Article Text

Abstract
Background The impact of blood transfusion on ovarian cancer survival is uncertain.
Objective To investigate whether peri-operative blood transfusion negatively impacted progression-free survival, overall survival, and quality of life in patients with advanced ovarian cancer.
Methods We performed an ancillary analysis of the European Organization for Research and Treatment (EORTC) 55971 phase III trial, in which patients were randomized to primary debulking surgery versus neoadjuvant chemotherapy. Patients included in the per-protocol analysis were categorized by receipt of a transfusion.
Results 612 of 632 (97%) of patients had adequate data for analysis. Of those, 323 (53%) received a transfusion. The transfusion cohort was more likely to have had better Word Health Organization (WHO) performance status, serous histology, undergone primary debulking surgery, and received more aggressive surgery, with higher rates of no gross residual disease. Median overall survival was 34.0 vs 35.2 months in the no transfusion and transfusion cohorts (p=0.97). The adjusted HR for death was 1.18 (95% CI 0.94 to 1.48) in favor of the transfusion cohort. Median progression-free survival was 13.6 vs 12.6 months in the no transfusion and transfusion cohorts (p=0.96). The adjusted HR for progression was 1.14 (95% CI 0.91 to 1.43). There were no significant differences in global quality of life, fatigue, dyspnea, or physical functioning between the two cohorts at baseline or at any of the four assessment times. Grade 3 and 4 surgical site infections were more common in the transfusion cohort.
Conclusion Transfusion did not negatively impact progression-free survival or overall survival; however, it was associated with increased peri-operative morbidity without improvements in quality of life.
- Ovarian Neoplasms
- Surgery
Data availability statement
Data are available upon reasonable request.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
The prevalence of peri-operative blood transfusion after cytoreductive surgery for ovarian cancer is high. Red blood cell transfusions are used in the peri-operative setting to improve oxygen delivery to tissues and ameliorate symptoms of anemia. Unfortunately, blood transfusions are not without complications, and several studies have suggested that blood transfusions are immunosuppressive and associated with increased peri-operative morbidity, mortality, and cancer recurrence.
WHAT THIS STUDY ADD
To our knowledge, this is the first ancillary study of a large randomized trial evaluating the impact of transfusion on progression-free survival, overall survival, quality of life, and peri-operative outcomes in ovarian cancer. Our study demonstrates peri-operative transfusions are associated with increased peri-operative morbidity without impact on progression-free survival, overall survival, or improvement in quality of life. Our findings contribute to the growing wealth of information questioning the benefit of peri-operative transfusion.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Future research could potentially focus on peri-operative optimization to decrease the need for intra-operative blood transfusions, examination of variability in surgeon practice, and/or consideration of implementation of more restrictive blood transfusion policies. Considering the global blood transfusion shortages that have occurred since the COVID-19 pandemic, surgeons have had to be more judicious with blood products. Evaluation of blood transfusion practices post-COVID-19 could be warranted.
INTRODUCTION
The cornerstone of treatment of metastatic advanced stage ovarian cancer includes a combination of surgery and cytotoxic chemotherapy. The surgical complexity of cytoreductive surgery places patients with ovarian cancer at high risk for receiving a peri-operative blood transfusion, with rates ranging from 42% to 77%.1–3 Although operative blood loss is a clear source of peri-operative anemia, patients with advanced ovarian cancer are also at risk for anemia secondary to chronic disease, nutritional deficiencies, and myelosuppressive effects of chemotherapy, each of which contribute to high transfusion rates.4
Transfusions are used in the peri-operative setting to improve oxygen delivery to tissues and ameliorate symptoms of anemia. Unfortunately, blood transfusions are not without complications and several studies have suggested that transfusions are immunosuppressive and associated with increased peri-operative morbidity, mortality, and cancer recurrence.3 5–7 Despite the plethora of evidence supporting restrictive blood use in other diseases, the data assessing the impact of blood transfusion in ovarian cancer are limited.8 9 To date, only a few studies have evaluated the impact of transfusion on progression-free survival or overall survival in patients with ovarian cancer. Most studies have been single-institution, retrospective studies yielding mixed results, with one meta-analysis suggesting that blood transfusion is not an independent risk factor for survival.1 2 10–16 To our knowledge no studies have evaluated quality of life in patients with gynecologic cancer after transfusion.
