Article Text

Abstract
Objective To evaluate the outcomes of minimally invasive surgery for patients with stage IA cervical carcinoma undergoing hysterectomy.
Methods Patients with pathological stage IA (IA1, IA2, IA not otherwise specified) squamous, adenocarcinoma, adenosquamous carcinoma of the cervix, no history of another tumor, who underwent radical or simple hysterectomy with known mode of surgery, diagnosed between 2010 and 2015 with at least 1 month of follow-up, were drawn from the National Cancer Database. Comparisons of demographic and clinicopathologic characteristics were made with the χ2 test. The impact of minimally invasive surgery (robotic-assisted or traditional laparoscopic) on overall survival was assessed with the log-rank test following generation of Kaplan–Meier curves. A Cox model was constructed to control for confounders.
Results A total of 1930 patients were identified; the majority (73.3%, 1414 patients) had stage IA1 disease, while 458 (23.7%) patients had stage IA2, and 58 (3%) patients had stage IA not otherwise specified. In the present cohort, 685 patients (35.5%) had open, 438 patients (22.7%) had laparoscopic, and 807 patients (41.8%) had robotic-assisted laparoscopic hysterectomy. Patients who had an open approach were more likely to undergo lymphadenectomy (58.1% vs 52.7%, p=0.021) and have radical hysterectomy (42% vs 32.4%, p<0.001). Patients who had minimally invasive surgery had a shorter hospital stay (median 1 vs 3 days, p<0.001). There was no difference in overall survival between patients who had open and minimally invasive hysterectomy (p=0.87); 4-year overall survival rates were 97.7% and 98.6%, respectively. There was no difference in overall survival between the open and minimally invasive surgery groups for patients who had simple (p=0.61; 4-year overall survival rates 97.6% and 98.7%, respectively) or radical hysterectomy (p=0.70; 4-year overall survival rates 97.8% and 98.4%, respectively). After controlling for patient age, tumor histology, and presence of lymphovascular invasion, minimally invasive hysterectomy was not associated with worse survival (HR 0.94, 95% CI 0.49 to 1.81). In a sensitivity analysis, based on 3048 patients with clinical stage IA after controlling for confounders, minimally invasive surgery was not associated with worse survival than laparotomy (HR 1.06, 95% CI 0.65 to 1.72).
Conclusions In a large cohort of patients with stage IA cervical carcinoma, performance of minimally invasive hysterectomy was not associated with a detrimental effect on overall survival.
- cervical cancer
- laparoscopes
- laparotomy
- hysterectomy
Data availability statement
Data may be obtained from a third party and are not publicly available. Data obtained from the American College of Surgeons.
Statistics from Altmetric.com
HIGHLIGHTS
The optimal route of hysterectomy for stage IA cervical cancer is not known.
Among 1930 patients with stage IA cervical cancer, 1245 patients had minimally invasive hysterectomy.
Overall survival was comparable between the laparoscopy and laparotomy groups.
Introduction
Cervical cancer is the third most common gynecologic malignancy in the USA with a decreasing incidence secondary to introduction of papilloma virus vaccination and Pap screening.1 For the majority of patients presenting with early-stage disease (International Federation of Gynecology and Obstetrics (FIGO) 2018, stage IA1, IA2 or IB1), simple or radical hysterectomy can be curative.2 Based on retrospective studies, minimally invasive surgery is associated with lower blood loss, decreased rate of post-operative complications, faster recovery, and shorter inpatient stay.3 However, for patients with FIGO 2009 stage IA1 with lymphovascular invasion, IA2 or IB1 cervical cancer who underwent radical hysterectomy, a recent randomized trial reported worse progression-free survival for those who had a minimally invasive hysterectomy.4 These results were also confirmed by a large number of retrospective studies showing a negative impact of minimally invasive radical hysterectomy.5 While recent clinical practice guidelines discourage the performance of minimally invasive radical hysterectomy for cervical cancer, the question remains whether a minimally invasive approach could potentially be considered for patients with small or microscopic tumors, especially for those who undergo simple hysterectomy.6 7 Unfortunately, given the very low incidence of cervical cancer, the majority of retrospective studies group patients with stage IA disease with those with stage IB disease and do not have sufficient statistical power to detect potential differences in relapse or death rates for this sub-group.8–12 The aim of the present study is to investigate the use of minimally invasive surgery and overall survival of patients with stage IA cervical carcinoma who underwent simple or radical hysterectomy using a large hospital-based database.
