Article Text

Abstract
Increasing numbers of women are surviving for longer with epithelial ovarian cancer. Consequently, there is increased focus on long-term quality of life in national guidance. Psychosexual morbidity including vaginal dryness, pain during intercourse (dyspareunia), reduced libido, and negative perceived body image exacerbate stress and anxiety and impact intimate relationships. Although a priority for women with epithelial ovarian cancer, clinicians seldom discuss sexual problems. Therefore, psychosexual morbidity and the associated distress remain unaddressed. We synthesize evidence from primary qualitative and quantitative research studies exploring psychosexual morbidity in women with epithelial ovarian cancer to identify potential risk factors and common symptoms, to facilitate the identification and management of sexual problems in clinic. Literature (2008–19) from 10 databases identified 29 suitable publications (4116 patients). The papers were assessed to answer the question: “What are the key potential risk factors and presentations of psychosexual morbidity in women with epithelial ovarian cancer?” Current literature lacks consensus in defining clinically significant psychosexual morbidity in women with epithelial ovarian cancer. Discrepancies in measurement tools, questionnaires, and primary outcome measures confound result interpretation, limiting wider application. Key potential risk factors identified included: younger age (<53 years); pre-menopausal status at diagnosis; aim of treatment; extent of surgery; more courses of chemotherapy; cardiovascular co-morbidities; and anxiety and depression. Up to 75% of women with epithelial ovarian cancer reported adverse changes in their sex lives following diagnosis and, of the sexually active, vaginal dryness affected 81–87% and pain 77%. Other prevalent symptoms included: reduced sexual desire and activity, impaired orgasm, diminished perceived body image, and reduced partner intimacy. Psychosexual morbidity represents a significant unmet need for women with epithelial ovarian cancer. Effective treatment necessitates a multimodal approach encompassing medical, psychoeducational, and physiotherapy-based strategies. Future studies need agreement in their questionnaires, definitions, thresholds, and primary outcome measures for meaningful interstudy comparisons to be drawn.
- ovarian cancer
- quality of life (PRO)/palliative care
- ovarian neoplasms
- gynecology
- ovary
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, an indication of whether changes were made, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Epithelial ovarian cancer, the sixth most common cancer in women in the UK, is usually diagnosed late: 60% of 7400 annual diagnoses have advanced stage disease.1 Consequently, most patients require extensive cytoreductive abdominopelvic surgery involving total hysterectomy, bilateral salpingo-oophorectomy, tumor debulking, and omentectomy, in addition to platinum-based chemotherapy (usually multiple courses for disease recurrences until chemoresistance limits further treatment).2 Thanks to recent advances in treatment options including poly ADP ribose polymerase (PARP) inhibitors,3 the number of women living with their disease as women with epithelial ovarian cancer is growing, with over 40% of patients alive at 5 years.1 In view of the increasing number of people surviving or ‘Living With And Beyond Cancer’, Macmillan and National Health Service (NHS) England have emphasized the importance of holistic and person-centered care to maximize quality of life.4 Women with epithelial ovarian cancer are ideal patients in whom to target efforts to improve quality of life, given their relatively young age at diagnosis (63 years median age at diagnosis) when most women are still living a full and active life, their extensive and sometimes debilitating disease and treatment, and the growing length of time with which they are living with their cancer.1 3
Women with epithelial ovarian cancer experience psychosexual morbidity (psychological and physical sexual problems) secondary to cytoreductive surgery to remove both ovaries and extended disease (or more rarely one ovary if undergoing fertility sparing surgery), gonadotoxic chemotherapy and sometimes radiation.5 Physically, ovary removal leads to a drop in circulating estrogen, more profoundly if pre-menopausal at the time of treatment, leading to vaginal atrophy, and reduced circulating testosterone and androstenedione contributing to reduced libido, and reduced peripheral conversion to estrogen.5 Psychologically, the visual effects of surgery and chemotherapy such as scarring, stomas, and hair loss can affect the woman’s perceived body image, which is associated with psychosexual morbidity.6 Socially, intimate relationships may struggle to navigate cancer treatments and symptoms, as roles may shift from partner to patient or partner to primary caregiver.7 This can lead to patient and partner emotional withdrawal from the relationship and contribute to anxiety and depression.8 Overall, these changes mean that women with epithelial ovarian cancer can encounter increased difficulty with sexual desire, arousal, orgasm, and sexual satisfaction compared with a healthy age-matched population.5
Psychosexual morbidity in women with epithelial ovarian cancer remains overlooked in clinic and under-represented in the literature, even as a direct side effect of the cancer and its treatment. Given that there are numerous simple and relatively low-cost measures already available to address such issues (vaginal lubricants), managing sexual problems offers a method to swiftly improve the quality of life of women with epithelial ovarian cancer. However, both clinicians and patients are unlikely to raise it for discussion.5 Women with epithelial ovarian cancer report psychosexual morbidity to be a priority in questionnaires yet do not raise it in clinic. Cited barriers to raising psychosexual morbidity in clinic arise from the clinician (perceived lack of time, insufficient training or resources, expecting the patient to bring up sexual problems if affected, and fear of embarrassing the patient)9 and the patient (requiring permission to talk about psychosexual morbidity, potentially considering sexual function as lower in their hierarchy of problems than survival, and seeking to provide 'socially