Article Text

Abstract
Background Early stage cervical cancer is prevalent in China and remains a major public health burden in developing countries. We aimed to determine the long term oncologic outcomes between laparoscopic and abdominal radical hysterectomy in patients with early cervical cancer.
Methods We conducted a multicenter, retrospective, case-control study of 37 hospitals. All consecutive early stage cervical cancer patients with International Federation of Gynecology and Obstetrics (FIGO) 2009 stage IA1 with lymphovascular space invasion to IB1, who underwent laparoscopic or abdominal radical hysterectomy between January 2004 and December 2016, were included. We compared the disease free survival and overall survival of the two approaches in 1:1 case-control matched settings based on prognosis related factors.
Results We selected 8470 of 46 313 patients. After matching (n=1601/1601), we found that laparoscopic surgery was associated with significantly worse 5 year disease free survival (89.5% vs 93.1%, p=0.001; hazard ratio (HR) 1.60, p=0.001), but not 5 year overall survival (94.3% vs 96.0%, HR=1.48, p=0.058). In the subgroup analysis, in patients with a tumor diameter <2 cm (n=739/739), both 5 year disease free survival and overall survival were similar between the laparoscopic and abdominal radical hysterectomy groups. However, when tumor diameter was 2–4 cm (n=898/898), laparoscopic surgery was a poor prognosis risk factor for 5 year disease free survival (84.7% vs 90.8%, p=0.001; HR=1.81, p<0.001), but not 5 year overall survival (90.9% vs 93.8%, p=0.077; HR=1.53, p=0.059).
Conclusions In patients with early cervical cancer, laparoscopic radical hysterectomy was associated with significantly poorer long term oncologic outcome, although in patients with tumors <2 cm, the 5 year overall survival and 5 year disease free survival were similar.
- cervical cancer
- laparoscopes
- laparotomy
Statistics from Altmetric.com
HIGHLIGHTS
Laparoscopic radical hysterectomy was associated with a poor prognosis in early stage cervical cancer.
Laparoscopic radical hysterectomy was associated with worse disease free survival for patients with 2–4 cm tumors.
Survival outcome was similar in patients with a tumor diameter <2 cm.
Introduction
Cervical cancer is the most common gynecologic cancer in developing countries, and 90% of fatalities occur in these regions, with cervical cancer related death being the third cause of death after breast cancer and lung cancer.1 Each year, 98 900 new cases of cervical cancer are diagnosed in China, and 30 500 people die from this disease.2 Radical hysterectomy and lymphadenotomy has become the standard strategy for treating early stage cervical cancer (International Federation of Gynecology and Obstetrics (FIGO) 2009 stage IA1 with lymphovascular space invasion, IA2, and IB1).3 4 Five year survival may be up to 87% when patients are managed by surgery.5 Currently, most studies focus on minimizing morbidity while maintaining the best oncologic outcomes. Hence minimally invasive approaches, such as laparoscopy and robot assisted surgery, have been routinely used until recently when concerns regarding poorer survival outcomes were noted with this approach.
Conventional surgical approaches for cervical cancer include abdominal radical hysterectomy, minimally invasive (laparoscopic or robotic assisted) radical hysterectomy, or vaginal radical hysterectomy. Previously published data reported that laparoscopic radical hysterectomy significantly reduced perioperative complication rates and days of hospital stay.3 4 However, according to a recently published randomized trial and several observational cohort studies, higher rates of death and recurrence by minimally invasive surgery raises major concerns about the safety of this approach.6 7 As a highly prevalent malignant tumor in China, a large number of patients with cervical cancer are available for evaluating the impact of laparoscopic or abdominal radical hysterectomy on oncologic outcomes.
Hence we gathered 37 hospitals where both laparoscopic and abdominal radical hysterectomy in mainland China are performed, and established a clinical database of cervical cancer. The aim of this study was to compare the difference in 5 year disease free survival and overall survival in patients undergoing laparoscopic or abdominal radical hysterectomy.