Methods
The National Cancer Database was accessed and patients without a history of another tumor diagnosed with microscopically confirmed invasive squamous, adenosquamous carcinoma, or adenocarcinoma of the cervix between January 2010 and December 2015 who had at least 1 month of follow-up were identified. Patients who underwent simple or radical hysterectomy (based on site-specific surgery codes) and had pathological stage IA disease (based on the 2018 FIGO staging schema) with known mode of surgery (open or minimally invasive) were selected for further analysis. Possible stage misclassified cases were excluded by cross-checking with the 'tumor extension', 'tumor size' (excluding tumors >7 mm in diameter), 'metastasis at diagnosis', and 'lymph node metastases' variables.
The National Cancer Database is a hospital-based database capturing approximately 70% of all malignancies diagnosed in the USA. The American College of Surgeons and the Commission on Cancer have not verified and are not responsible for the analytical or statistical methodology employed, or the conclusions drawn from these data. The present study was deemed exempt from Institutional Board Review from Penn Medicine (Protocol #829268).
Demographic, clinicopathological, and treatment characteristics were extracted from the de-identified dataset. For analysis purposes, insurance status was recoded into Private, Government (including Medicaid and Medicare), and Uninsured/Unknown. In addition, based on the median age of menopause in the USA, patient age was dichotomized into ≤50 and >50 years while the presence of co-morbidities was assessed from the Charlson–Deyo Comorbidity index and classified as absent (score 0) or present (score ≥1). Patients who underwent another surgical procedure before hysterectomy were identified. While the National Cancer Database does not collect details on the first surgical procedure, the assumption was made that cold knife cone or loop electrode excision procedures were performed.
The frequency of distribution of categorical variables was compared with the χ2 test and continuous variables with the Kruskall–Wallis test. Overall survival, defined in the National Cancer Database as months from diagnosis to death or censoring, was assessed following generation of Kaplan–Meier curves and compared with the log-rank test. A Cox model was constructed to control for patient age, presence of lymphovascular invasion, and histology. We conducted a sensitivity analysis to evaluate a more relevant clinical scenario by identifying patients diagnosed with clinical stage IA disease with no history of another tumor, who underwent simple or radical hysterectomy with known mode of surgery and at least 1 month of survival, and compared their survival. All statistical analyses were performed with the Statistical Package for the Social Sciences v.27 (IBM Corp, Armonk, New York, USA) and the α level of statistical significance was set at 0.05.
Results
A total of 1930 patients who met the inclusion criteria were identified; the majority (73.3%, 1414 patients) had stage IA1 disease, while 458 (23.7%) patients had stage IA2, and 58 (3%) patients had stage IA not otherwise specified. Median patient age was 43 years (range 22–87), and the majority were white (81.4%), had private insurance (63%), and squamous histology (68.3%). A total of 1238 (64.1%) patients underwent a simple hysterectomy and 692 (35.9%) patients had a radical hysterectomy. The rate of radical hysterectomy was higher among patients with stage IA2 disease compared with those with stage IA1 disease (53.3% vs 30.4%, p<0.001). Radiation therapy was rarely administered (28 cases, 1.5%). A total of 1225 (64.6%) patients underwent a surgical procedure before hysterectomy. Median time between first surgical procedure and hysterectomy was 39 days (IQR 57).
In the present cohort, 35.5% (685 patients) had open, 22.7% (438 patients) had laparoscopic, and 41.8% (807 patients) had robotic-assisted laparoscopic hysterectomy. For patients undergoing minimally invasive hysterectomy, the overall conversion rate to open surgery was 1.7%: 3% for laparoscopic and 1% for robotic-assisted hysterectomy (p=0.019). The rate of minimally invasive hysterectomy for stage IA1 (65.6%) and IA2 (62.7%) disease were comparable (p=0.25). Table 1 shows the clinicopathological characteristics stratified by mode of surgery. The two groups were comparable in terms of patient age, race, insurance status, presence of co-morbidities, tumor histology, and presence of lymphovascular invasion. However, patients who had an open approach were more likely to undergo lymphadenectomy (58.1% vs 52.7%, p=0.021) and to have a radical hysterectomy (42% vs 32.4%, p<0.001).
