Article Text

Abstract
Objective Previous studies have investigated the impact of preoperative hysteroscopy on the staging and survival of predominantly grade 1 endometrial cancers. We sought to evaluate the effect of hysteroscopy on the peritoneal spread of tumor cells and disease course in a large series of patients with high-risk endometrial cancer.
Methods Patients who underwent hysterectomy for grade 3 endometrial carcinoma on final surgical pathology at the Mayo Clinic in Rochester, MN between January 2009 to June 2016 were included, noting hysteroscopy within 6 months from surgery. Intra-peritoneal disease was defined as any positive cytology OR adnexal invasion OR stage IV. The presence of intra-peritoneal disease OR peritoneal recurrence within 2 years from surgery was defined as peritoneal dissemination. Cox proportional hazards models were fit to evaluate associations between hysteroscopy exposure and progression within 5 years following surgery.
Results Among 831 patients, 133 underwent hysteroscopy. There was no difference in age, body mass index, ASA ≥3, or serous histology between patients who did or did not undergo hysteroscopy. Advanced stage disease (III/IV) was less common among patients who underwent hysteroscopy (30.1% vs 43.8%, P=0.003). No difference was observed between those with vs without hysteroscopy in the rate of positive cytology (22.0% vs 29.7%, P=0.09), stage IV (16.5% vs 21.9%, P=0.16), intra-peritoneal disease (28.6% vs 36.1%, P=0.09), or peritoneal dissemination (30.8% vs 39.3%, P=0.06). On stratifying by stage, hysteroscopy did not increase the risk of progression (HR 1.06, 95% CI 0.59 to 1.92 for stage I/II; HR 0.96, 95% CI 0.62 to 1.48 for stage III/IV).
Conclusion In this retrospective study of grade 3 endometrial cancer, we did not observe any significant association between pre-operative hysteroscopy and the incidence of positive cytology, peritoneal disease, peritoneal dissemination, or cancer progression.
- endometrial neoplasms
- hysteroscopes
- surgical procedures
- operative
- neoplasm recurrence
- local
Statistics from Altmetric.com
HIGHLIGHTS
The use of hysteroscopy has previously been studied in predominantly low-grade endometrial cancer
Our study reviewed the use of hysteroscopy and its effect on peritoneal disease in the workup of grade 3 endometrial cancer
Hysteroscopy was not associated with an increased risk of positive cytology, peritoneal disease, peritoneal dissemination, or cancer progression
Introduction
Endometrial cancer is the most common gynecologic cancer in developed countries, and its incidence is currently increasing.1 Abnormal uterine bleeding is the presenting symptom in up to 90% of patients.2 The diagnosis of endometrial cancer is typically made via endometrial sampling by office endometrial biopsy, uterine curettage, or hysteroscopy with directed endometrial biopsy.3 The advantages of hysteroscopy include direct visualization of the endometrial cavity, with hysteroscopy-guided biopsy serving as the gold standard for full evaluation of abnormal uterine bleeding.4 Within the oncology community, concerns have surfaced regarding the possible intraperitoneal spread of cancer cells via pressurized spill through the fallopian tubes during the procedure. This has been hypothesized to have a deleterious effect on staging and prognosis.
The literature to date has reported a higher frequency of positive peritoneal cytology in women undergoing hysterectomy following diagnostic hysteroscopy, but the long-term significance of this is unclear.3 5–9 Other surgical practices that have been called into question for endometrial cancer patients include the use of uterine manipulators, which have not yet been found to increase the risk of disease progression.10–12 Existing research has evaluated the use of hysteroscopy on patients with predominantly early-stage or low-grade endometrioid tumors, and has found no increased risk of gross peritoneal disease, or disease recurrence in these cases.8 13–18
Studies on the safety of hysteroscopy in patients with predominantly lower-risk histologies cannot be extrapolated to infer safety for high-risk histologies. No studies to date have investigated the effect of hysteroscopy on a large number of high-risk histology endometrial cancer patients. Given this, we sought to investigate the effect of preoperative hysteroscopy on the final pathologic stage at the time of surgery, peritoneal dissemination, recurrence, and survival of patients with all stages of grade 3 endometrial cancer. We hypothesize that patients undergoing hysteroscopy prior to the diagnosis of grade 3 endometrial malignancies may be at increased risk of peritoneal tumor seeding, resulting in increased omental involvement, adnexal disease, positive cytology, and peritoneal dissemination.
