Article Text

Abstract
Objective Revised staging of patients with locally advanced cervical cancer is based on clinical examination, imaging, and potential surgical findings. A known limitation of imaging techniques is an appreciable rate of understaging. In contrast, surgical staging may provide more accurate information on lymph node involvement. The aim of this prospective study was to evaluate the impact of pre-treatment surgical staging, including removal of bulky lymph nodes, on disease-free survival in patients with locally advanced cervical cancer.
Methods Uterus-11 was a prospective international multicenter study including patients with locally advanced cervical cancer who were randomized 1:1 to surgical staging (experimental arm) or clinical staging (control arm) followed by primary platinum-based chemoradiation. Patients with histologically proven squamous cell carcinoma, adenocarcinoma, or adenosquamous cancer International Federation of Gynecology and Obstetrics (FIGO) 2009 stage IIB–IVA underwent gynecologic examination and pre-treatment imaging including abdominal computed tomography (CT) and/or abdominal magnetic resonance imaging (MRI). Patients had chest imaging (any of the following: X-ray, CT, or PET-CT). The primary endpoint was disease-free survival and the secondary endpoint was overall survival. An ad hoc analysis was performed after trial completion for cancer-specific survival. Randomization was conducted from February 2009 to August 2013.
Results A total of 255 patients (surgical arm, n=130; clinical arm, n=125) with locally advanced cervical cancer were randomized. Of these, 240 patients were eligible for analysis. The two groups were comparable with respect to patient characteristics. The surgical approach was transperitoneal laparoscopy in most patients (96.6%). Laparoscopic staging led to upstaging in 39 of 120 (33%) patients. After a median follow-up of 90 months (range 1–123) in both arms, there was no difference in disease-free survival between the groups (p=0.084). For patients with FIGO stage IIB, surgical staging is superior to clinical staging with respect to disease-free survival (HR 0.51, 95% CI 0.30 to 0.86, p=0.011). In the post-hoc analysis, surgical staging was associated with better cancer-specific survival (HR 0.61, 95% CI 0.40 to 0.93, p=0.020).
Conclusion Our study did not show a difference in disease-free survival between surgical and clinical staging in patients with locally advanced cervical cancer. There was a significant benefit in disease-free survival for patients with FIGO stage IIB and, in a post-hoc analysis, a cancer-specific survival benefit in favor of laparoscopic staging. The high risk of distant metastases in both arms emphasizes the need for further evaluation.
- cervical cancer
- radiation oncology
- surgical procedures
- operative
- laparoscopes
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, an indication of whether changes were made, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
HIGHLIGHTS
There was no difference in disease-free survival between surgical and clinical staging in patients with locally advanced cervical cancer.
The Uterus-11 trial is the only completed randomized trial comparing surgical (laparoscopic) versus clinical staging prior to primary chemoradiation.
Laparoscopic staging was safe, did not delay primary chemoradiation, and led to 33% upstaging in patients with locally advanced cervical cancer.
Introduction
Tumor stage and lymph node involvement are the most important prognostic factors for patients with locally advanced cervical cancer. In particular, the detection of para-aortic lymph node metastases is of utmost importance in order to adjust target volume definition of primary chemoradiation. Para-aortic lymph node involvement occurs in approximately 10–50% of patients with locally advanced cervical cancer.1–3 Known limitations of imaging modalities, even positron emission tomography-computed tomography (PET-CT), lead to false negative rates of 8–20%,4–6 potentially advocating surgical staging. However, this has been a controversial topic among gynecologic oncologists and radiation oncologists for decades due to contradictory results published in the literature.1 7–12 Unacceptably high treatment-related toxicity caused the premature termination of the only previously published randomized trial.13 Another planned randomized study (LiLACs) could not be finished due to lack of funding.14 Although the principle of upstaging and its impact on treatment has been confirmed, discussion continues on morbidity associated with surgical staging, particularly when using an open approach.6 Consequently, recommendations with regard to surgical staging are contradictory in national and international guidelines.15 16
The Uterus-11 randomized intergroup (German Association of Gynecologic Oncology, North-Eastern German Gynecologic Oncology Group, and German Association of Radiation Oncology) study was designed to evaluate the impact of pre-treatment surgical staging, including removal of bulky lymph nodes, on disease-free survival for patients with locally advanced cervical cancer. First analyses of this trial showed that laparoscopic surgical staging was not associated with higher rates of early toxicity during chemoradiation or a delay in treatment.17 18 Furthermore, our study showed that upstaging occurred in 33% of patients who underwent surgical staging, thus leading to treatment changes.3 The current study reports on the prospective comparison of disease-free survival between surgical and clinical staging. In addition, we present data on the secondary outcome of overall survival and on post-hoc analysis evaluating cancer-specific survival.