Demographic and clinicopathological characteristics of patients with stage IA cervical carcinoma who had open or minimally invasive hysterectomy
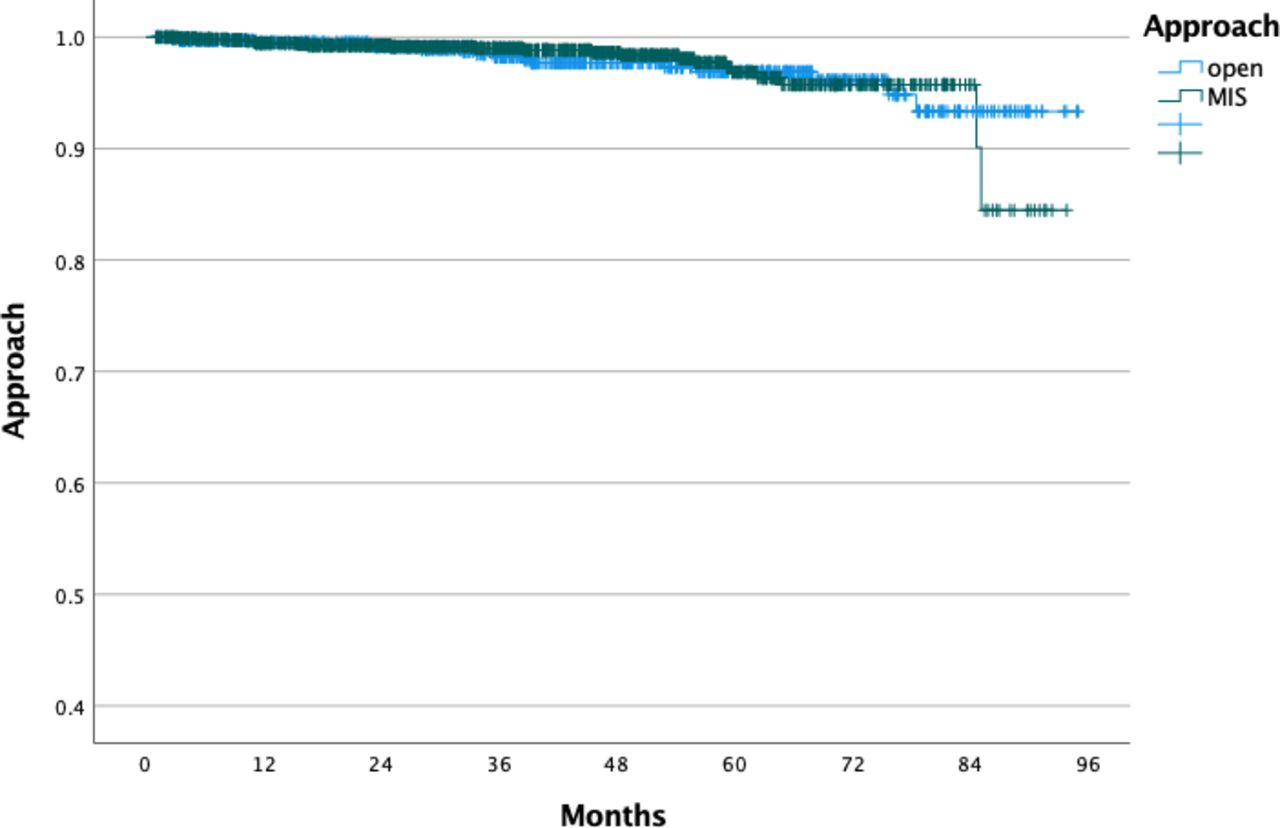
Patients who had minimally invasive hysterectomy had a shorter hospital stay (median 1 vs 3 days, p<0.001). The rate of unplanned re-admission 30 days from discharge were comparable between the open and minimally invasive groups (4.3% vs 2.8%, p=0.097). Based on the reverse Kaplan–Meier method, median follow-up was 38.1 months with 37 deaths observed. There was no difference in overall survival between the open (16 deaths) and minimally invasive (21 deaths) hysterectomy groups (p=0.87; 4-year overall survival rates 97.7% and 98.6%, respectively; Figure 1). After controlling for patient age, tumor histology, and the presence of lymphovascular invasion, minimally invasive surgery was not associated with worse survival (HR 0.94, 95% CI 0.49 to 1.81). There was no difference in overall survival between the open and minimally invasive surgery groups for patients who had simple (p=0.61; 4-year overall survival rates 97.6% and 98.7%, respectively) or radical hysterectomy (p=0.70; 4-year overall survival rates 97.8% and 98.4%, respectively). Similarly, following stratification by disease sub-stage, overall survival was comparable between the open and minimally invasive approach for patients with stage IA1 (p=0.76; 4-year overall survival rates 97.7% and 98.5%, respectively) and IA2 disease (p=0.93; 4-year overall survival rates 97.1% and 98.8%, respectively). Within the minimally invasive hysterectomy group there was no difference in overall survival between those who had robotically-assisted or traditional laparoscopic hysterectomy (p=0.83; 4-year overall survival rates 98.9% and 98.2%, respectively). Lastly, there was no difference in overall survival between patients who did and did not undergo a prior cervical surgical procedure (p=0.40; 4-year overall survival rates 98.5% and 98%, respectively).

Overall survival of patients with pathological stage IA cervical carcinoma who underwent hysterectomy based on route of surgery. MIS, minimally invasive surgery.
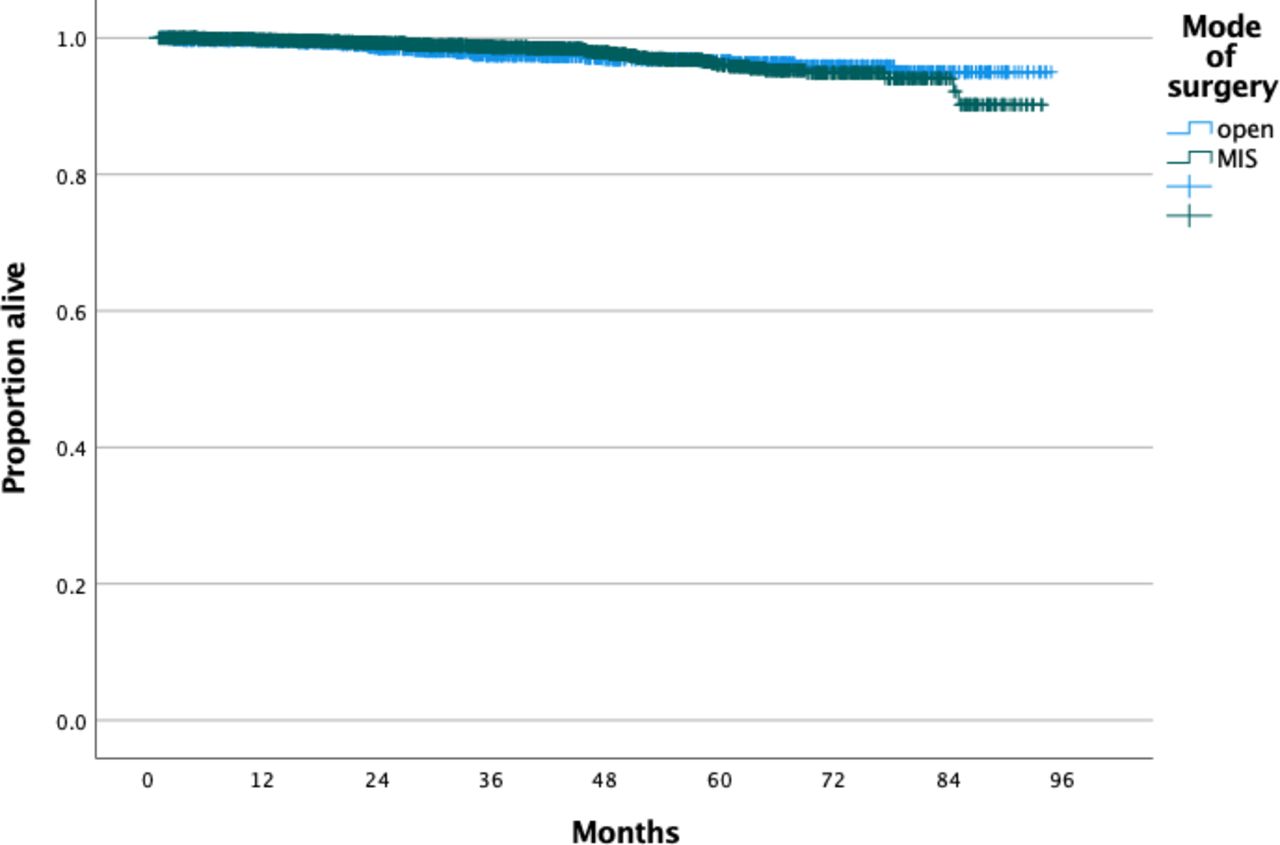