Methods
This study was approved by the Mayo Clinic institutional review board. Patients who underwent primary hysterectomy for grade 3 endometrial cancer at the Mayo Clinic in Rochester, MN between January 2009 and June 2016 were included for review. All patients were confirmed to have active research authorization. None received neoadjuvant chemotherapy or had synchronous tumors. Within this group, those who had undergone hysteroscopy were identified, and its timing relative to surgery noted. Hysteroscopy was performed either in the office, or in the operating room under general anesthesia, using normal saline as the distending media. The timing of hysteroscopy was grouped as same day of surgery, 1–7 days, 8–30 days, or 31–180 days prior to surgery.
Surgery included, at a minimum, hysterectomy (robotic, laparoscopic, or abdominal), bilateral salpingo-oophorectomy, and in the majority of patients, cytology and pelvic or peri-aortic lymph node assessment. Peritoneal cytology was performed at the Mayo Clinic as part of the staging procedure. Additional procedures were performed as indicated for serous histology (omental biopsy), generalized tumor debulking, and other procedures including bowel resection for advanced stage disease. Patients were staged according to the International Federation of Gynecology and Obstetrics (FIGO) 2009 staging guidelines, with final stage, histologic type, and grade confirmed by gynecologic pathologists. All stages of patients with high grade (grade 3) and non-endometrioid histology were included. Patients were recommended adjuvant treatment in accordance with National Comprehensive Care Network (NCCN) guidelines.19
The outcomes of interest included positive cytology, stage IV disease, a composite of (cytology or stage IV disease or adnexal disease), which was called “intra-peritoneal disease”, and a composite of cytology or stage IV disease or adnexal disease or peritoneal recurrence within 2 years, which was called “peritoneal dissemination”. In addition, progression following the date of surgery were evaluated.
Hysteroscopy exposure was defined as a hysteroscopy within the 180 days prior to hysterectomy. Comparisons of baseline characteristics and binary outcomes between those with and without hysteroscopy exposure were evaluated using the two-sample t-test for continuous variables and the chi-square test for categorical variables. The association of hysteroscopy exposure with progression and death, respectively, was evaluated separately by stage (I/II and III/IV). Given that the cohort spans from 1999 to 2016, follow-up was restricted to the first 5 years after surgery. Progression-free survival estimated using the Kaplan–Meier method. Cox proportional hazards models were fit to evaluate the association of hysteroscopy exposure with progression and death, respectively. Associations were summarized using the HR and corresponding 95% CIs. All calculated P-values were two-sided and P-values less than 0.05 were considered statistically significant. We also performed a sensitivity analysis in which we excluded patients with previous tubal ligation since we hypothesized that tubal ligation may prevent the intraperitoneal spillage of cells and confound our results.