Methods
Patients with histologically proven squamous cell carcinoma, adenocarcinoma, or adenosquamous cell cancer International Federation of Gynecology and Obstetrics (FIGO) 2009 stage IIB–IVA underwent gynecologic examination and pre-treatment imaging including abdominal CT and/or abdominal magnetic resonance imaging (MRI) and any of the following chest imaging (X-ray, CT, or PET-CT). There was no central imaging review. Eligible patients were 1:1 randomized to either the experimental (surgical staging) arm or the control (clinical staging) arm. For patients with suspicious para-aortic lymph nodes in the clinical staging arm, a CT-guided lymph node biopsy was performed prior to primary chemoradiation, and in patients with metastatic disease in those lymph nodes, the radiation field was extended (Figure 1). The study was approved by the institutional review boards of the participating institutions. An independent data safety board evaluated the safety and recruitment of the trial annually.
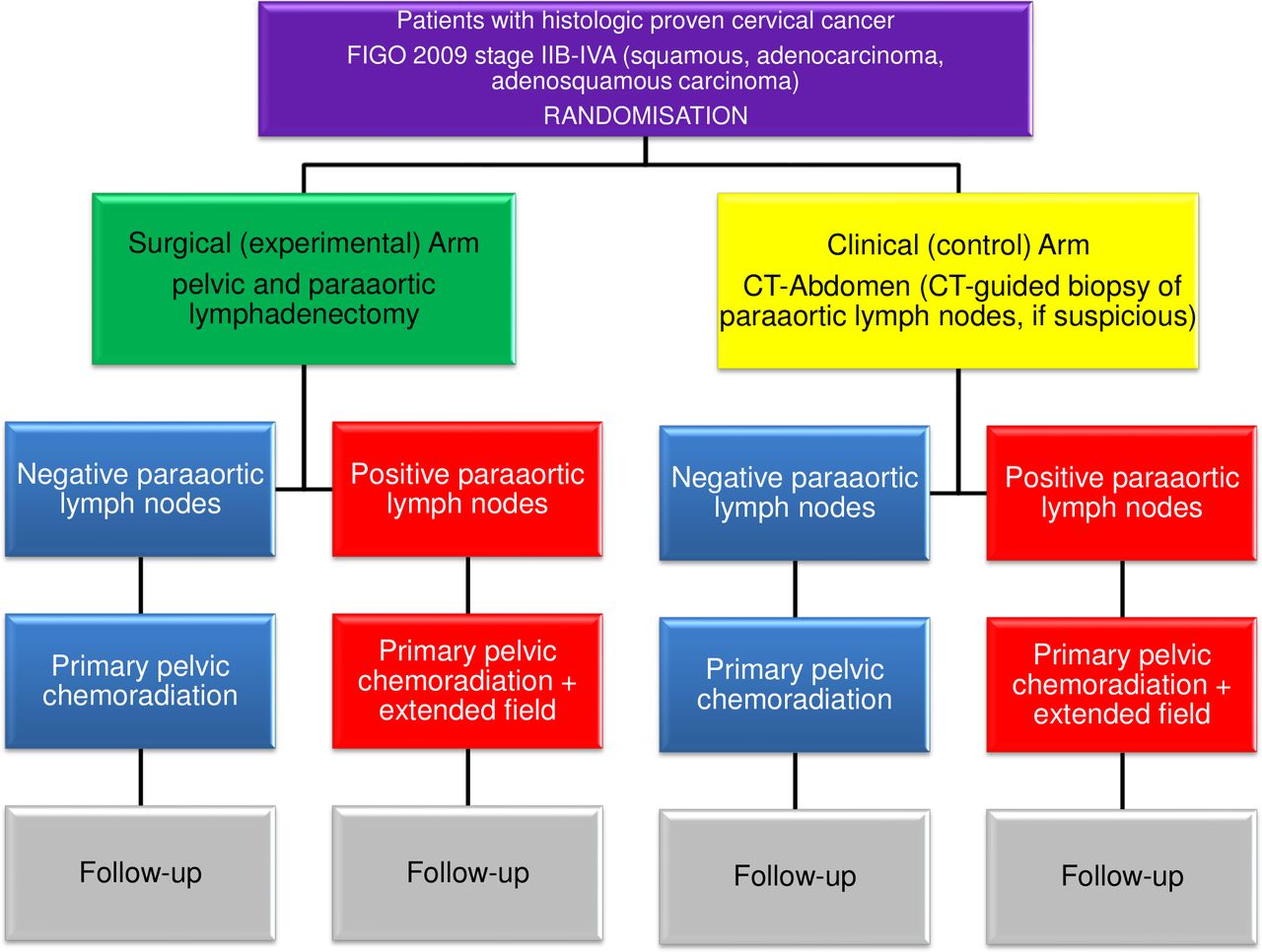
Flowchart of the Uterus-11 study design.
Surgical Staging
Details of surgical staging have been reported elsewhere17 (see online supplement). Surgical staging prior to primary chemoradiation was performed via a transperitoneal laparoscopic, extraperitoneal laparoscopic, or open transperitoneal approach. After careful inspection of the abdominal cavity, biopsies were taken from any suspicious area and sent to frozen section. If peritoneal spread and/or tumor in the supraclavicular lymph node were confirmed, no retroperitoneal lymph node dissection was carried out and the operation was abandoned. In all other patients, para-aortic and bilateral pelvic lymphadenectomy was performed. The upper limit of para-aortic lymphadenectomy was the renal vessels; pelvic lymphadenectomy comprised external iliac and obturator lymph nodes. If enlarged/bulky para-aortic and/or pelvic lymph nodes were identified, removal of these was mandatory in order to reduce the burden for subsequent chemoradiation.