In evaluating a clinically oriented scenario, a total of 3048 patients with clinical stage IA were identified: 58.7% (1789) with IA1, 19.4% (590) with IA2, and 21.9% (669) with IA not specified. The majority of patients had simple hysterectomy (67.4%). Minimally invasive hysterectomy was performed for 2006 cases (65.8%) while 1042 (34.2%) patients had open surgery. There was no difference in overall survival between the open and minimally invasive hysterectomy groups (p=0.99; 4-year overall survival rates 96.9% and 97.9%, respectively; Figure 2). After controlling for patient age, tumor histology, and the presence of lymphovascular invasion, minimally invasive surgery was not associated with worse survival than laparotomy (HR 1.06; 95% CI 0.65 to 1.72). Data on the final pathological stage were available for 2196 patients; upstaging occurred for 18.2% and 14.8% of patients who had open and minimally invasive hysterectomy, respectively (p=0.041). Among patients who underwent lymphadenectomy, rates of positive lymph nodes were 4.2% and 3.4% in the open and minimally invasive hysterectomy groups, respectively (p=0.43).

{kind=link}
{kind=link}
Overall survival of patients with clinical stage IA cervical carcinoma who underwent hysterectomy based on route of surgery. MIS, minimally invasive surgery.
Discussion
Summary of Main Results
In a large cohort of patients with stage IA cervical carcinoma who underwent simple or radical hysterectomy, the 4-year overall survival rate was 98.3%. The majority of patients underwent minimally invasive hysterectomy. Median hospital stay was shorter for patients who had minimally invasive hysterectomy, while they did not have worse overall survival after controlling for confounders compared with those who had a laparotomy. In our sensitivity analysis we evaluated a common clinical scenario that surgeons may encounter—patients with clinical stage IA disease. Again, we found that minimally invasive surgery was not associated with worse survival compared with laparotomy in patients with stage IA disease, while the incidence of upstaging was overall comparable.
Results in the Context of Published Literature
