Article Text

Abstract
Introduction Recently, the safety of minimally invasive surgery in the treatment of cervical cancer has been questioned. This study was designed to compare the disease-free survival and overall survival of abdominal radical hysterectomy and laparoscopic radical hysterectomy in patients with early-stage cervical cancer.
Methods A total of 1065 patients with early-stage cervical cancer who had undergone abdominal/laparoscopic radical hysterectomy between January 2013 and December 2016 in seven hospitals were retrospectively analyzed. The 1:1 propensity score matching was performed in all patients. Patients with tumor size ≥2 cm and <2 cm were stratified and analyzed separately. Disease-free survival and overall survival were compared between matched groups. After confirming the normality by the Shapiro-Wilks test, the Mann-Whitney U test and the χ2 test were used for the comparison of continuous and categorical variables, respectively. The survival curves were generated by the Kaplan-Meier method and compared by log-rank test.
Results After matching, a total of 812 patients were included in the disease-free survival and overall survival analyses. In the entire cohort, the laparoscopic radical hysterectomy group had a significantly shorter disease-free survival (HR 1.65, 95% CI 1.00 to 2.73; p=0.048) but not overall survival (HR 1.60, 95% CI 0.89 to 2.88; p=0.12) when compared with the abdominal radical hysterectomy group. In patients with tumor size ≥2 cm, the laparoscopic radical hysterectomy group had a significantly shorter disease-free survival (HR 1.93, 95% CI 1.05 to 3.55; p=0.032) than the abdominal radical hysterectomy group, whereas no significant difference in overall survival (HR 1.90, 95% CI 0.95 to 3.83; p=0.10) was found. Additionally, in patients with tumor size <2 cm, the laparoscopic radical hysterectomy and abdominal radical hysterectomy groups had similar disease-free survival (HR 0.71, 95% CI 0.24 to 2.16; p=0.59) and overall survival (HR 0.59, 95% CI 0.11 to 3.13; p=0.53).
Conclusion Laparoscopic radical hysterectomy was associated with inferior disease-free survival compared with abdominal radical hysterectomy in the entire cohort, as well as in patients with tumor size ≥2 cm. For the surgical treatment of patients with early-stage cervical cancer, priority should be given to open abdominal radical hysterectomy.
- laparotomy
- cervical cancer
- laparoscopes
- surgery
Statistics from Altmetric.com
HIGHLIGHTS
Laparoscopic radical hysterectomy had lower rates of disease-free survival but not overall survival in patients with early-stage cervical cancer.
Laparoscopic radical hysterectomy was associated with lower rates of disease-free survival but not overall survival in patients with tumor size ≥2 cm.
Laparoscopic and abdominal radical hysterectomy had similar disease-free survival and overall survival in patients with tumor size <2 cm.
Introduction
Cervical cancer ranks fourth for both incidence and mortality of female cancer in the world, with 569 847 new cases and 311 365 deaths reported in 2018.1 In China, cervical cancer ranks as the sixth leading cause of female cancer, with 98 900 new cases and 30 500 deaths reported in 2015.2 Before 2019, the guidelines of several authoritative societies recommended that radical hysterectomy with pelvic lymphadenectomy, either laparotomy (open surgery) or laparoscopy (minimally invasive surgery), was the standard surgical treatment for patients with stage IA2–IIA cervical cancer.3–5 However, a prospective, randomized controlled study, known as the Laparoscopic Approach to Cervical Cancer (LACC) trial, showed that patients who underwent minimally invasive radical hysterectomy for early-stage cervical cancer had lower rates of disease-free survival and overall survival than patients who underwent abdominal radical hysterectomy.6 This study prompted the authoritative societies to update the guidelines to support only open abdominal surgery in cervical cancer.7–9 After the LACC trial, the inferior survival outcomes associated with minimally invasive radical hysterectomy of cervical cancer were found in several retrospective studies.10–17 Contrarily, there were other retrospective studies that showed that the survival outcomes of minimally invasive surgery were not inferior to that of abdominal surgery in cervical cancer.18–23 In this study, we conducted a retrospective multicenter matching study involving seven hospitals in Southwest China in order to examine the disease-free survival and overall survival of early-stage cervical cancer patients undergoing laparoscopic radical hysterectomy versus abdominal radical hysterectomy; moreover, a separate analysis was conducted after dividing the patients according to tumor size.