Given the high incidence of transfusion in patients with ovarian cancer, it is prudent to evaluate the clinical benefits of transfusion and identify potential deleterious clinical outcomes.17 We performed a secondary analysis of the European Organization for Research and Treatment of Cancer (EORTC) Gynecological Cancer Group trial, in which patients were randomized to primary debulking surgery versus neoadjuvant chemotherapy followed by interval debulking surgery to investigate the impact of peri-operative blood transfusion on progression-free survival, overall survival, and quality of life in patients with advanced ovarian cancer. We hypothesized that peri-operative transfusion would be associated with improved quality of life without impact on progression-free survival or overall survival.
METHODS
The EORTC 55971 (ClinicalTrials.gov number: NCT00003636) trial design, eligibility criteria, and outcomes have been previously published.18 19 There were 632 patients included in the per-protocol analysis. In this ancillary data analysis, patients included in the per-protocol analysis were categorized by receipt of a peri-operative blood transfusion. Peri-operative blood transfusion was defined as intra-operative or post-operative transfusion within 28 days of surgery. The decision to transfuse was based on provider discretion and not part of the original protocol for peri-operative management. The outcomes of interest were overall survival, progression-free survival, quality of life, and peri-operative adverse events. Overall survival was defined as the time from randomization to death from any cause. Patients alive at last follow-up were censored on the date of last follow-up. Progression-free survival was defined as the time from randomization to documented progressive disease or death. Patients without documented progressive disease were censored on the date of last assessment for progressive disease. Quality of life was assessed using the psychometrically validated EORTC QLQ-C30 questionnaire version 3.0.20 Patients completed the questionnaire at baseline, before the third and sixth cycles of chemotherapy, and at 6 and 12 months of follow-up.
Descriptive statistics summarized demographic and clinical characteristics of patients in the transfusion and no transfusion cohorts. Χ2 or Fisher’s exact test were used to test for differences between categorical variables, and Mann-Whitney test to compare medians between cohorts for continuous variables. Cox proportional hazards regression modeled overall survival as a function of potential prognostic factors while adjusting for treatment arm and transfusion cohort.21 Hazard ratios are reported by their respective confidence intervals. A multivariable analysis of overall survival was constructed by first building a saturated model including treatment arm, transfusion cohort, and all factors with a p value <0.20. Backward elimination was used by removing factors with a p value <0.05, to construct a parsimonious model for overall survival while retaining treatment arm and transfusion cohorts. The product-limit estimator of Kaplan and Meier was used to illustrate overall survival for various cohorts of interest. Progression-free survival was similarly analyzed.22 The quality-of-life analysis methodology has been previously reported.20 23
This study was reviewed by the MD Anderson institutional review board and found to be exempt. In accordance with the journal’s guidelines, we will provide our data for independent analysis by a selected team from the editorial team for the purposes of additional data analysis or for the reproducibility of this study in other centers if such is requested.
RESULTS
Between September 1998 and December 2006, 670 patients with stage IIIC or IV ovarian cancer were randomized to primary debulking surgery or neoadjuvant chemotherapy on trial. Of these, 38 were ineligible or did not start allocated treatment, and a further 20 patients were excluded from our ancillary status because of missing intra-operative transfusion data. A comparison of the baseline characteristics between the no transfusion and transfusion cohorts is given in Table 1 and a comparison of the operative characteristics between the two cohorts is listed in Table 2. There was no difference in age, body mass index, histologic grade, stage, or location of primary tumor between the cohorts. The transfusion cohort was more likely to have had better WHO performance status, serous histology, undergone primary debulking surgery, and received more aggressive surgery, with higher rates of no gross residual disease.
Baseline characteristics
Operative characteristics
Of the 612 patients included in our analysis, 323 (53%) received an intra-operative blood transfusion. Eighty-two (13%) patients received a post-operative transfusion. Of note, all patients who received a post-operative transfusion also received an intra-operative transfusion. Transfusion was more common in the primary debulking surgery cohort (n=174 (54%) vs 149 (46%), p=0.01). Transfusion rates among participating countries that entered five more patients were highly variable, ranging from 17% to 91% (median: 46%, IQR 31–62). These data are not shown in the tables provided.