Supplemental material
Chemoradiation
Details of primary chemoradiation have been reported elsewhere.18 Primary chemoradiation in both arms comprised external beam radiation, brachytherapy, and concurrent chemotherapy according to national and international guidelines. Patients underwent radiation-planning CT using immobilization devices with a full bladder and empty rectum, with 2 mm slices from the 12th thoracic vertebra in cases of para-aortic lymph node metastases for extended fields or from the third lumbar vertebra in cases of only pelvic radiation to trochanter minor. Commercial treatment planning systems were used for contouring and planning. Radiation treatment was performed using intensity modulated radiotherapy (IMRT) techniques (volumetric arc, conventional IMRT, or tomotherapy) in 65% and three-dimensional planned conventional techniques in 35% of patients using 6 or 10 MV-X photons. Five weekly single doses of 1.8 Gy to a total dose of 50.4 Gy with or without a simultaneous or sequential parametric boost to a total dose of 60 Gy to the parametria were applied. Brachytherapy was performed according to the policy of the center. MRI-based after-loading was recommended according to the GEC-ESTRO recommendations. The tumor region (high-risk area of residual tumor) had to be covered by at least 80 Gy (EQD2,α/β = 10) taking brachytherapy and external beam radiation together. Cisplatin 40 mg/m2 body surface area was given in five weekly applications to a total dose of 200 mg/m2 during external beam radiation. In case of contraindication to cisplatin, carboplatin (area under curve 2-weekly) was applied.