Methods
China Cervical Cancer Clinical Database
We examined all patients with cervical cancer between January 2004 and December 2016, and obtained their complete medical data. This retrospective study was approved by the ethics committee of Nanfang Hospital, Southern Medical University (ethical No NEEC-2017–135, clinical trial No CHiCTR1800017778 (International Clinical Trials Registry Platform Search Port, http://apps.who.int/trialsearch/)). Details of this database have been described previously.8 Follow-up was performed through telephone calls only, and information on survival, recurrence status, and complications were obtained. When telephone contact was not possible, we extracted information from the inpatient/outpatient medical records. The date of the latest record was considered as the last valid follow-up date. All original data were double checked and verified by two independent gynecologists to assure accuracy.
Inclusion and Exclusion Criteria
The selection of patients for our study was determined by the following criteria: age ≥18 years; early stage cervical cancer (FIGO 2009 stage IA1 with lymphovascular space invasion, IA2, and IB1); squamous cell carcinoma, adenocarcinoma, and adenosquamous carcinoma; primary laparoscopic radical hysterectomy or abdominal radical hysterectomy; Querleu–Morrow type B/C radical hysterectomy in combination with pelvic and/or para-aortic lymphadenotomy; and complete pathology report. We excluded patients who underwent neoadjuvant therapy or those lost to follow-up. In the matching cohort, we also excluded those with non-standard postoperative adjuvant therapy. Standard postoperative adjunct therapy was defined according to the Sedlis criteria9 as patients with no or one intermediate risk factor and who did not receive any postoperative therapy, and those with two or three intermediate risk factors or any high risk factors and who received postoperative radiotherapy or chemoradiotherapy. Intermediate risk factors included tumor size >4 cm, cervical stroma invasion >1/2, and lymphovascular space invasion. High risk factors included lymph node metastasis, vaginal margin positive, and parametrial invasion. Non-standard postoperative therapy was defined as patients with two or three intermediate risk factors or any high risk factors but who did not receive any postoperative therapy or with no or one intermediate risk factor but who received any postoperative therapy. Pregnant patients or those with a secondary malignant disease were also excluded. In the subgroup analysis, all patients were subdivided into two groups according to the diameter of the tumor: tumor diameter <2 cm and tumor diameter 2–4 cm.
Case Matching
Because the baseline characteristics of the patients were significantly different, we used a 1:1 case-control matching procedure to ensure between group balance. The variables included age, FIGO stage, year of diagnosis, histopathological subtype, lymphovascular space invasion status, depth of stromal invasion, lymph node metastasis, vaginal margin status, and parametrial invasion status.
Outcome Measurement
The main outcomes endpoints of this study were 5 year disease free survival and overall survival. Disease free survival was defined as the date of diagnosis to the date of death from any cause, the date of recurrence, or the last valid follow-up. Overall survival was defined as the date of diagnosis to the date of death from any cause or the last valid follow-up.
Statistics
All statistical procedures were performed by Statistical Product and Service Solutions (SPSS) statistical software (V.23.0, SPSS Inc, Chicago, Illinois, USA). The between group differences in baseline characteristics were assessed using the Student's t test, a Mann–Whitney U test, Pearson's χ2 test, and Fisher's exact test. Quantitative data are shown as mean (±standard deviation (SD)), and nominal scale data are shown as percentage (%). We considered a p value of <0.05 to be statistically significant. In multivariate analysis, we included the following factors into the model: age, FIGO staging (IA1 (lymphovascular space invasion positive) and IA2, IB1), histopathological subtypes (squamous cell carcinoma, adenocarcinoma, adenosquamous carcinoma), year of diagnosis (2004–2009, 2010–2016), cervical stroma invasion status (≤1/2, >1/2, or unknown), lymphovascular space invasion status (negative, positive), lymph node metastasis (negative, positive), vaginal margin status (negative, positive), parametrial invasion status (negative, positive), and adjuvant therapy (no, yes). All statistics were reviewed under the guidance of a statistician.
Results
We collected a total of 46 313 patients from 37 hospitals into our database. We then selected 8470 patients with early stage cervical cancer for the non-matching cohort. Considering that baseline differences existed between the two groups, the selection of patients was statistically processed by 1:1 case-control matching according to prognosis related factors. We also conducted a subgroup analysis to obtain a more robust result. The process of study selection is shown in Figure 1.