Results
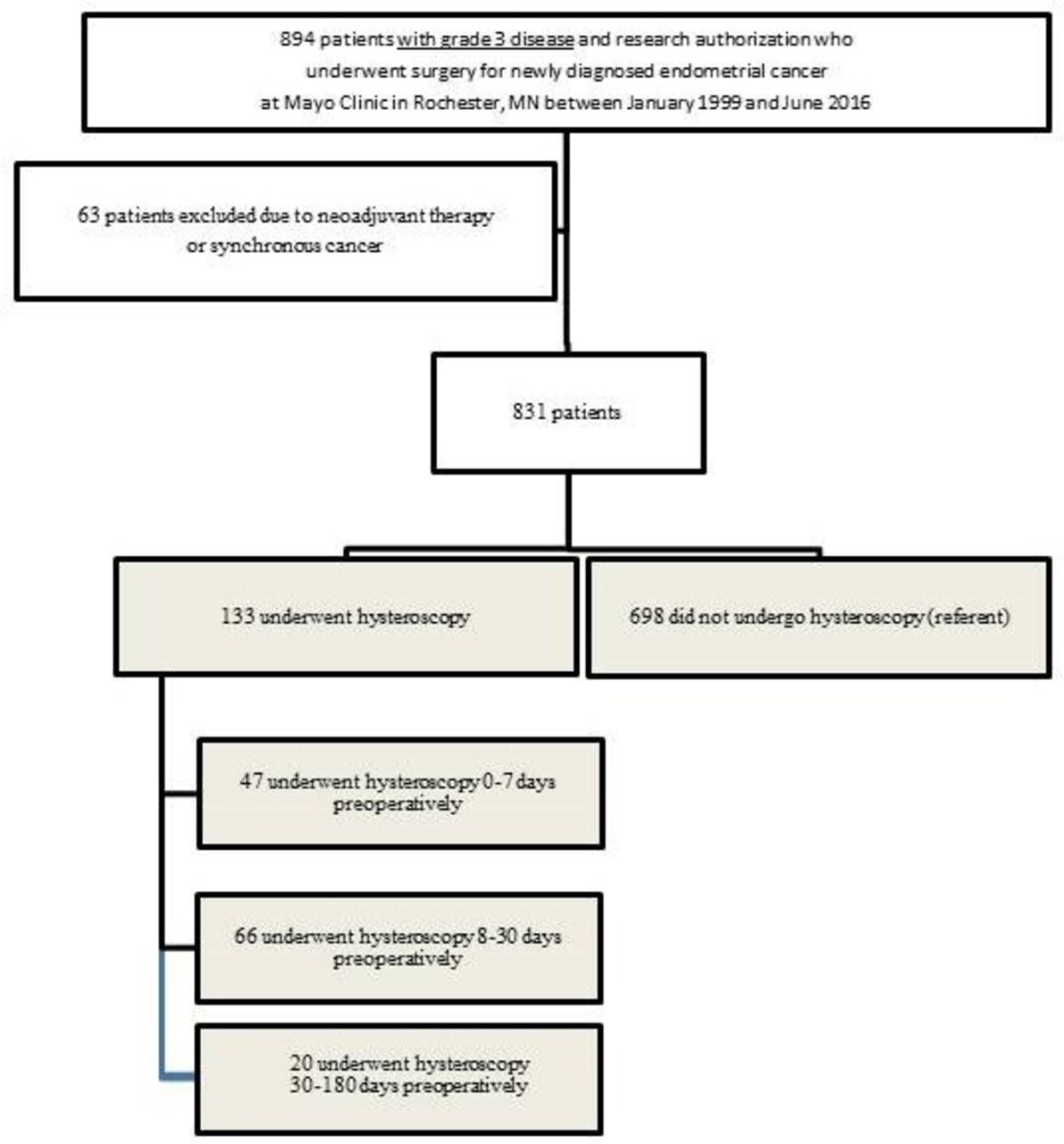
A total of 831 patients met the inclusion criteria (Figure 1). Among these 831 patients, 133 patients underwent hysteroscopy: 26 on the same day as their hysterectomy, 21 with 1–7 days, 66 within 8 to 30 days, and 20 within 31 to 180 days. Median time from hysteroscopy to surgery was 13 days (IQR, 3–22 days). Patients with vs without hysteroscopy did not significantly differ in terms of mean age (67.7 vs 67.8 years), mean body mass index (BMI) (31.6 vs 31.3 kg/m2), American Society of Anesthesiologists score ≥3 (35.3% vs 38.1%), or serous histology (47.4% [63/133] vs 48.7% [340/698]). Peritoneal cytology sampling was performed at the time of hysterectomy in similar proportions of both groups (88.7% [118/133] vs 92.1% [643/698]). The rates of adjuvant chemotherapy and radiotherapy did not differ between groups. These patient characteristics are summarized in Table 1.

Study population selection.