desirable' responses).10 11 For clinicians to feel confident in exploring these themes so that patients then feel 'permitted' to discuss sexual issues,10 evidence-based knowledge of the common potential risk factors and presentations of psychosexual morbidity is required. This review examines the latest primary qualitative and quantitative research, aiming to identify potential risk factors, protective factors, and common presentations of psychosexual morbidity in epithelial ovarian cancer to improve management and maximize quality of life.
Methods
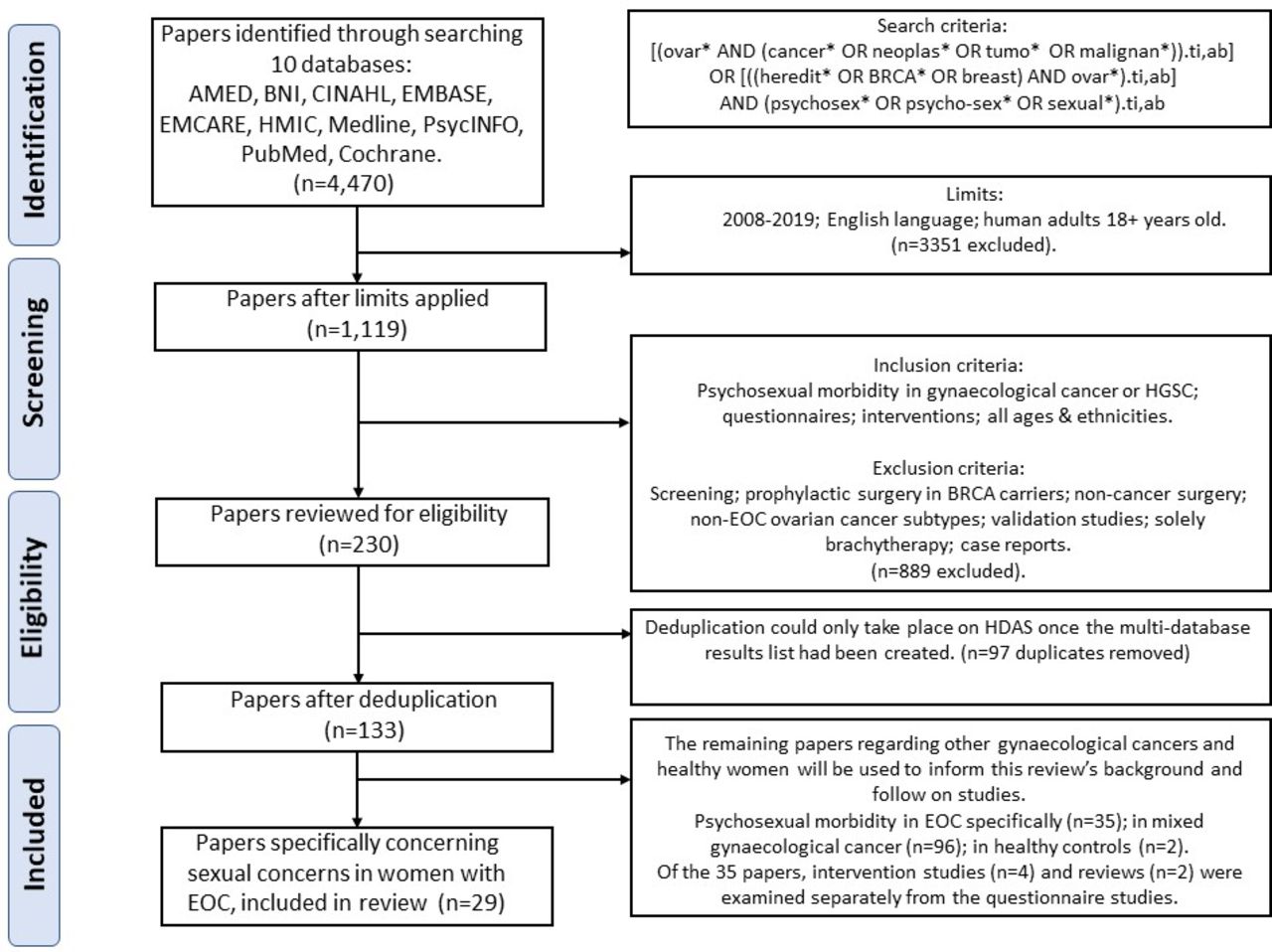
In order to answer the question: “What are the key potential risk factors and presentations of psychosexual morbidity in women with epithelial ovarian cancer?”, the search tool Healthcare Databases Advanced Search (HDAS) provided by the National Institute for Health and Care Excellence (NICE) and NHS Health Education England was used to investigate nine databases. The Cochrane Library was then searched (Figure 1). Potentially relevant studies were reviewed for eligibility and duplicates removed, leaving 29 primary research papers exploring psychosexual morbidity in women with epithelial ovarian cancer. Full texts and conference abstracts were critically appraised independently by two reviewers for methodological quality and their ability to answer the search question (see Figure 1 for inclusion/exclusion criteria). Included papers investigated psychosexual morbidity in epithelial ovarian cancer generally or specifically high-grade serous ovarian cancer which accounts for 90% of epithelial ovarian cancer.1 Fallopian tube and primary peritoneal cancer were also included. Findings populated a results table from which common themes were extrapolated concerning potential risk factors, protective factors, presenting symptoms, and research methods (see Online supplemental tables 1–3).
Supplemental material
{kind=link}
PRISMA flow diagram. Healthcare Databases Advanced Search (HDAS) tool provided by NICE and NHS Health Education England, 10 databases: Allied and Complementary Medicine (AMED), British Nursing Index (BNI), Cumulative Index to Nursing and Allied Health Literature (CINAHL), Excerpta MEDICA database (EMBASE), EMCare (Nursing and Allied Health), Health Management Information Consortium (HMIC), Medline, PsycINFO, PubMed and Cochrane (searched separately). Search tools used: Boolean operators (and, or); truncation (*); Ti,ab=searches title and abstract. HGSC, high grade serous ovarian cancer; EOC, epithelial ovarian cancer.
Results
The resulting 29 primary research papers investigated the prevalence of psychosexual morbidity in over 4116 women with epithelial ovarian cancer (see Online supplemental tables 1–3). Only five of the 29 studies (17.2%) used healthy control groups.12–16 With such a lack of comparison groups, quantifying how much psychosexual morbidity is directly attributable to epithelial ovarian cancer cannot be decisively answered. Furthermore, studies applied variable timepoints during a woman’s cancer journey at which they assessed her sexual function, with some studies assessing at multiple consecutive time-points which complicated result synthesis.