Study selection. IA1, IA2, and IB1, International Federation of Gynecology and Obstetrics (FIGO) 2009 stage. AC, adenocarcinoma; ARH, abdominal radical hysterectomy; ASC, adenosquamous carcinoma; LRH, laparoscopic radical hysterectomy; LVSI, lymphovascular space invasion; SCC, squamous cell carcinoma.
Long Term Oncological Outcomes Before Matching
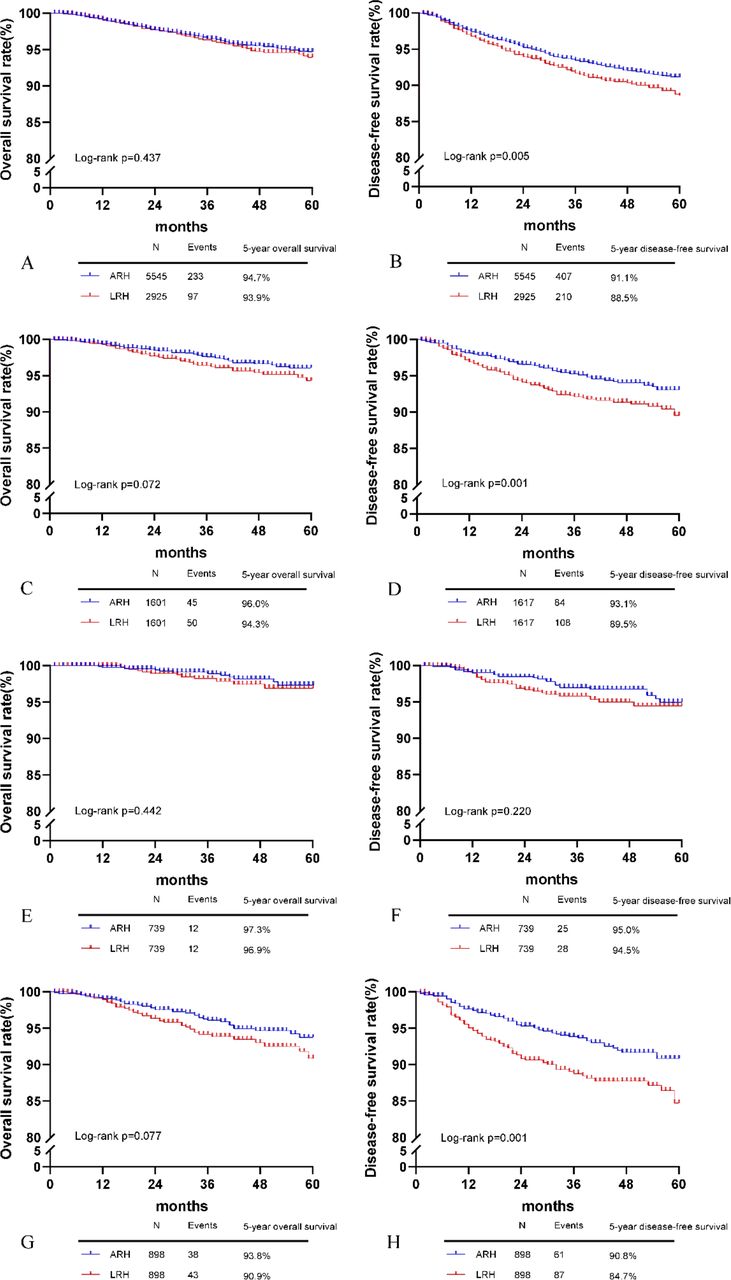
For the non-matching cohort of 8470 patients (laparoscopic radical hysterectomy n=2925, abdominal radical hysterectomy n=5545), we conducted a survival analysis regardless of the imbalanced baseline characteristics (online supplementary Table 1). The median follow-up time of the non-matching cohort was 42 months (range 1–172). In this group, the number of deaths at 5 years in patients who underwent laparoscopic and abdominal radical hysterectomy were 97 (3.3%) and 233 (4.2%), respectively. Laparoscopic radical hysterectomy was associated with a worse 5 year disease free survival (88.5% vs 91.1%, p=0.005; Figure 2B) but not a worse 5 year overall survival (93.9% vs 94.7%) compared with the open approach (p=0.44) (Figure 2A). In the multivariate Cox analysis (online supplementary Table 2), laparoscopic radical hysterectomy was identified as an independent risk factor for poorer disease free survival (hazard ratio (HR) 1.31; 95% confidence interval (CI) 1.10 to 1.57; p=0.002).