Based on the current National Comprehensive Cancer Network guidelines, radical hysterectomy is recommended for patients with stage IA1 disease with lymphovascular invasion or those with stage IA2 disease, while simple hysterectomy is sufficient for patients with stage IA1 disease without lymphovascular invasion.2 The SHAPE randomized trial is currently investigating the oncologic safety of simple hysterectomy for patients with low-risk cervical carcinoma defined as stage IA2 or IB1, with tumor size <2 cm, at least 3 mm of intact cervical stroma, and <50% stromal invasion.13 If simple hysterectomy is established as the standard of care for all patients with stage IA disease, selecting the route of hysterectomy will be challenging in light of the results of the LACC trial.4 The CONCERV trial is also investigating conservative and fertility-sparing options in this patient population.14
Nevertheless, since the LACC trial investigated the outcomes of radical hysterectomy, it is unclear if it can be fully extrapolated to patients undergoing simple hysterectomy. In addition, in that trial only 10 and 41 patients had stage IA1 and stage IA2 disease, respectively.4 Given the lack of statistical power, investigators concluded that the results of the LACC trial cannot be applied to patients with low-risk tumors (tumor size <2 cm, no lymphovascular invasion, depth of invasion <10 mm).4 Similarly, the majority of studies comparing the oncologic outcomes of patients with cervical cancer undergoing radical hysterectomy based on route of surgery include a very small number of patients with stage IA disease. For example, a large retrospective cohort from the USA included only four patients with stage IA1 disease and 33 patients with stage IA2 disease.8 Similarly, in an analysis of the Swedish Cancer Registry, only 30 patients with stage IA disease were identified.10 A prior analysis of the National Cancer Database identified 155 and 157 patients with stage IA2 who underwent minimally invasive and open radical hysterectomy, respectively.12 Given the very low incidence of relapse among patients with stage IA disease, all these studies were not powered to detect a statistically significant difference between the open and minimally invasive surgery groups. In addition, we should underline that, to date, no study has compared outcomes of open and minimally invasive simple hysterectomy for patients with stage IA1 disease.