Unfortunately, there was no agreed definition of clinically significant psychosexual morbidity and studies measured different aspects. It was consequently difficult to estimate the overall published prevalence of clinically significant psychosexual morbidity, such as sexual dysfunction affecting quality of life and relationships. Over a third of the 29 studies (34.5%) reported the proportion of sexually active women with epithelial ovarian cancer which ranged from 9% to 65%.13 16–24 When compared with a healthy population, women with epithelial ovarian cancer were less sexually active (47% vs 53%, respectively).16 The questionnaires used were not always appropriate for the sexual activity status. As an example, the Female Sexual Function Index is designed for women who have had sex in the past month but was inappropriately used in sexually inactive cohorts.21 22 Furthermore, many tools relied on self-reported retrospective measures inherently at risk of recall bias. Most study populations sampled a predominantly white, heterosexual, married population of women with epithelial ovarian cancer, limiting wider applicability.
A likely factor contributing to reduced sexual activity in women with epithelial ovarian cancer is the higher levels of sexual distress compared with published general population values (18% vs 12%, respectively).25 Questionnaires were able to separate sexual distress into distinct categories. The only quality of life questionnaire specifically validated for women with epithelial ovarian cancer is the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire for Ovarian Cancer (EORTC QLQ-OV28). However, the Female Sexual Function Index and Sexual Activity Questionnaire are validated for female cancer patients.26 27 Numerous data collection methods and tools were used (Online supplemental table 3), which confounded comparisons between studies and data synthesis. Of the 29 studies, 26 used questionnaires to assess sexual functioning: most commonly the EORTC-QLQ OV28 (46.2%), followed by the cancer generic EORTC-QLQ C30 (38.4%), Female Sexual Function Index (23.1%), Female Sexual Distress Scale (7.7%), and Sexual Activity Questionnaire (7.7%). Non-validated questionnaires designed by their authors featured in five of the 29 studies, further complicating data interpretation. With an aim to facilitate identification and management of psychosexual morbidity in women with epithelial ovarian cancer, common themes which emerged from the literature will be discussed in the following sections: (1) Patient characteristics as potential risk factors; (2) Presenting symptoms; (3) Intimate relationships; followed by recommendations for interventions and future research.
Patient Characteristics
Patient characteristics commonly cited in the literature to be associated with psychosexual morbidity in women with epithelial ovarian cancer included: younger age (<53 years); pre-menopausal status at diagnosis; cardiovascular co-morbidities including anxiety and depression; aim of treatment; extent of surgery; and having received more courses of chemotherapy.
Age
Age was heterogeneously recorded: some studies cited age at diagnosis (ranging from 48.3 to 63 years),16 24 28 while others cited age at interview or survey,16 24 mean age,6 18–20 29–31 median age,12 17 25 32 or modal age.33 Age thresholds for categorizing younger versus older patients varied above or below 48 years,34 53 years,16 62 years,20 or 65 years.35 This inconsistency loses the distinction of women who have undergone a pre-menopausal hysterectomy and salpingo-oophorectomy being in the younger cohort, confounding interpretation of the results. Only one study considered menopausal age with their age threshold of 53 years, approximately the age of the natural menopause.16 Reduced sexual functioning due to younger age was reported by four of the 29 studies,16 19 24 34 alongside diminished sexual pleasure.16 This may reflect the fact that younger patients are more likely to undergo a surgically-induced menopause with a more profound drop in circulating estrogen. Conversely, a minority of studies found no difference in sexual activity or functioning with age.19 36 This inconsistency may indicate heterogenous study design across the results with varying age thresholds and failing to comprehensively document other relevant issues such as extent of surgery. Future work should incorporate an age threshold of 53 years for sub-group analysis, documentation of pre-treatment menopausal status, and extent of treatment.