Statistical Analysis
Survival endpoints were defined as the time from randomization to relapse or death from any cause. The primary endpoint was disease-free survival and the secondary endpoint was overall survival, measured as the time from randomization to death from any cause. As a post-hoc analysis, we also evaluated cancer-specific survival. Death without prior relapse was considered an event in the definition of disease-free survival. The sample size calculation assumed a disease-free survival of 54% after 5 years in the experimental arm (surgical staging) and 36.5% in the control arm (clinical staging) based on a Gynecologic Oncology Group (GOG) analysis by Gold et al.7 In total, a sample size of 250 patients including 20% drop-outs, leading to 200 evaluable patients and a number of events amounting to 129, was needed to achieve a power of 80%. A recruitment period of 4 years and a minimum follow-up of 4 years was planned. The actual recruitment period was 4 years and 6 months (February 2009 to August 2013) and the planned follow-up ended in August 2017. Follow-up was prolonged until August 2019 because fewer events were observed than the planned number to August 2017. However, even after the prolonged period, there were only 102 events in 240 evaluable patients (compared with 129 events planned). At this point it was decided to close the databank and perform primary statistical analysis. Randomization was 1:1 stratified for FIGO 2009 stage (IIB vs III/IV) and study center.
Survival rates for the primary and secondary endpoints and related survival curves were estimated using the Kaplan–Meier method. Hazard ratios (HR) including two-sided 95% limits of confidence were estimated using the Cox proportional hazard model including the study arm only. In three sensitivity analyses this model was adjusted, stratified, and calculated separately for FIGO stage. Additionally, interaction terms between the study arm and FIGO stage were tested for each outcome. Note, however, that the study was not powered for sub-group analyses. Cancer-specific survival was affected by a competing risk (death from other causes) and the Fine–Gray method19 was applied to estimate sub-distribution hazard ratios for cumulative incidences and their respective confidence limits and p values. Sensitivity analyses included adjustment for histology (squamous cell carcinoma vs adenocarcinoma/adenosquamous cell carcinoma) and tumor size (≤4 cm vs >4 cm).
The primary analysis population was the intent-to-treat population. Comparisons of baseline characteristics between study arms were conducted using the χ2 test (categorical variables), the Mann–Whitney test (ordered or non-normally distributed variables), and the t-test for independent samples (normally distributed variables). The level of significance was 0.05 (two-sided) in all analyses. However, only the primary analysis for disease-free survival was confirmatory; p values given for the secondary analysis should be interpreted as additional descriptive parameters. The analysis was performed using SPSS (IBM, Armonk, New York, USA) for Windows, release 25, and R (R Foundation for Statistical Computing, Vienna, Austria) release 3.01.
Results
A total of 255 patients with cervical cancer FIGO 2009 stage IIB–IVA were randomized, with a subsequent total of 240 evaluable patients, 121 in the surgical arm and 119 in the clinical arm. There were no significant differences between the two arms with respect to clinical parameters, except for a higher number of grade 3 tumors in the control arm (Table 1).
Demographic and clinical data
Surgical Staging
Surgical staging was performed via the laparoscopic approach in 96.6% of patients. Intra-operative and post-operative complication rates were 1.6% and 7.3%, respectively. The median number of harvested pelvic and para-aortic lymph nodes was 19 (range 1–70) and 17 (range 3–74), respectively. In the surgical arm, positive pelvic lymph nodes were confirmed in 51% of patients and positive para-aortic lymph nodes in 24% of patients.3 The median time between surgical staging and the start of chemoradiation was 13 days (range 7–21),17 and the median time interval between randomization and the start of chemoradiation in the clinical arm was 13.5 days (range 3–30). Histology results led to upstaging in 33% of patients in the surgical arm compared with 8% in the clinical arm (CT-guided lymph node biopsy) (p<0.001).3 Of note, a total of 47 patients underwent PET/CT scans; however, the number of patients was considered too small to derive definitive conclusions on analysis of comparison.
Chemoradiation
A total of 236 of the 240 patients (98.3%) underwent external beam radiation therapy with a median total dose of 50.4 Gy (117 patients in the surgical arm and 119 patients in the clinical arm, Figure 2). The radiation technique used was IMRT in 65% of patients and three-dimensional radiation therapy in 35% of patients. The mean total treatment time was 53.7±8.9 days in the experimental arm and 53.0±9.8 days in the clinical arm. Patients in the surgical arm received extended field radiation more frequently than those in the clinical arm (23% vs 12%, p=0.02). In 234 patients (97.5%) platinum-based chemotherapy was administered. High dose rate (HDR)-192Ir brachytherapy was performed in 227 of the 240 patients (94.5%), with a median single dose of 6 Gy to a median nominal total dose of 28 Gy. Chemotherapy and radiation were well tolerated in both arms without early genitourinary and gastrointestinal toxicity grade >3. No chemoradiation-related death occurred in either arm.18

CONSORT diagram. EBRT, external beam radiation therapy; FIGO, International Federation of Gynecology and Obstetrics; RCT, chemoradiation.