Supplemental material
Supplemental material
{kind=link}
{kind=link}
Survival outcomes, including overall survival and disease free survival. For the non-matching cohort, overall survival (A) and disease free survival (B). For the 1:1 matched group, overall survival (C) and disease free survival (D). For the tumor diameter <2 cm group, overall survival (E) and disease free survival (F). For the tumor diameter 2–4 cm group, overall survival (G) and disease free survival (H). ARH, abdominal radical hysterectomy; LRH, laparoscopic radical hysterectomy.
Survival Analysis of 1:1 Matched Group
After excluding patients with two or three intermediate risk factors or any high risk factors but who did not receive any postoperative therapy, or with no or one intermediate risk factor but who received any postoperative therapy, 4821 early stage cervical cancer patients (laparoscopic radical hysterectomy n=1634, abdominal radical hysterectomy n=3187) entered a 1:1 case-control matching cohort. Median follow-up time in this group was 42 months (range 1–172). After matching, the baseline characteristics of patients who received laparoscopic radical hysterectomy or abdominal radical hysterectomy (n=1601/1601) were all balanced (Table 1). In this matched cohort, the 5 year disease free survival in the laparoscopic radical hysterectomy group was worse but not 5 year overall survival (5 year overall survival: 94.3% vs 96.0%, p=0.072, Figure 2C; 5 year disease free survival: 89.5% vs 93.1%, p=0.001, Figure 2D). Multivariate Cox analysis (online supplementary Table 3) also showed that laparoscopic radical hysterectomy was associated with worse disease free survival but not overall survival (disease free survival: HR 1.605, 95% CI 1.205 to 2.138, p=0.001 and overall survival: HR 1.483, 95% CI 0.987 to 2.228, p=0.058).
Supplemental material
Baseline characteristics of the 1:1 matched group
Survival Analysis of Patients with Tumor Diameter Less Than 2 cm After Matching
Median follow-up time in this subgroup was 42 months (range 1–169). After matching, 739 patients with a tumor diameter <2 cm were evaluated. All baseline differences were eliminated (Table 2). The negative effect of laparoscopic radical hysterectomy on survival was no longer demonstrated in this group (5 year overall survival: 96.9% vs 97.3%, p=0.44; 5 year disease free survival: 94.5% vs 95.0%, p=0.22; Figure 2E,F). Cox analysis (online supplementary Table 4) found that laparoscopic radical hysterectomy was not an independent risk factor in this subgroup.
Supplemental material
Baseline characteristics of the tumor diameter <2 cm group
Survival Analysis of Patients with Tumor Diameter 2-4cm After Matching
In this subgroup with a median follow-up time of 40 months (range 1–168), 898 patients with a tumor diameter of 2–4 cm were evaluated and baseline differences are shown in Table 3. Laparoscopic radical hysterectomy was associated with worse outcomes than abdominal radical hysterectomy in terms of 5 year disease free survival (84.7% vs 90.8%, p=0.001; Figure 2G) but not 5 year overall survival (90.9% vs 93.8%, p=0.08; Figure 2H). In Cox analysis (online supplementary Table 5), laparoscopic radical hysterectomy was an independent risk factor for poorer disease free survival (HR=1.81, 95% CI 1.29 to 2.51, p<0.001).