Co-Morbidities
Co-morbidities including increased cardiovascular risk, sedentary lifestyle, physical problems, anxiety and depression were found to affect psychosexual morbidity in six studies, yet none investigated how treatment of such co-morbidities might improve sexual function.16 23 25 28–30 Cardiovascular co-morbidities significantly worsen sexual dysfunction.30 Sedentary behavior was also associated with worse quality of life including sexual functioning (p=0.001) and body image (p=0.018).28 30 Interestingly, diabetes was not mentioned in the literature despite its potential to affect sexual functioning, given its role in autonomic neuropathy. It was not possible to discern the temporality of such co-morbidities in women with epithelial ovarian cancer (pre-cancerous co-morbidities were not reported). Depression rates were higher in women with epithelial ovarian cancer than those published for the general population, and depression correlated with sexual problems in patients and their partners.25 37 Over half of women with epithelial ovarian cancer are at risk of clinically significant anxiety and over a third are vulnerable to depression (compared with 19.8% depression prevalence in the general public).25 29 In particular, younger women with epithelial ovarian cancer with relationship concerns are particularly vulnerable to anxiety (p<0.05),29 and anxiety and fear are associated with pain during sex (dyspareunia) leading to reduced intimate touching.25 Unfortunately, no study evaluated how treatment of such anxiety and depression might improve psychosexual morbidity. As global quality of life may decline with co-morbidities or sedentary lifestyle, psychosexual dysfunction may increase indirectly; distinguishing the effect of co-morbidities on psychosexual dysfunction from their effect on global quality of life would require a detailed regression analysis.
Treatment
In the review, 14 of the 29 studies considered how the treatment that a patient receives during her cancer journey appears to affect sexual function. Primary surgery including hysterectomy and bilateral oophorectomy precedes a significant deterioration in body image and attitude towards the disease, which is then significantly compounded by chemotherapy-associated symptoms (p<0.05).34 Extent of surgery influences the degree of psychosexual morbidity in women with epithelial ovarian cancer: women who underwent lymphadenectomy reported impaired orgasm at 12 months compared with baseline, whereas those who did not undergo lymphadenectomy described an improvement (p=0.02).21 Women with early stage disease may undergo lymphadenectomy for staging and are more likely to live longer as women with epithelial ovarian cancer. Thus, such women will require adequate counseling and enquiry about sexual problems for at least a year following surgery. More chemotherapy cycles are associated with psychosexual morbidity (p<0.001).17 A threshold figure for the number of cycles of chemotherapy required to place a woman at significantly increased risk of psychosexual morbidity is not possible to ascertain from the published data presented but is recommended for future research.
Stage
Surprisingly, the relationship between the stage of disease and psychosexual dysfunction is unclear. This may be because of the number of confounding factors such as age, as younger patients tend to have earlier stage disease, menopausal symptoms and differences in treatment. Tolerance of side effects may vary depending on aim of treatment, which inherently depends on stage of disease: 61% of women with ovarian cancer were willing to tolerate sexual side effects if the goal of treatment was cure, but 55% if aiming for disease stabilization (p=0.070).33 Only nine of the 29 studies reflected on the aim of treatment. Future studies and clinicians should routinely enquire about the tolerability and acceptability of psychosexual symptoms in patients with different disease stages and at different points along their treatment journey.
Presenting Symptoms
Sexual dysfunction was cited to be a priority of women with epithelial ovarian cancer in eight studies.19 31–33 35 38–40 Regarding priority symptoms, psychosexual morbidity was the second most commonly patient-reported symptom following chemotherapy-induced peripheral neuropathy,39 and 58% reported sex to be very or somewhat important.19 Common symptoms evident across the literature exploring psychosexual morbidity in women with epithelial ovarian cancer included: vaginal dryness; reduced ability to orgasm; reduced sexual pleasure; and worse perceived body image.