Oncologic Results
Overall, 102 patients relapsed or died. In 90 patients death was cancer-related (Table 2). There was no difference in disease-free survival between the surgical staging and clinical staging arms (95% CI 0.48 to 1.05, p=0.084). Analyses adjusted (HR 0.73, 95% CI 0.49 to 1.08, p=0.12) or stratified (HR 0.74, 95% CI 0.50 to 1.10, p=0.13) for FIGO stage showed similar results. Moreover, surgical staging was associated with significantly improved disease-free survival compared with clinical staging in patients with FIGO stage IIB (HR 0.51, 95% CI 0.30 to 0.86, p=0.011), but not in patients with FIGO stage III (HR 1.24, 95% CI 0.67 to 2.28, p=0.50). The difference between the HRs (0.51 vs 1.24) was significant (statistical interaction between study arm and FIGO stage p=0.031). In 41 (34%) of 121 patients in the surgical staging arm and 54 (45%) of 119 patients in the clinical staging arm there was recurrence of disease at study completion. In the post-hoc analysis evaluating cancer-specific survival, patients in the surgical staging arm had improved outcomes (HR 0.61, 95% CI 0.40 to 0.93, p=0.020; FIGO IIB: HR 0.35, 95% CI 0.19 to 0.64, p<0.001; FIGO III: HR 1.27, 95% CI 0.69 to 2.33, p<0.44; Figure 3). A sub-analysis of patients who underwent extended field radiation (6%) in either group was not possible due to the small number of patients.
Reasons for non-cervical cancer-related death

{kind=link}
{kind=link}
{kind=link}
(A) Disease-free survival, (B) overall survival, (C) disease-free survival FIGO stage IIB, and (D) cancer-specific death rate (mortality).
The most important risk factor was the FIGO stage for each of the outcomes. For FIGO stage III/IV, HR was 1.89 (95% CI 1.27 to 2.83, p=0.002) for overall survival, 1.81 (95% CI 1.22 to 2.69, p=0.003) for disease-free survival, and 2.21 (95% CI 1.45 to 3.35, p=0.0002) for cancer-specific survival. In contrast, patients with adenocarcinoma or adenosquamous carcinoma had no increased risk for progression compared with patients with squamous cell carcinoma, with HR 1.28 (95% CI 0.73 to 2.26, p=0.39) for overall survival, 1.23 (95% CI 0.70 to 2.15, p=0.48) for disease-free survival, and 1.16 (95% CI 0.63 to 2.13, p=0.63) for cancer-specific survival. Patients with bulky tumors (>4 cm) had no significant difference in overall survival (HR 1.67, 95% CI 0.98 to 2.86, p=0.06) and disease-free survival (HR 1.52, 95% CI 0.91 to 2.52, p=0.096) compared with patients with tumors ≤4 cm. However, there was a difference in cancer-specific survival (HR 1.92, 95% CI 1.07 to 3.45, p=0.028). Lymph node status could only be evaluated in patients with surgical staging. The presence of para-aortic lymph metastases (overall survival: HR 3.14, 95% CI 1.67 to 5.90; disease-free survival: HR 3.03, 95% CI 1.63 to 5.62; cancer-specific survival: HR 3.53, 95% CI 1.84 to 6.79; p<0.001 for each outcome) and pelvic±para-aortic lymph nodes (overall survival: HR 3.30, 95% CI 1.61 to 6.76; disease-free survival: HR 2.79, 95% CI 1.43 to 5.46; cancer-specific survival: HR 3.79, 95% CI 1.72 to 8.33; p<0.001 for each outcome) were negative prognostic factors. When recurrence was detected, it was distant or distant in combination with local in 87% in the surgical arm and 91% in the clinical arm.