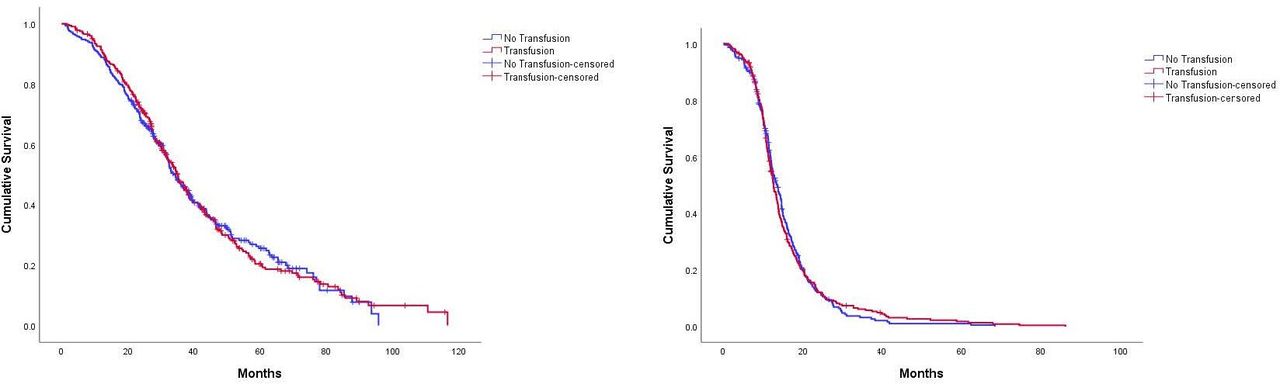
There was no difference in overall survival in the no transfusion compared with transfusion cohort. Median overall survival was 34.0 (95% CI 31.1 to 37.0) vs 35.2 (95% CI 32.1 to 38.4) months, respectively (p=0.97). Similarly, there was no difference in progression-free survival in the no transfusion compared with transfusion cohort. The median progression-free survival was 13.6 months (95% CI 12.2 to 14.9) vs 12.6 months (95% CI 11.7 to 13.5), respectively (p=0.96). In the multivariable analysis adjusting for stage, country, treatment arm, residual disease, performance status, histology, grade, stage, age, body mass index, primary disease site, and operating time there was no difference in overall survival (HR=1.18, 95% CI 0.94 to 1.48, p=0.15) or progression-free survival (HR=1.14, 95% CI 0.91 to 1.43, p=0.24). (Online supplemental table 2). Twelve patients were noted to have a post-operative hemorrhage; however, confirmation of associated transfusion could not be confirmed. Thus, these patients were included in the no transfusion cohort for the purposes of the primary analysis. A sensitivity analysis was performed including these patients in the transfusion cohort with no significant impact on magnitude of effect or statistical significance.