Methods
This study was approved by the ethics committees of all the participating hospitals. In addition, written informed consent was obtained from each patient for data use. The participating hospitals included West China Second University Hospital, Sichuan University, Affiliated Hospital of Southwest Medical University, Affiliated Hospital of Zunyi Medical University, Affiliated Hospital of North Sichuan Medical College, People’s Hospital of Deyang City, Panzhihua Municipal Central Hospital, and The First People’s Hospital of Neijiang City. Patients with early-stage cervical cancer who had undergone laparoscopic radical hysterectomy or abdominal radical hysterectomy from January 2013 to December 2016 in these seven hospitals were retrospectively reviewed. There was no robotic case in this study. The surgeon’s preference and eventually the patient’s decision determined the surgical approach. Patients were eligible if they had pathologically diagnosed cervical cancer, had a diagnosis of FIGO (International Federation of Gynecology and Obstetrics) stage (2009) IA2, IB1 or IIA1 disease, and underwent laparoscopic or abdominal Piver-Rutledge type III radical hysterectomy and lymphadenectomy. Patients were excluded if they had neoadjuvant chemotherapy, incomplete medical recordings or irregular follow-up.
Two investigators (TH and YH) went to each hospital to collect the patient data, including demographic, clinical, as well as pathological information. We used preoperative magnetic resonance imaging or computed tomography to measure the tumor size. In patients without imaging data, the tumor size was clinically defined. Surgical treatment consisted of radical hysterectomy, bilateral salpingo-oophorectomy, and lymphadenectomy of the pelvic lymph nodes ± para-aortic lymph nodes. In the procedure of radical hysterectomy, the para-cervix was transected completely, including the part located caudal to the deep uterine vein. All patients underwent pelvic lymphadenectomy, including resection of the lymph nodes along the bilateral iliac vessels, around the obturator nerves, and in the parametrium. Para-aortic lymphadenectomy was performed in selected patients who were suspected to have metastasis to para-aortic lymph nodes during the intraoperative inspection. An intrauterine manipulator was used in all laparoscopic procedures; the decision about whether to seal the vagina before vaginal excision depended on the surgeon’s preference.
Patients would receive postoperative radiochemotherapy if the postoperative pathological results showed at least one of the following: tumor size >4 cm, poorly-differentiated tumor, stromal invasion >1/2, lymphovascular space invasion, positive pelvic nodes, positive surgical margin, positive parametrium, and/or positive para-aortic lymph nodes with no distant metastasis. All patients were followed either through telephone interviews or at outpatient clinics until October 2019. Disease-free survival was defined as the time interval between surgery and first recurrence or last follow-up. Overall survival was defined as the time interval between surgery and death or last follow-up.
We used the Statistical Package for the Social Sciences (SPSS) software, version 20.0 (International Business Machines (IBM) Corp, Armonk, NY, USA) to perform the survival analysis. After confirming the normality by the Shapiro-Wilks test, the Mann-Whitney U test and the χ2 test were used for the comparison of continuous and categorical variables, respectively. The survival curves were generated by the Kaplan-Meier method and compared by log-rank test. Considering that some variables may affect the survival outcome, we used the R software, version 3.3.6 (Vienna, Austria; https://www.r-project.org/) to perform one-to-one propensity score matching according to the variables of age, FIGO stage, histology, tumor size, stromal invasion depth, and postoperative radiochemotherapy in all patients. Meanwhile, the one-to-one propensity score matching was also performed in the two subgroups of patients with a tumor size ≥2 cm and <2 cm after confirming the interaction effect between surgical approach and tumor size through the multivariate Cox regression model. However, we must point out that there were not enough patients for the power analysis in the subgroup of patients with tumor size <2 cm. Tests were two-sided with p<0.05 deemed statistically significant.
