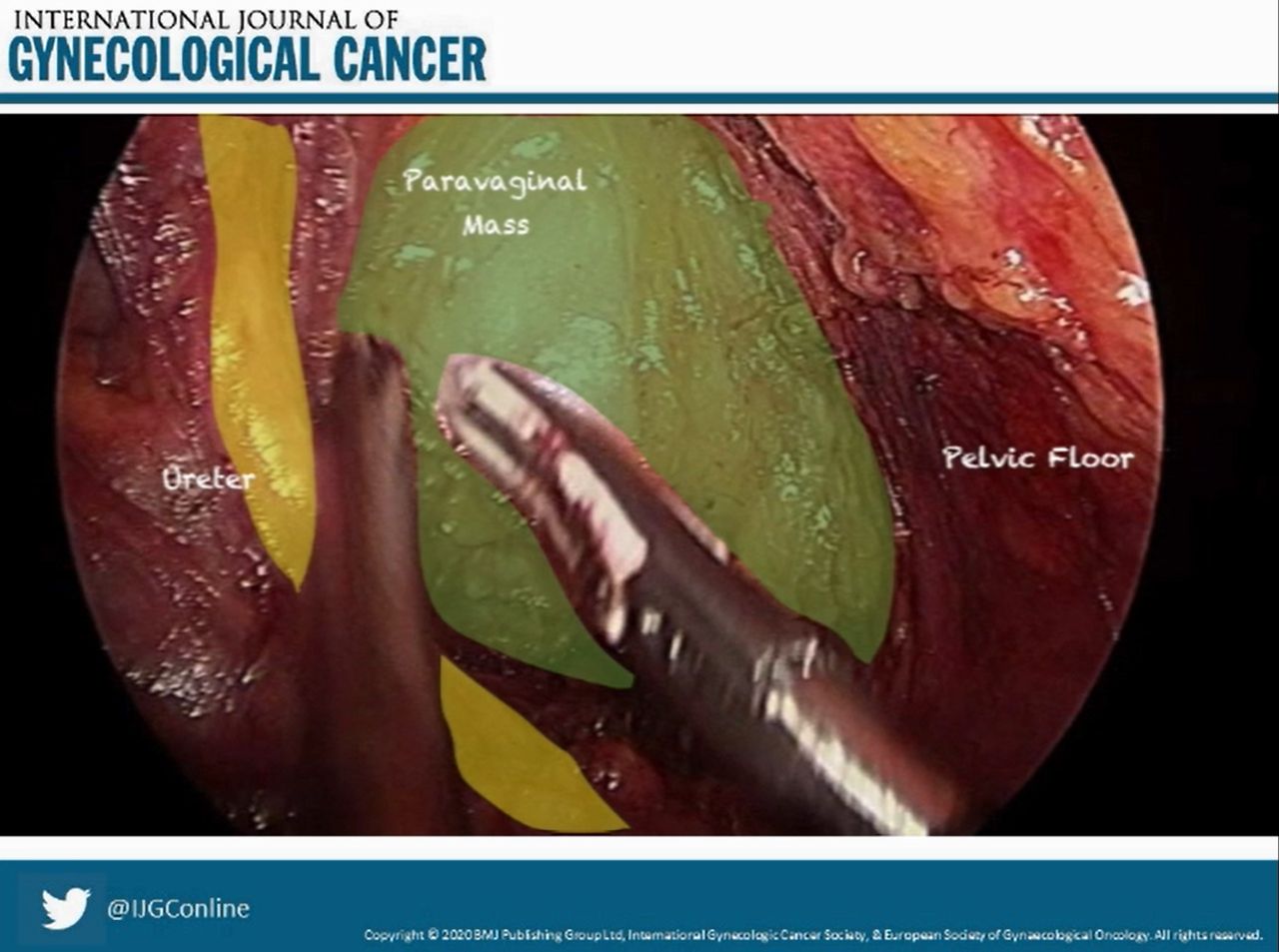
Nerve preservation dissection to access the para-vaginal sarcoma.
{kind=link}
{kind=link}
Dissected pelvic mass and its anatomical relationships with the ureter and the pelvic floor.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information
Ethics statements
Ethics approval
The study was approved by the appropriate Institutional Review Board - Comitê de ética em pesquisa com seres humanos do Hospital Israelita Albert Einstein number CAAAE: 40495920.9.0000.0071 and written informed consent was obtained from all subjects.
Footnotes
Contributors GBB: video creator and edition; DDAM: narration, abstract and submission; VAB: final submission edition; AT: images edition; EZ: organizational support; RM-M: anatomy review, main surgeon, edition review, video coordination.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.