As previously noted, we observed a significant difference in size of residual tumor in the transfusion compared with no transfusion cohort, with 26% of patients having no residual disease in the no transfusion cohort compared with 42% of patients having no residual disease in the transfusion cohort. In the original manuscript,19 complete cytoreductive resection to no gross residual disease was the strongest predictor of overall survival. Since there were remarkable differences in oncologic outcomes based on residual disease and significant differences in our transfusion and no transfusion cohorts, we performed subgroup univariable and multivariable analysis based on the presence of residual disease. There was no difference in overall survival or progression-free survival in the transfusion compared with no transfusion cohort for patients who had residual disease after their cytoreductive surgery (HR=1.15, 95% CI 0.86 to 1.54, p=0.34) and HR=1.22, 95% CI 0.92 to 1.61, p=0.16, respectively) (Figure 1). For patients who had an optimal tumor reductive surgery to those with no gross residual disease, the univariable analysis of transfusion was associated with worse overall survival (HR=1.77, 95% CI 1.21 to 2.58, p=0.003); however, this difference did not persist in the multivariable analysis (HR=1.50, 95% CI 0.95 to 2.36, p=0.08). Online supplemental table 2
Supplemental material
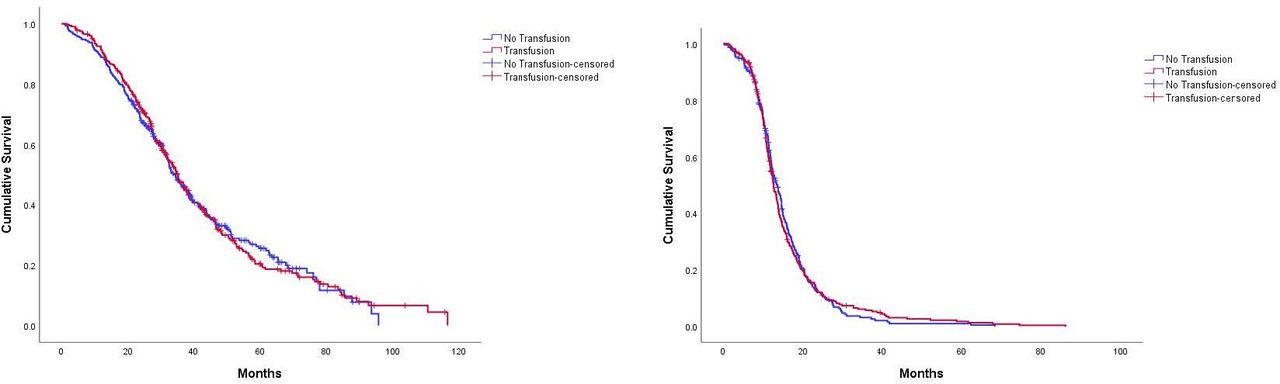
Kaplan-Meier estimates of the probably of (A)overall survival and (B)progression-free survival according to transfusion status. There was no difference in overall or progression-free survival between the two cohorts.
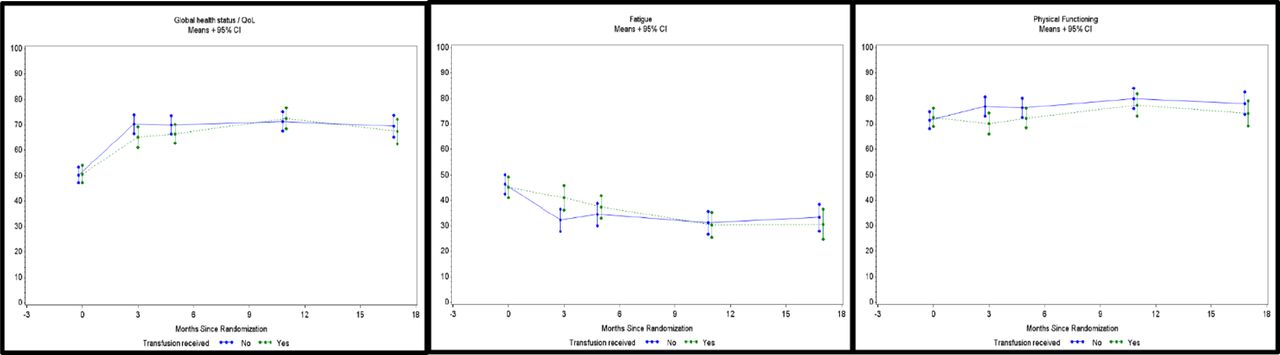
The mean and SD of the EORTC QLQ-C30 scales by transfusion cohort and assessment time are displayed in Online supplemental table 1). There were no statistically significant differences between the cohorts in any of the quality-of-life functioning or symptom scales. Specifically, there were no significant differences in global quality of life, fatigue, dyspnea, or physical functioning between the two cohorts at baseline, or at any of the four subsequent assessment times (Figure 2).
Supplemental material
{kind=link}
{kind=link}
European Organization for Research and Treatment Cohort QLQ-C30 symptom scores by transfusion status. High scores indicate higher levels of symptoms.