Discussion
Our study showed that there was no difference in disease-free survival between surgical staging and clinical staging in patients with locally advanced cervical cancer. In patients with locally advanced cervical cancer and any pelvic±para-aortic, any para-aortic, or any histologically confirmed lymph node metastases, false negative imaging occurs in 30–50%, 10–37%, and 8–25% of cases, respectively.6 20–23 In their meta-analysis, Choi et al derived pooled sensitivities and specificities for detecting lymph node metastases for CT (50% and 92%), MRI (56% and 91%), and PET-CT (82% and 95%).24 Detection of lymph node metastases is of utmost importance for defining the personalized treatment volume and achieving subsequent improved outcomes after chemoradiation. Although patients in the Uterus-11 trial did not routinely undergo pre-operative PET-CT, study results need to be compared with PET-CT, which is considered the standard-of-care for pre-operative work-up today in many centers, rather than surgical staging.8 The main arguments for PET-CT are avoiding potential surgical morbidity, delay in starting chemoradiation, and the lack of evidence for improved survival following performance of surgical staging.8 23 However, as demonstrated in several retrospective and prospective studies, in patients with negative PET-CT who underwent minimally invasive para-aortic lymph node staging, the false negative rate for para-aortic lymph node involvement is between 8% and 22%, especially in those patients with PET-CT positive pelvic nodes20 or small tumor volume in para-aortic lymph nodes.5
Surgical staging should not be performed via laparotomy in order to avoid the subsequent severe morbidity or mortality during radiation that occurs in up to 34% of patients.23 Using a laparoscopic approach, the complication rate is between 1.6% and 7% without delay of primary chemoradiation.2 4 5 9 17 20 22 23 25 26 It is not finally decided whether a transperitoneal or retroperitoneal approach, a conventional or robotic laparoscopy, and the infra-renal or infra-mesenteric extent of para-aortic lymphadenectomy should be preferred.2 4 9 12 25 The surgical approach used in the Uterus-11 trial was conventional laparoscopy extending to the renal vessels in 96.6% of patients. Furthermore, Lee et al showed that nodal staging surgery before definitive chemoradiation may be cost effective, especially in patients with negative PET-CT.27 Well-designed randomized trials comparing PET-CT with surgical staging (PALDISC trial) are ongoing.28 Minimally invasive surgical staging in patients with locally advanced cervical cancer has demonstrated upstaging rates between 22% and 43% compared with clinical staging.1 7 At 33%, the rate of upstaging in Uterus-11 is exactly within this range.3
Another important aspect of surgical staging is the potential oncologic benefit of removing bulky pelvic and para-aortic lymph node metastases prior to primary chemoradiation. Thus, from a radiobiological point of view, one should consider removal of larger lymph nodes in order to provide higher locoregional control. Wakatsuki et al have described a 97% control rate with 50 Gy radiotherapy for lymph nodes <10 mm in patients with cervical cancer in contrast to 76% for nodes >10 mm.29 Similar results were found by Oh et al in 310 patients with locally advanced cervical cancer with a follow-up of 83 months. In-field failure rates for pelvic as well as para-aortic lymph nodes >10 mm were significantly higher than for smaller lymph nodes.30 This has been confirmed by retrospective clinical data.1 7
Primary chemoradiation in both arms of the Uterus-11 trial fulfilled high-quality treatment standards with respect to radiation treatment duration, use of brachytherapy, application of concomitant chemotherapy, and use of modern techniques for external beam radiation therapy and brachytherapy. Consequently, over 92% of the patients in the Uterus-11 study received a biologically sufficient tumor dose (external beam radiation therapy + brachytherapy), which is much better than general chemoradiation practice.31 Moreover, early chemoradiation-related toxicity in Uterus-11 was moderate with 0% grade >3 genitourinary and gastrointestinal toxicity, 6% grade 3 nausea, 3% grade 3 vomiting, and <2% grade 3 diarrhea. In contrast, within the small prematurely closed randomized study by Lai et al using outdated radiation techniques, toxicity grade ≥3 occurred in 45% of patients in the clinical arm and 38% in the surgical arm, which demonstrated that radiation technique, not surgery, contributed to the unfavorable results.13