Supplemental material
Baseline characteristics of the tumor diameter 2–4 cm group
Discussion
This multicenter retrospective cohort study conducted in 37 hospitals in mainland China indicated that in the non-matching cohort, patients with early stage cervical cancer (FIGO 2009 IA1 with lymphovascular space invasion, IA2, and IB1) who underwent laparoscopic radical hysterectomy had a worse disease free survival but similar overall survival compared with those who underwent open radical hysterectomy. After exclusion of patients who received non-standard postoperative adjuvant therapy and a 1:1 matching, laparoscopic radical hysterectomy was a poor prognosis factor for early stage cervical cancer patients. In the subgroup analysis, in patients with a tumor diameter <2 cm, laparoscopic radical hysterectomy was not a predictor for poorer oncological outcome. However, laparoscopic radical hysterectomy was associated with worse disease free survival in patients with a tumor size of 2–4 cm. As the design of this study was based on a large number of patients, we observed similar results for laparoscopic radical hysterectomy in both the matched and non-matching cohorts, and we conclude that, for early stage cervical cancer, laparoscopic radical hysterectomy is associated with worse disease free survival.
Although laparoscopic radical hysterectomy has been used in the management of patients with cervical cancer for more than 30 years,10 recently, several studies have strongly questioned the impact of laparoscopic radical hysterectomy in treating early stage cervical cancer. Ramirez et al conducted a multicenter, prospective, randomized, controlled trial that reported a 4.5 year overall survival rate of 96.5% after abdominal radical hysterectomy, while after laparoscopic radical hysterectomy it was 86.0%. This indicated a significantly lower survival rate of patients who underwent laparoscopic radical hysterectomy compared with those who underwent open abdominal radical hysterectomy.6 Another study conducted by Melamed et al extracted data from two large national databases that confirmed a significantly higher risk of death from laparoscopic radical hysterectomy, but could not further compare the survival of low risk patients.7 A single center study by Kim et al confirmed that laparoscopic radical hysterectomy was associated with worse disease free survival but not worse overall survival, while a subgroup analysis suggested that the rates of overall survival and disease free survival were similar in patients with FIGO IB1 and a tumor size <2 cm.11 Other retrospective cohort studies also revealed similar results.12–17 However, a recently published multi-institutional study by Uppal and colleagues revealed that minimally invasive surgery was associated with higher recurrences, even in patients with a tumor size ≤2 cm. Of note, a high proportion of patients in this study were treated by robotic surgery.18
To our knowledge, ours is the largest cohort study comparing the survival of laparoscopic and abdominal radical hysterectomy in cervical cancer to date. Our study provided information on a subgroup of patients with a tumor diameter <2 cm. The limitations of our study included the fact that we were restricted by the limited means of follow-up; we could not obtain all information regarding the time and site of recurrence for approximately 7–8% of patients. However, given the size of our cohort, we considered that this should not negatively affect the results. We were unable to clarify the mechanism by which laparoscopic radical hysterectomy was associated with a worse prognosis. As a retrospective study, a number of confounding factors might cause bias, and therefore we applied multiple methods to balance all confounding factors to ensure that the results were reliable.
In conclusion, laparoscopic radical hysterectomy was associated with a significantly higher risk of death and recurrence in patients with early stage cervical cancer, especially in those with a tumor diameter of 2–4 cm. Although our study did not show a negative impact of laparoscopic radical hysterectomy on patients with a tumor diameter <2 cm, we consider that laparoscopic radical hysterectomy in this subgroup of patients should be performed with great caution and consideration of prospective studies is needed.