Reduced Sexual Activity
Compared with age-adjusted healthy controls, fewer women with epithelial ovarian cancer were sexually active (47% vs 53%, respectively) and those who were sexually active reported lower levels of sexual pleasure (p<0.001) and higher levels of sexual discomfort (p<0.001).16 Up to three quarters (63–75%) of women reported negative changes in their sex life following diagnosis, especially after multiple recurrences.18 19 Possible explanations for reduced sexual activity and quality in women with epithelial ovarian cancer include: vaginal dryness (87%); dyspareunia (77%); reduced sexual interest (51%); physical problems preventing sex (36%); and fatigue (18%).19 Common barriers to sexual activity in women with ovarian cancer are further examined below.
Vaginal dryness and dyspareunia were often reported together and discussed by 13 of the 29 (45%) studies.12–14 16–21 23–25 36 When prevalence was documented, vaginal dryness affected 81–87% of sexually active women with epithelial ovarian cancer,19 20 with significant intensity in up to a quarter.20 Dyspareunia affected up to 77% of women with ovarian cancer,19 worsening from diagnosis24 25 and with longer survival.12 21 Although one study (n=47) found menopausal symptoms comparable between women with ovarian cancer and healthy women,23 women who had undergone pre-menopausal oophorectomy were found to have higher levels of sexual discomfort (p<0.001).16 Similarly, greater sexual discomfort in sexually active women with ovarian cancer was associated with both lower serum levels of estradiol (p=0.02) and higher levels of sex hormone binding globulin (p=0.04).16
Reduced sexual desire, interest and arousal were described as reduced in seven studies (24.1%),6 12 16 19 20 24 25 except in one which reported these as similar to healthy women.13 Lack of sexual interest increased with epithelial ovarian cancer diagnosis from 33% to 61% (54% attributed to epithelial ovarian cancer)24 and elsewhere reduced sexual interest ranged widely (31–90%).6 16 19 20 Psychological factors play a role alongside physical and hormonal barriers in sexual dysfunction. A lack of interest or desire for sex is described to affect over a third of women with epithelial ovarian cancer (36–43%) and more commonly than age-adjusted controls.16 19 Lack of satisfaction was described in 21% of women with epithelial ovarian cancer.19 Psychological (such as talking therapies) and physical interventions (such as vaginal lubricants) which have aimed to address these symptoms are discussed later.
Reduced sexual enjoyment and ability to orgasm were discussed by seven studies,12 13 16 18 21 24 25 with orgasm worse in long-term survivors12 and at 1 year post lymph node resection.21 Up to two-thirds of women with epithelial ovarian cancer described reduced sexual satisfaction (21–66.7%)18 19 and nearly half (29–47%) felt less satisfied since treatment.41 Interestingly, the possibility of chemotherapy-induced autonomic neuropathy contributing to impaired orgasm was not mentioned in these studies, although previously mentioned in an expert review by Whicker et al.5
Body image was discussed in 10 studies. Difficulties with altered body image affected one-third to more than half of women with epithelial ovarian cancer,22 41 with up to two-thirds feeling less sexually attractive since diagnosis.22 24 Body image changes were associated with psychosexual morbidity,6 16 sedentary behavior,28 younger age,34 and more time since chemotherapy ended.20
Intimate Relationships
Intimate relationships were mentioned in 13 studies, with evidence of an impaired relationship or reduced enjoyment of intimacy.22 25 36 Two-thirds of women with epithelial ovarian cancer were dissatisfied with their sex life.18 Common reasons reported for sexual inactivity included: lack of interest in sex (51%); having no partner (35%); and their partner not being interested in sex (16%).19 Conversely, two studies described similar or improved intimate relationships.18 41 Regardless of sexual function, most women (75–81.5%) reported feeling close to their partners18 and that their partners were 'supportive and tender'.41 Therefore, the interplay between psychosexual dysfunction and intimate relationships requires clarification, but evidence suggests this area could be improved for some women with epithelial ovarian cancer.