Peri-operative complications within 28 days of surgery are depicted in Table 3. Grade 3 and 4 complications were more common in the transfusion cohort than in the no transfusion cohort. Specifically, grade 3 and 4 surgical sites infections were more common in the transfusion cohort than in the no transfusion cohort (n=25 (8%) vs 4 (2%), p<0.001). Grades 3 and 4 dysrhythmia were more common in the transfusion cohort than in the no transfusion (n=9 (3%) vs 1 (0.3%), p=0.048). As expected, grade 3 and 4 hemorrhage was more common in the transfusion cohort than in the no transfusion cohort (n=32 (10%) vs 3 (1%), p<0.001). There were no differences in grades 3 and 4 venous thromboembolism events between the two cohorts (n=1 (0.4%) vs 7 (2%), p=0.083). There were no post-operative deaths in either of the two cohorts within 28 days of surgery.
Peri-operative complications within 28 days of surgery
DISCUSSION
Summary of Main Results
We demonstrated that patients with advanced stage ovarian cancer are at high risk of receiving a blood transfusion, with 53% of participants having received a peri-operative blood transfusion. Blood transfusions do not appear to be associated with changes in progression-free survival or overall survival; however, they are associated with increased peri-operative morbidity without improvements in quality of life.
Results in the Context of Published Literature
To our knowledge, this is the first ancillary study of a large, randomized trial evaluating the impact of transfusion on progression-free survival, overall survival, quality of life and peri-operative outcomes in ovarian cancer. Only eight single institution retrospective studies have evaluated the impact of transfusion on progression-free survival or overall survival in patients with ovarian cancer, yielding discordant results.1 2 10 12–15 McGehee et al were the first to evaluate the effect of blood transfusion in patients with ovarian cancer. They noted that transfusion was associated with decreased overall survival and progression-free survival; however, their study was inclusive of all gynecologic cancers with only 28 patients with ovarian cancer. No subgroup analysis by tumor type was performed, thus limiting interpretation of their study.14 De Oliveira et al, evaluated the impact of peri-operative transfusion in optimally cytoreduced ovarian cancer. The authors demonstrated that transfusion was associated with a reduction in progression-free survival and overall survival after adjustment for age and tumor grade.1 Altman et al evaluated the impact of peri-operative, as well as peri-chemotherapy transfusion in patients with advanced ovarian cancer and noted that overall transfusion was a negative prognostic indicator for progression-free survival, but not overall survival with an adjusted HR of 1.06 (95% CI 1.01 to 1.11) for progression-free survival. When the peri-operative period was evaluated independently, there was no impact on survival.12 Zhang et al identified 1037 patients undergoing primary debulking surgery and found increased incidence of post-operative complications, length of stay, readmission, with decreased overall survival and disease-free survival.24 Connor et al reported that peri-operative transfusion was also associated with decreased overall survival.10
However, the following studies showed no difference in progression-free survival or overall survival based on receipt of transfusion: Warner et al, Abu-Rustum et al, and Hunsicker et al.2 13 15 Pergialiotis et al performed a meta-analysis using seven of the eight previously mentioned single institution studies and noted that when using propensity score matching and multivariable analysis, transfusion was not an independent risk factor for negative survival outcomes.11
Our data confirm the findings of the negative trials and suggest that peri-operative transfusion is not associated with decreased survival metrics. However, our data appear to contradict the findings from studies of other tumor types, including colorectal and lung cancer, which support worse oncologic outcomes after transfusion.7 25 26 There are several possible explanations for the mixed results. First, most studies use different definitions of peri-operative transfusion, which ranges from 72 hours after surgery to 1 month after surgery. Second, blood management studies suggest that not all blood is created and stored equally and that variations in blood storage and processing, such as age, leukocyte reduction, and blood type, may be confounding factors that impact the outcomes of the aforementioned studies.4 Blood storage and processing details are not often collected or reported in many published studies and likewise were not available for our ancillary analysis. Our results are consistent with previously published studies that demonstrate that transfusion is associated with worse peri-operative outcomes.2 9 27 28 We noted an increased incidence of surgical site infections, dysrhythmias, and hemorrhage. We found no difference in the incidence of venous thromboembolism; however, our study was underpowered to detect this difference, given the low incidence of venous thromboembolism in this study (1.3%).