It has not been established whether the worse oncologic outcomes observed for patients undergoing minimally invasive surgery are related to the use of a uterine manipulator, intra-abdominal spread of tumor cells during colpotomy, or inadequate surgical technique.6 7 However, the presence of gross tumor appears to play an important role. For patients who have no visible tumor following cold knife cone, a recent study demonstrated comparable outcomes between the open and minimally invasive routes. Uppal et al analyzed 243 patients who underwent conization and had no residual tumor on pre-operative imaging; there was no difference in relapse rate between the open (n=72) and minimally invasive surgery groups (n=171) (1.4% vs 2.9%, p=0.48).8 In an analysis of the SUCCOR multi-institutional study, which included 1156 patients with stage IB1 cervical cancer undergoing radical hysterectomy, 733 underwent cold knife cone.15 Following propensity score matching, cold knife cone was associated with a 65% reduction in the risk of relapse.15 Another multi-institutional study demonstrated a significant correlation between the presence of gross cervical tumor at the time of surgery and risk of relapse.16 Casarin et al identified 186 patients with stage IA1–IB1 disease who underwent minimally invasive radical hysterectomy and reported that performance of pre-operative conization was associated with a lower risk of relapse (1.1% vs 16.1%, p<0.001) even for patients with stage IB1 disease (1.8% vs 17.2%, p=0.004). Interestingly, no relapses were noted for patients with stage IA1–IA2 disease.16 Data from these studies potentially support the use of minimally invasive surgery for patients with stage IA disease since, by definition, no visible tumor is present, while many of them undergo pre-operative cold knife cone to determine the exact tumor spread to plan a definitive surgical approach.
Strengths and Weaknesses of the Study
A major strength of the present study was the large number of patients identified from a multi-institutional database. Several limitations should be mentioned. Given the absence of central pathology review, possible histology or stage misclassifications cannot be excluded. In addition, the National Cancer Database does not collect data on tumor relapse or cause of death, precluding us from analyzing differences in progression-free and cause-specific survival or patterns of relapse. Moreover, specific details on uterine size or patient’s surgical history that could have influenced the surgeon’s decision on the route of hysterectomy were not available. Lastly, while we were able to identify patients who underwent a surgical procedure before hysterectomy, the exact details of the surgical procedure were not available, although we hypothesize that they underwent cold knife cone or loop electrode excision as part of their surgical planning work-up (to determine type of hysterectomy).
Implications for Practice and Future Research
Our study should be regarded as hypothesis-generating and stimulate an international collaboration to investigate the optimal route of hysterectomy for this patient population. Given the low relapse rate observed for patients with stage IA disease, a prospective randomized trial may be difficult to accrue an adequate number of patients. A multi-institutional retrospective study is feasible, and we invite authors of large studies that have already been published to join our efforts and pool their individual patient-level data.
Conclusions
In a large cohort of patients with cervical carcinoma and stage IA disease who underwent hysterectomy, minimally invasive surgery was not associated with worse overall survival. Patients with microscopic cervical cancer may benefit from a minimally invasive approach.
Supplemental material
Data availability statement
Data may be obtained from a third party and are not publicly available. Data obtained from the American College of Surgeons.
Ethics statements
References
Footnotes
Contributors DN: conception, data acquisition, data management, statistical analysis, critical analysis, drafting/final editing. MB, EMK, AFH, LC, SK, RLG: critical analysis, drafting/final editing. NL: supervision, critical analysis, drafting/final editing.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.