Interventions addressing psychosexual concerns in a cancer setting typically adopt physical, biochemical, and psychological approaches. Intervention papers from the literature search were limited to psychoeducational approaches (see Online supplemental table 3). Unfortunately, the review did not identify any intervention studies that incorporated common approaches to alleviate symptoms that are familiar to most clinicians such as hormone replacement therapy, antidepressants, pelvic floor physiotherapy, dilators, or even vaginal lubricants and moisturizers which have been applied in gynecological cancer settings.5 This may reflect the search design despite covering multiple databases, or the lack of such studies in women with epithelial ovarian cancer specifically.
Discussion
Psychosexual morbidity remains one of the most important issues for women with epithelial ovarian cancer, yet it is not being detected and managed adequately. Despite being a priority for patients19 and associated with reduced quality of life,18 24 psychosexual symptoms are not documented in patient notes by clinicians.40 Failure to document psychosexual morbidity may reflect lack of recognition or acknowledgment of sexual problems, thus reducing the likelihood these issues will be addressed. Patients would like clinicians to broach the topic of psychosexual morbidity.10 42 Often called ‘permission giving’, this relates to the patient’s perceived hierarchy of concerns. A barrier to discussing sexual issues may be the patient’s perception that it is more acceptable to discuss non-sexual medical issues and that the clinician may be better equipped to deal with the latter.11 However, women with epithelial ovarian cancer are at increased risk of psychosexual morbidity compared with healthy women, following diagnosis and at several stages along their cancer journey,12 17 41 emphasizing that sexual problems should be discussed clinically.
The literature reviewed here is heterogeneous in terms of questionnaires, data quality, age thresholds, and outcomes. Further, there is no consensus on frequency of follow-up assessments. Given these caveats, firm conclusions are difficult to draw but, overall, we estimate that as up to 75% of women with epithelial ovarian cancer report negative changes in their sex lives following diagnosis18 19 and, of those sexually active, vaginal dryness affects 81–87% and pain 77%,19 20 approximately 75% of women with epithelial ovarian cancer will incur clinically significant psychosexual morbidity. The most common symptoms include vaginal dryness, dyspareunia, reduced sexual desire and activity, impaired orgasm, diminished perceived body image, and reduced partner intimacy.
Unaddressed psychosexual concerns contribute to negative relationship changes in partnerships affected by cancer.8 43 One possible explanation for reduced sexual activity during treatment, which remained unexplored in these studies, is that some patients and partners are concerned that cancer or chemotherapy can be sexually transmitted.44 Additionally, pain in the patient may make the partner reluctant to engage in sexual activity.45 However, partners’ perceptions were largely lacking from the results of this literature search. Furthermore, female gender is a strong predictor of partner abandonment in patients with serious medical illness.43 Therefore, clinicians are encouraged to consider and incorporate partners in consultations and research.
Due to the heterogeneous quality of the studies, it remains difficult to conclusively define the risk factors that predict psychosexual morbidity in women with epithelial ovarian cancer. However, the most prevalent factors to consider include younger age (less than 53 years),16 which may reflect a surgically-induced menopause, co-existing cardiovascular conditions that are associated with a more sedentary life style, anxiety, and depression. The treatment for epithelial ovarian cancer, which consists of surgery to remove the uterus and ovaries followed by chemotherapy, also contributes to psychosexual morbidity. Critical points in cancer treatment may correlate with particularly poor sexual function. Domenici et al found that worse menopause-related symptoms, body image, and attitude toward the disease occurred during first-line chemotherapy and poorer body image, attitude toward the disease and chemotherapy-associated symptoms occurred after the primary surgery.34 Such time-points may prove useful in identifying early psychosexual morbidity in women with epithelial ovarian cancer, thereby minimizing distress. Assessment of sexual concerns should therefore be an important part of the end of treatment assessment of patients, particularly as they enter the follow-up period when they are seen much less frequently.