The proposed mechanism of transfusion-associated adverse events has been attributed to alterations in the immune system termed ‘transfusion-related immunomodulation.’29 This concept was initially derived from observations that renal transplant recipients who received blood transfusions had improved allograft survival. Animal models have been used to investigate the mechanism of action of immunomodulation and have shown that blood transfusions can suppress natural killer cell activity, induce suppressor T cells, decrease function of macrophages, and alter antigen presentation.29 30 It has been postulated that these cellular changes may be the underlying mechanism for the adverse clinical effects of increased infection, venous thromboembolism, cancer recurrence, and mortality seen in previous studies. Additional work is needed in this area to fully understand the impact of transfusion in humans and the tumor microenvironment. Current studies collecting tissue specimens pre-operatively and post-operatively are ideal for evaluating the impact of transfusion on the tumor microenvironment.
Transfusions are often used in the peri-operative setting to immediately ameliorate signs and symptoms of anemia and are often justified by the perceived benefit of this intervention. Our quality-of-life data suggest, however, that transfusions are not associated with improvement in global quality of life, fatigue, dyspnea, or physical functioning between the two cohorts at baseline or at any of the four assessment times. This might be because the effect of transfusion on quality of life is shorter than the assessment period or because transfusion itself is not as effective at dealing with symptoms that are multifactorial, from underlying malignancy, surgery, or cytotoxic therapy. Given that quality of life was collected at cycles 3 and 6 it is possible that a post-surgery benefit of transfusion might have been overpowered by the toxicities related to chemotherapy.
Interestingly, we also identified high variability of transfusion practices among countries participating in the EORTC trial. This is consistent with previous studies that have evaluated the prevalence of anemia and use of transfusion in oncologic patients.31 32 Procedures or interventions with high degrees of variation and variability indicate areas of opportunity to reduce costs and improve healthcare delivery. Such procedures often indicate either a lack of implementation of evidence-based guidelines, or a deficiency of evidence, or both. Awareness of transfusion rates and understanding the benefits and risks of transfusion is essential to maximize the clinical benefit of transfusing practices. Several randomized clinical trials have challenged the clinical dogma that liberal transfusion practices are beneficial and, as a result, widespread adoption of more restrictive transfusion practices has slowly infiltrated most clinical specialties.5 6 33–36 Oncologists have been slower to change practice, confirmed by the high degree of variation in transfusion practices.
Strengths and Limitations
Strengths of our study include use of a large randomized trial to evaluate the impact of transfusion on progression-free survival, overall survival, quality of life, and peri-operative outcomes in ovarian cancer. Given that this was a secondary analysis of an international multicenter randomized control trial, we would anticipate high external validity. Our study has several limitations. First, this was an unplanned secondary analysis of a previously conducted randomized trial. As such, the design of the trial, including choice of endpoints and sample size was determined by its original primary objective. Second, we were limited to the variables that were previously collected and therefore do not have some variables that would be of interest, such as estimated blood loss, number and quantity of transfusions, hemoglobin levels, reason for transfusion, or receipt of anticoagulation. Third, as noted in the original manuscript on quality of life, the results from the quality-of-life endpoints were mostly derived from a selected number of institutions with better quality-of-life compliance.18 Fourth, although there was an association between transfusion and peri-operative morbidity, transfusion was more common in patients undergoing primary debulking surgery with more aggressive surgery so causative relationship cannot be assumed. We performed a multivariable analysis including presence of residual disease and operative time as a surrogate marker for surgical complexity but did not include surgical complexity as an independent variable. Finally, transfusion data were self-reported by individual institutions, therefore it is possible that the transfusion data captured in the EORTC study was under-reported or misreported.
Implications for Practice and Future Research
Given the association with increased peri-operative risk and lack of improvement in quality of life, our findings contribute to the growing wealth of information questioning the overuse of transfusions. Our data are hypothesis-generating and thought-provoking about the potential overuse of transfusions without clear benefit and potential for harm.