Results
Characteristics and Survival Outcomes of all Patients
A total of 1065 patients met the criteria and were included in this study, of which 634 patients underwent abdominal radical hysterectomy and 431 patients underwent laparoscopic radical hysterectomy. The selection of the study population is presented in Figure 1. Surgeries through the two approaches in all participating hospitals were done concurrently during 2013–2016. During a median follow-up period of 60 months (range 3–82), the abdominal radical hysterectomy group experienced a recurrence rate of 10.1% and a death rate of 8.8%, and the laparoscopic radical hysterectomy group experienced a recurrence rate of 9.5% and a death rate of 6.7%. After evaluating the associations between surgical approach and clinicopathologic characteristics, significant differences were found between the two groups in FIGO stage, tumor size, and stromal invasion depth (p<0.01, p=0.07, p<0.01, respectively), as presented in Table 1. No significant differences were found between the two groups in disease-free survival and overall survival (online supplementary file S1) before matching.
Supplemental material
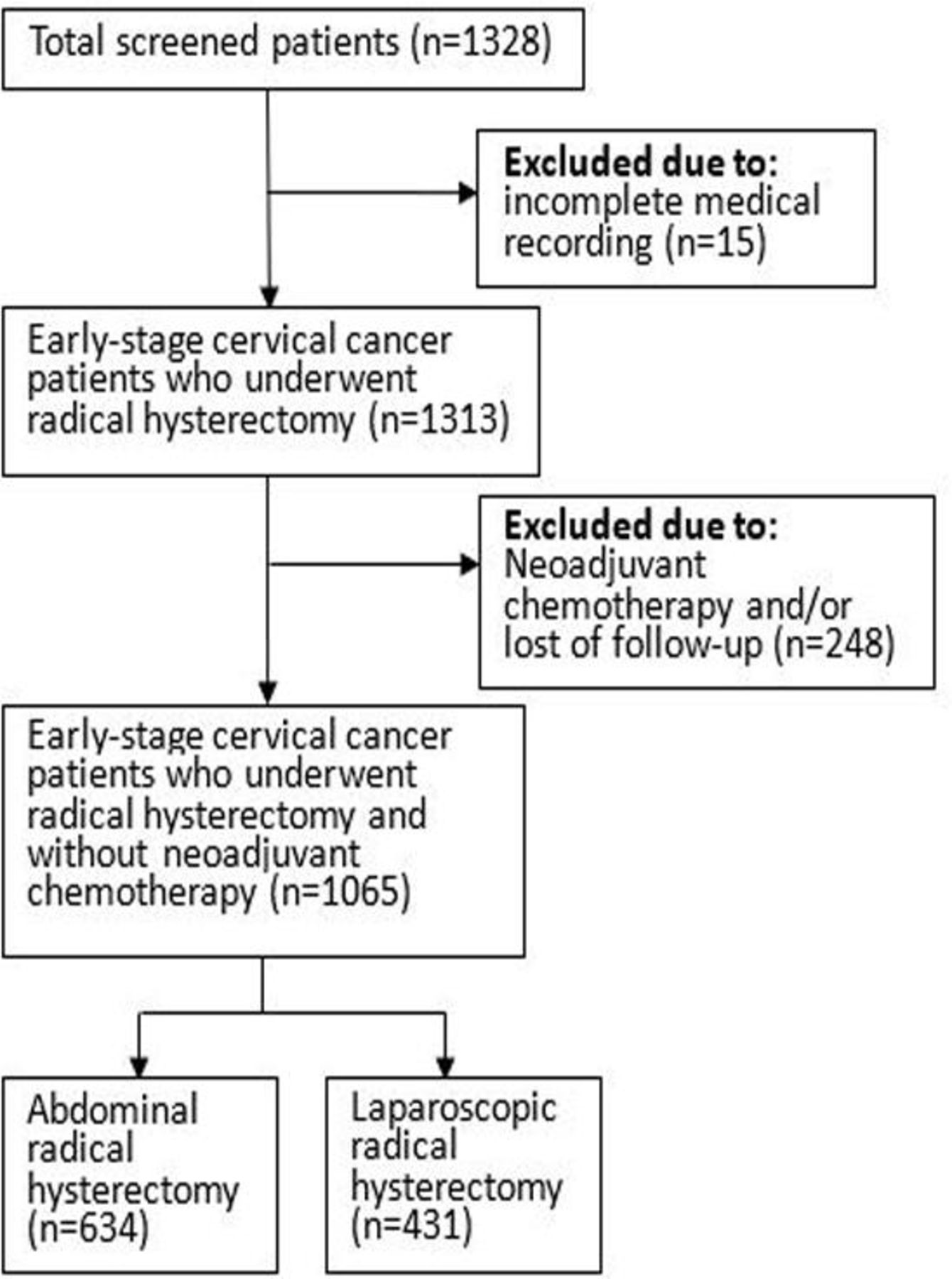
Flow diagram depicting the selection of the study population.