Several factors contribute to psychosexual morbidity including treatment, physical and psychological co-morbidities which may precede diagnosis, and hormonal changes. Some of these factors are amenable to treatment. For instance, it is important for clinicians to assess anxiety and depression as these can be treated through psychological measures and antidepressants.5 Psychological therapies (such as cognitive behavioral therapy) may help to tackle body image difficulties, especially in younger women in whom body image is worse34 and relationship concerns predict anxiety risk.29 Vaginal lubricants provide a simple mechanical intervention to alleviate dyspareunia from vaginal dryness and vaginal moisturizers can improve long-term tissue health (also reducing systemic absorption of local hormonal treatments from the vaginal epithelium).5
The reduction in estrogen that occurs through surgically-induced menopause has a significant effect on psychosexual dysfunction. Unsurprisingly, lower circulating estradiol levels are associated with greater sexual problems in women with epithelial ovarian cancer.16 We know that estrogen therapy is in general safe in patients with epithelial ovarian cancer; Hopkins et al, showed in their systematic review that hormone replacement therapy can and should be considered in women with epithelial ovarian cancer who exhibit troublesome menopausal symptomatology,46 and data from an ongoing Cochrane review looks promising.47 Moreover, hormone replacement therapy does not influence the recurrence rate in epithelial ovarian cancer.48 Therefore, hormone replacement to physiological levels may be beneficial in mitigating the contribution of oophorectomy to psychosexual morbidity. However, there may be reluctance to prescribe hormonal treatments in a gynecological cancer setting if the patient carries a germline BRCA gene mutation, has previous estrogen receptor-positive breast cancer, or if unsure of hormone receptor status of the tumor. Previous data have shown that hormone replacement does not address psychosexual morbidity completely and additional support through nurse-led interventions is important.
This review has highlighted significant heterogeneity between studies, which confounds interpretation and therefore recommendations. As some questionnaires were not validated and sometimes developed only for the cited publication, there is a critical need for the community to define a core set of questionnaires and parameters on which to focus. The only validated questionnaire is the EORTC QLQ-OV28, which has been developed for women with epithelial ovarian cancer. Validated questionnaires to assess psychosexual morbidity in the population include the Female Sexual Function Index and Sexual Activity Questionnaire. Future studies should capture key demographic information such as age and menopausal status but otherwise focus on these validated questionnaires. Clearly it will be important to assess psychosexual morbidity over time, and therefore there is a trade-off to consider between the depth (the number of questionnaires at any point) and the breadth (the frequency of assessing psychosexual morbidity) that needs to be considered if we are to assimilate high quality data sets from which our patients can best be managed. However, for now the most important change we can make for our patients is enquiring about their symptoms of psychosexual morbidity.
Recommendations for Future Research and Practice
A stronger consensus is required regarding definitions relating to psychosexual morbidity in women with epithelial ovarian cancer, outcome measure tools chosen (such as questionnaires), and age thresholds (such as older vs younger patients). Consideration of partners in assessing and managing sexual problems is beneficial and required, given their role in supporting women and to minimize anxiety and depression. Promising areas which warrant further exploration include: clinician and patient tools to broach the topic; questionnaire optimization; patient education and empowerment initiatives; and interventions to tackle the potential risk factors highlighted here, such as increasing physical activity and improving mental health. It is hoped that increasing recognition and consideration of psychosexual morbidity in women with epithelial ovarian cancer will optimize quality of life in this patient group.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @logue_chloe
Contributors CAL and JP contributed equally to this paper. CAL is a junior doctor who was undertaking an academic Foundation programme at the Christie Cancer Hospital in medical gynaecological oncology. JP is a Macmillan nurse specializing in psychosexual therapy at the Christie Cancer Hospital. Together, CAL and JP conducted the literature search, data collection, analysis and write up of this review, supervised in the field of gynecological oncology by GJ.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.