Baseline patient characteristics
Advanced stage disease (III/IV) was less common among those with a hysteroscopy (30.1% vs 43.8%, P=0.003). When comparing those with vs without prior hysteroscopy, we did not observe a significant difference in the rate of positive cytology, among those with cytology sampling (22.0% vs 29.7%, P=0.09). We also did not observe a significant difference in the rate of stage IV disease (16.5% vs 21.9%, P=0.16), intra-peritoneal disease (28.6% vs 36.1%, P=0.09), or peritoneal dissemination (30.8% vs 39.3%, P=0.06). In fact, the afore-mentioned outcomes rates were each non-significantly lower in those with a prior hysteroscopy. These findings remained unchanged in a sensitivity analysis excluding 21 hysteroscopy patients with a prior tubal ligation (data not shown). We did not observe a dose-response relationship for the timing of hysteroscopy with any of these outcomes (Table 2).
Peritoneal disease outcomes relative to timing of hysteroscopy
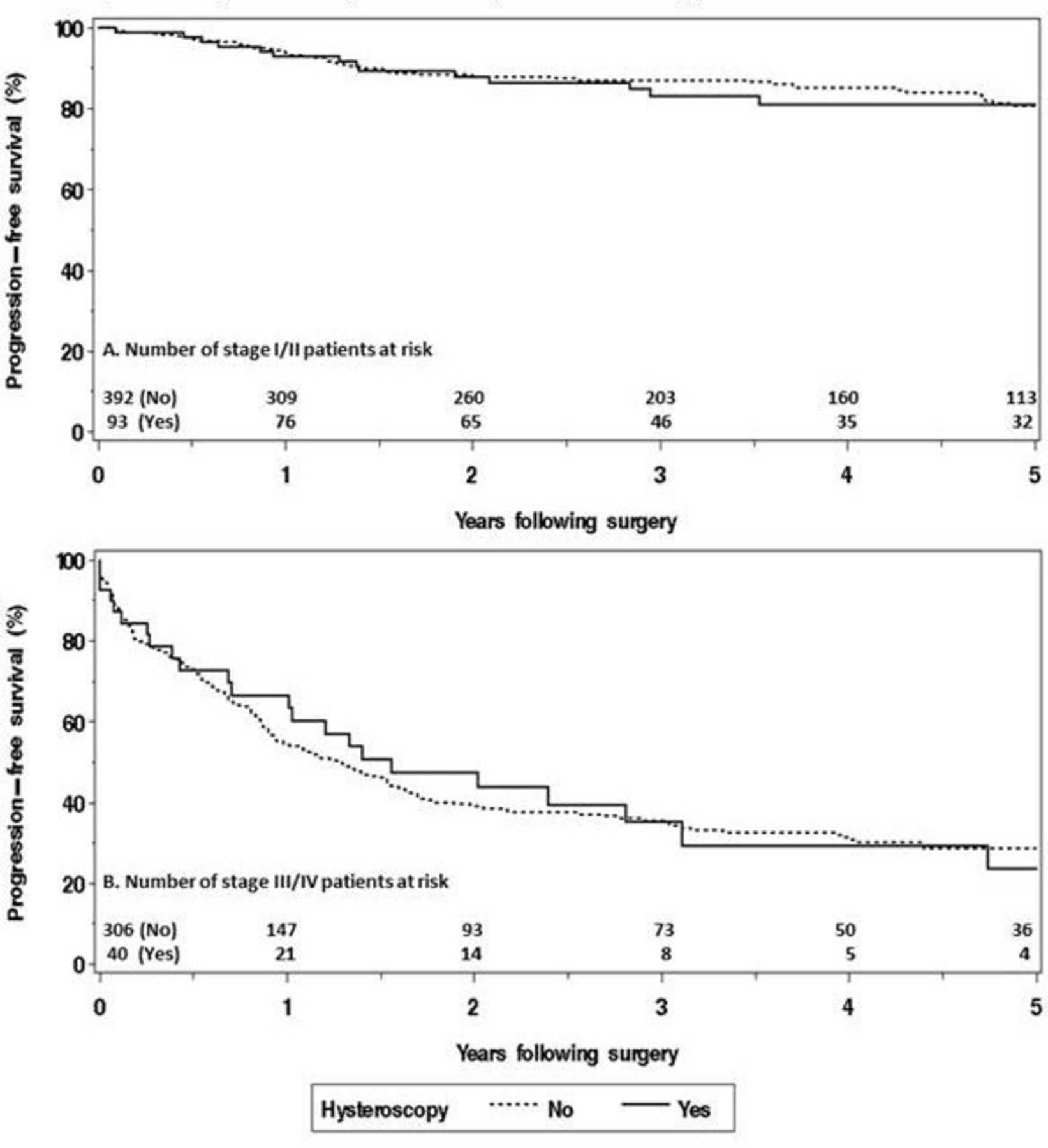
Among the 831 patients, there were 266 documented deaths within the first 5 years: the median duration of follow-up for those alive at last follow-up was 3.7 years (IQR, 2.0–6.1 years). Figure 2 depicts progression-free survival (any location) according to prior hysteroscopy, stratified by stage.