Para-aortic lymph node metastases significantly impair survival of patients with locally advanced cervical cancer, as demonstrated in several retrospective publications.1 7 Benito et al reported a mean survival time in 139 patients of 77 months and 21 months, respectively, for patients without (N0) and with (N1) proven para-aortic lymph node metastasis. Mezquita et al found a 5-year overall survival rate in 67 patients of 71% (N0) and 21% (N1).22 26 Similar results were described by Gouy et al with 3-year event-free survival of 74%, 69%, and 17% for para-aortic N0, N1 <5 mm, and N1 >5 mm, respectively.12 However, further oncologic results of studies comparing clinical staging versus surgical staging in patients with locally advanced cervical cancer differ considerably. Analyzing the data of GOG 85, GOG 120, and GOG 165 trials, Gold et al showed a benefit in progression-free survival (50% vs 36%) and overall survival (54% vs 40%) in favor of surgical staging, which was more beneficial for stage III/IV than for stage II.7 Dabi et al10 compared 377 patients who underwent surgical staging with 270 patients who had clinical staging. After a mean follow-up of 38 months, patients in the surgical group had a better prognosis with respect to disease-free survival (OR 0.64) and overall survival (OR 0.43). However, a study by Yang et al in 148 patients with locally advanced cervical cancer showed no significant survival differences between the surgical and imaging group after a mean follow-up of 41 months.32
The only prospective randomized trial so far has to be interpreted with caution due to the small number of patients (n=29 clinical arm, n=32 surgical arm) and also because it was prematurely stopped due to significantly worse disease-free survival in the surgical arm with an HR of 3.13 for recurrence and HR 1.76 for death. However, all eight patients with histologically confirmed para-aortic lymph node metastasis died due to treatment failure or complications. Given the low number of events, this probably influenced survival curves.13
The rates of 5-year disease-free survival, 5-year overall survival, and 5-year cancer-specific survival in the Uterus-11 trial were 67%, 68%, and 73% for surgical staging and 57%, 58%, and 58% for clinical staging. For FIGO stage II, the 5-year disease-free survival, 5-year overall survival, and 5-year cancer-specific survival in the Uterus-11 trial were 77%, 80%, and 86% for surgical staging and 59%, 60%, and 61% for clinical staging, which is in the upper range of previously reported oncologic results.7 26 32
Although negative for the primary endpoint, our study results suggest that surgical staging prior to primary chemoradiation might be beneficial for patients with FIGO stage IIB tumors (HR 0.51). Thus, further studies in patients with FIGO stage IIB tumors should be considered. The fact that in cases of recurrence there were >85% distant metastases underlines the need for more effective systemic (maintenance) treatments such as sequential chemotherapy following primary chemoradiation, immunotherapy, or a combination of both.32
Among the strengths of our study is the fact that it is the largest investigator-initiated randomized trial comparing surgical staging with clinical staging in patients with locally advanced cervical cancer. Nearly all patients underwent surgical staging by a minimally invasive approach and modern radiation techniques. Long-term follow-up and a high level of data completeness was achieved. However, PET-CT could not be routinely implemented in pre-operative work-up due to lack of reimbursement. Patients with stage IB2 (FIGO 2009) could not be included in the protocol. Finally, with only 102 instead of 129 observed events, the power of our study was 70% instead of 80% as initially planned.
Conclusion
The Uterus-11 trial showed that laparoscopic staging prior to primary chemoradiation in patients with locally advanced cervical cancer was not associated with improved disease-free survival or overall survival. Patients with FIGO stage IIB benefit from surgical staging prior to primary chemoradiation. We showed that surgical staging is safe and leads to an upstaging in more than 30% of patients. Primary chemoradiation was not delayed nor associated with higher rates of early complications following surgical staging.
Supplemental material
Supplemental material
Acknowledgments
We thank Talita Garcia do Nascimento and Sylvia Blass for excellent technical support.
References
Footnotes
Contributors All authors contributed substantially to this manuscript.
Funding This study was funded by Deutsche Krebshilfe.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.