Acknowledgments
We are grateful to Wuliang Wang (Department of Obstetrics and Gynecology, The Second Affiliated Hospital of Zhengzhou University), Ying Yang (Department of Obstetrics and Gynecology, Xinqiao Hospital, Army Medical University), Shan Kang (Department of Obstetrics and Gynecology, The Forth Hospital of Hebei Medical University), Bin Ling (Department of Obstetrics and Gynecology, China-Japan Friendship Hospital), Xinli Sun and Hongwei Zhao (Department of Gynecology, Shanxi Cancer Hospital), Lizhi Liang and Jihong Liu (Department of Gynecologic Oncology, Sun Yat-sen University Cancer Center), Yu Guo and Lihong Lin (Department of Gynecology, Anyang Tumor Hospital), Li Wang (Department of Gynecology, The Affiliated Tumor Hospital of Zhengzhou University), Weidong Zhao (Department of Gynecology and Oncology, Anhui Provincial Cancer Hospital), Yan Ni (Department of Obstetrics and Gynecology, The Yuncheng Central Hospital of Shanxi Province), Donglin LI and Wentong Liang (Department of Obstetrics and Gynecology, Guizhou Provincial People's Hospital), Jianxin Guo (Department of Obstetrics and Gynecology, Research Institute of Surgery, Daping Hospital, The Third Military Medical University), Shaoguang Wang (Department of Gynecology, The Affiliated Yantai Yuhuangding Hospital of Qingdao University), Xuemei Zhan and Mingwei Li (Department of Gynecology, Jiangmen Central Hospital), Weifeng Zhang (Department of Obstetrics and Gynecology, Ningbo Women and Children's Hospital), Peiyan Du (Department of Gynecological Oncology, the Affiliated Cancer Hospital and Institute of Guangzhou Medical University), Ziyu Fang (Department of Obstetrics and Gynecology, Liuzhou Workers' Hospital), Rui Yang (Department of Obstetrics and Gynecology, Shenzhen Hospital of Peking University), Long Chen (Department of Obstetrics and Gynecology, Qingdao Municipal Hospital), Encheng Dai and Ruilei Liu (Department of Obstetrics and Gynecology, Linyi People's Hospital), Mubiao Liu and Yuanli He (Department of Obstetrics and Gynecology, Zhujiang Hospital, Southern Medical University), Jilong Yao (Department of Obstetrics and Gynecology, Shenzhen Maternity and Child Health Hospital), Xueqin Wang (Department of Obstetrics and Gynecology, The Fifth Affiliated Hospital of Southern Medical University), Anwei Lu (Department of Obstetrics and Gynecology, Maternal and Child Health Hospital of Guiyang Province), Shuangling Jin (Department of Obstetrics and Gynecology, Peace Hospital affiliated to Changzhi Medical College), Yan Xu (Department of Obstetrics and Gynecology, Guangzhou Pan Yu Central Hospital), Ben Ma (Department of Obstetrics and Gynecology, Guangzhou First People's Hospital), Zhonghai Wang (Department of Obstetrics and Gynecology, Shenzhen Nanshan People's Hospital), Lin Zhu (Department of Gynecology, The Second Hospital of Shandong University), Hongxin Pan (Department of Obstetrics and Gynecology, the Third Affiliated Hospital of Shenzhen University, Luohu People's Hospital), Qianyong Zhu (Department of Obstetrics and Gynecology, No153 Center Hospital of Liberation Army and Hospital No 988 of the Chinese People's Liberation Army Joint Support Force), Xiaohong Wang (Department of Obstetrics and Gynecology, Laiwu People's Hospital and Jinan City People's Hospital), Dingyuan Zeng and Zhong Lin (Department of Obstetrics and Gynecology, Maternal and Child Health Care Hospital of Liuzhou), Bin Zhu (Department of Gynecology, The Affiliated Yiwu Women and Children Hospital of Hangzhou Medical College), for providing the cases involved in this study.
References
Footnotes
JH, MH and PL contributed equally.
Contributors All authors approved the final version of the study. MH, JH, and PL contributed equally to the work. CC handled the protocol development, study supervision, and study design. MH collected and analyzed the data, and interpreted the results. JH collected the data and conducted the literature search. PL participated in the drafting of the original version of the manuscript. ZL collected the data. JL participated in the protocol development, study supervision, and study design. XB analyzed the data and interpreted the results. All authors participated in writing, review, editing of the manuscript.
Funding The study received funding from the National Science and Technology Support Program of China (2014BAI05B03), the National Natural Science Fund of Guangdong (2015A030311024), and the Science and Technology Plan of Guangzhou (158100075).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study was approved by the ethics committee of Nanfang Hospital, Southern Medical University (ethical No NEEC-2017–135, clinical trial No CHiCTR1800017778 (International Clinical Trials Registry Platform Search Port, http://apps.who.int/trialsearch/)).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information. The data are not published elsewhere. Data are available upon reasonable request.