{kind=link}
{kind=link}
Progression-free survival (any location) according to prior hysteroscopy within 6 months prior to hysterectomy, stratified by International Federation of Gynecology and Obstetrics (FIGO) 2009 stage.
Patients with a prior hysteroscopy were not found to be at an increased risk of progression among those with stage I/II disease (HR 1.06, 95% CI 0.59 to 1.92 for stage I/II) or stage III/IV disease (HR 0.96, 95% CI 0.62 to 1.48 for stage III/IV). Although we saw a trend toward increased risk of vaginal progression among those with a prior hysteroscopy, the results were not statistically significant (HR 2.04, 95% CI 0.51 to 8.18, P=0.31 for stage I/II; HR 1.98, 95% 0.66–5.93, P=0.22 for stage III/IV). Small sample size prohibited analysis of the timing of hysteroscopy and vaginal progression, after stratifying by stage. Additional results for overall survival and non-vaginal progression are presented in Table 3. The findings for all of these outcomes were unchanged after excluding 21 hysteroscopy patients with a prior tubal ligation (data not shown).
Association between prior hysteroscopy and death or progression, stratified by stage
Discussion
In this retrospective study of grade 3 endometrial cancer patients, we assessed the association between preoperative hysteroscopy and the incidence of positive cytology, peritoneal disease, peritoneal dissemination, or cancer progression. We did not observe any significant associations between the practice of hysteroscopy and these important outcomes. Hysteroscopy remains the gold standard for the workup of abnormal uterine bleeding, with particular clinical utility in patients with focal lesions and/or recurrent postmenopausal bleeding.4 20 Hysteroscopy has been reported to have a sensitivity, specificity, positive predictive value, and negative predictive value of 94.2%, 88.8%, 96.3%, and 83.1%, respectively, in a series of 1500 women after comparing both operative assessment and final pathology reports.21 Office hysteroscopy has been useful in the preoperative setting to inform the risk of malignancy,4 and predict cervical spread of endometrial adenocarcinoma.22
The procedural risks of hysteroscopy are relatively minimal, and include bleeding, cervical trauma, and fluid overload via intraperitoneal absorption of distending media.23 Due to the known transmission of distending media fluid through the fallopian tubes, hypothetical concerns arise when this fluid dislodges and transports cancer cells into the peritoneal cavity. It is also unknown if the hysteroscopic media itself has any effect on cancer cell growth. Although histology may not always predict underlying genetic mutations, traditionally low-grade endometrial cancers may harbor genetic alterations which lead to less aggressive behavior (POLE (DNA polymerase epsilon), PTEN (phosphatase and TENsin)), while high-grade endometrial cancer often exhibits more aggressive alterations and may behave differently.24 25 Mutations common in these particularly aggressive cancers include p53, PI3K, KRAS, ERBB2, and MYC pathways.26 In the case of serous cancers, this is thought to predispose them to peritoneal spread and poor prognosis.27
Previous studies have noted an increased incidence of positive cytology in patients with a recent hysteroscopy, an effect which has been shown in small studies to be impacted by the timing of hysteroscopy relative to surgery28–30 in predominantly early-stage patients. This has led to speculation that this difference may be due to the timing of hysteroscopy relative to hysterectomy, with tumor cell dissemination occurring over time.15 While cytology was removed from FIGO staging criteria in 2009, the organization continued to endorse routine collection for research purposes and to inform prognosis.31 Indeed, the negative prognostic value of positive cytology has been noted in a large retrospective cohort analysis of databases such as the National Cancer Database (NCDB) and Surveillance Epidemiology and End Results (SEER) databases.31 32 The prognostic effect of positive cytology is not limited to early-stage disease, and when combined with uterine risk factors, has the utility to guide treatment.33 34 To this effect, we recommend considering cytology for research and when clinically useful to guide decisions on adjuvant treatment in clinically challenging cases, such as in earlystage disease with uterine risk factors.