Conclusions
We demonstrate that overall blood transfusions do not appear to be associated with changes in progression-free survival or overall survival; however, they are associated with increased peri-operative morbidity without improvements in quality of life.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Acknowledgments
The authors thank the European Organization for Research and Treatment of Cancer for permission to use the data from EORTC study 55971 for this research. The contents of this publication and methods used are solely the responsibility of the authors and do not necessarily represent the official views of the EORTC. The authors thank Corneel Coens for his support in providing the data and serving as liaison with the EORTC. The authors also wish to thank Mark Munsell for his statistical support and advice.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @LPrescottMD, @rcoledude
Contributors LSP: (1) Involved in conception and design of the project, analysis, and interpretation of data; (2) participated in drafting the article and revising it critically for important intellectual content; (3) approved the final manuscript. IV: (1) Involved in conception and design of the project, acquisition of data, analysis, and interpretation of data;(2) participated in drafting the article and revising it critically for important intellectual content; (3) approved the final manuscript. CCS: (1) Involved in conception and design of the project, analysis, and interpretation of data; (2) participated in drafting the article and revising it critically for important intellectual content; (3) approved the final manuscript. DCB: (1) Involved in conception and design of the project; (2) participated in drafting the article and revising it critically for important intellectual content; (3) approved the final manuscript. RLC: (1) Involved in conception and design of the project, analysis and interpretation of data; (2) participated in drafting the article and revising it critically for important intellectual content; (3) approved the final manuscript.
Funding This research was supported in part by the National Institutes of Health through MD Anderson Cancer Center’s support grant CA016672, the Ann Rife Cox Chair in Gynecology, and the Judy Reis/Al Pisani, MD Ovarian Cancer Research Fund. LSP was supported for work on this projectb y a NIH T32 grant, Training of Academic Gynecologic Oncologists, from the National Cancer Institute (5T32-CA101642).
Competing interests RLC: grants from AstraZeneca, Clovis, Genelux, Genmab, Merck, Immunogen Janssen, Roche/Genentech; consulting fees from Agenus, Alkermes, AstraZeneca, Clovis, Deciphera, Genelux, Genmab, GSK, Immunogen Janssen, OncoQuest, Onxeo, Onxerna, Regeneron, Roche/Genentech; participated in a data safety monitoring board or advisory board - VBL therapeutics. LSP: advisory board tempus, payment or honoraria for lectures from Clinical Care Options. CCS: research funding AstraZeneca; payment or honoraria from Ludemann Family Fund. IV: grants or contracts Amgen, Roche, Oncoinvent; consulting fees - Amgen (Europe) GmbH (2019), AstraZeneca (2019-2020), Clovis Oncology inc. (2019), Carrick Therapeutics (2019), Deciphera Pharmaceuticals (2020), Elevar Therapeutics (2020), F. Hoffmann-La Roche Ltd (2019-2020), Genmab (2019-2020), GSK (2019-2020), Immunogen Inc. (20192020), Mersana (2020), Millennium Pharmaceuticals (2019), MSD (2019-2020), Novocure (2020), Octimet Oncology (2019), Oncoinvent AS (2019-2020), Sotio a.s. (2019-2020), Verastem Oncology (2020), Zentalis (2020) Deciphera Pharmaceuticals (2021), Jazzpharma (2021-2022), Oncoinvent AS (2021-2022); payment or honoraria - Agenus (2021), Aksebio (2021), AstraZeneca (2021-2022), Bristol Myers Squibb (2021), Deciphera Pharmaceuticals (2021), Eisai (2021), F. Hoffmann-La Roche Ltd (2021), Genmab (2021), GSK (2021), Immunogen Inc. (2021-2022), Jazzpharma (2021-2022), Karyopharm (2021), MSD (2021-2022), Novocure (2021-2022), Novartis (2021), Oncoinvent AS (2021-2022), Seagen (2021), Sotio a.s. (2021-2022); meeting support - Amgen, MSD, Tesaro, AstraZeneca, Roche advisory board - Agenus (2021), AstraZeneca (2021-2022), Bristol Myers Squibb (2021), Deciphera Pharmaceuticals (2021), Eisai (2021), F. Hoffmann-La Roche Ltd (2021), Genmab (2021), GSK (2021), Immunogen Inc. (2021-2022), MSD (2021-2022), Novocure (2021-2022), Novartis (2021), Seagen (2021), Sotio a.s. (2021-2022)
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.