To compare our findings to those of previous studies, we were able to stratify by both timing of hysteroscopy and disease stage. Our median time from hysteroscopy to surgery was 13 days (IQR, 3–22 days) in comparison with a mean of 24.4 days (12–32 days) noted in other studies.13 16 35–38 Interestingly, we did not note a relationship with the timing of hysteroscopy and positive cytology, overall or when stratified by stage. In a meta-analysis of 2944 women with all grades of endometrial cancer, Chang et al noted the rate of positive peritoneal cytology to be significantly higher in the hysteroscopy group, but a subgroup analysis of patients with early stage (I–II) disease revealed no difference between the two groups.14 In our study, fewer patients with advanced-stage disease underwent hysteroscopy prior to surgery, which does limit generalization of these results. While a type II error cannot be excluded, our study did note a non-significant trend toward increased positive cytology, increased peritoneal disease, or dissemination in patients without preoperative hysteroscopy, making a type II error less likely.
Our secondary outcome was a composite outcome of evidence of peritoneal disease spread at the time of surgery (positive cytology, stage IV disease, or adnexal involvement), or early peritoneal recurrence. Fortunately, we did not find any effect of hysteroscopy on these, nor on disease progression or overall survival. This finding is in accordance with previous authors’ survival reports in predominantly low-grade, type I histologies.5–7 13 14 A previous study by Chen et al evaluated the impact of hysteroscopy on disease-specific survival in a smaller number (n=54) of type II histology patients, also noting no difference in survival when compared with 86 patients undergoing dilation and curettage as part of their workup.30 In our cohorts, hysteroscopy and non-hysteroscopy groups had similar rates of adjuvant therapy, despite hysteroscopy being more common in early-stage disease. In our practice, adjuvant therapy may be completed in even early-stage high-grade disease, and may impact the risk of disease progression.27 While we did note a non-significant trend toward vaginal recurrences (HR 2.04 [95% CI 0.51, 8.18]) for stage I/II, it should be noted that small numbers were prohibitive, leading to a wide CI. Additionally, after stratifying by stage, an important confounding variable, we did not have sufficient number of stage III/IV patients with a hysteroscopy to evaluate a relationship between the timing of hysteroscopy and the risk of vaginal progression.
The strengths of our study included the largest single institution cohort of grade 3 endometrial cancer patients reported on to date, with follow-up of our patient population at a tertiary cancer care center with departmental standardization of surgical staging practices. Lastly, we hypothesized that tubal ligation may prevent intraperitoneal spillage of cells, and confounded results between groups. Therefore, we performed a sensitivity analysis by excluding the 21 patients with previous tubal ligation in the hysteroscopy group, and indeed our findings did not change. Limitations of our study included a limited number of advanced stage patients undergoing hysteroscopy, which prohibits inference of our findings to their clinical course. Indeed, the molecular alterations may be more aggressive and conducive to the seeding of metastasis in patients with more advanced stage disease,26 39 40 and the peritoneal dissemination of these cells via hysteroscopy may still pose a yet-undetected risk.
When interpreted within the context of previous studies, our study does not suggest an adverse impact on the incidence of positive cytology, spread of peritoneal disease, post-operative disease progression, or survival in predominantly early-stage high-risk endometrial cancer. Based on our findings, we suggest further large confirmatory studies at other institutions to ensure the safety of hysteroscopy when used in the workup of patients ultimately diagnosed with advanced- stage or high-grade disease.
References
Footnotes
Contributors All authors contributed meaningfully to the conception, design, data interpretation, manuscript preparation, and revision of this study.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. Deidentified participant data may be obtained after appropriate data use agreements between institutions.