Characteristics of all patients
After 1:1 propensity score matching (online supplementary file S2), 812 patients were analyzed for survival outcomes, and there were no significant differences found in all characteristics between the two groups (Table 1). The survival analysis showed that patients treated with laparoscopic radical hysterectomy had a significantly shorter disease-free survival than patients treated with abdominal radical hysterectomy (5 year rate, 91.2% vs 94.1%; HR 1.65, 95% CI 1.00 to 2.73; p=0.048) (Figure 2A). However, there were no significant differences in overall survival (5 year rate, 95.7% in abdominal group and 93.8% in laparoscopic group; HR 1.60, 95% CI 0.89 to 2.88; p=0.12) (Figure 2B) between the two groups.
Supplemental material

{kind=link}
{kind=link}
Kaplan-Meier analysis of disease-free survival and overall survival for all patients (A,B), patients with tumor ≥2 cm (C,D), and patients with tumor <2 cm (E,F) after matching.
Characteristics and Survival Outcomes of Patients with Tumor Size ≥2 cm
After adjusting for age, FIGO stage, histology, stromal invasion depth, and postoperative radiochemotherapy, the interaction analysis showed a significant interaction effect between surgical approach and tumor size on disease-free survival (HR 1.27, 95% CI 1.05 to 1.53; p=0.014) (online supplementary file S3). Then we divided the patients into two subgroups according to tumor size. There were 673 patients with tumor size ≥2 cm (abdominal radical hysterectomy 422, laparoscopic radical hysterectomy 251). The abdominal radical hysterectomy group experienced a recurrence rate of 12.3% and a death rate of 11.4%; the laparoscopic radical hysterectomy group experienced a recurrence rate of 13.1% and a death rate of 10.0%. After evaluating the associations between the surgical approach and clinicopathologic characteristics, a significant difference was found in FIGO stage (p<0.01), as presented in Table 2. No significant differences were found between the two groups in disease-free survival and overall survival (online supplementary file S1) before matching. There were 436 patients (abdominal radical hysterectomy 218, laparoscopic radical hysterectomy 218) included in the survival analysis after 1:1 propensity score matching (online supplementary file S2). No significant differences were found in all characteristics between the two groups (Table 2). The results of survival analysis showed that patients who underwent laparoscopic radical hysterectomy had a significantly shorter disease-free survival than patients who underwent abdominal radical hysterectomy (5 year rate, 87.4% vs 93.5%; HR 1.93, 95% CI 1.05 to 3.55; p=0.032) (Figure 2C). However, no significant difference was found between the two groups in overall survival (5 year rate, 92.9% in abdominal group and 90.3% in laparoscopic group; HR 1.90, 95% CI 0.95 to 3.83; p=0.10) (Figure 2D).
Supplemental material
Characteristics of patients with tumor size ≥2 cm
Characteristics and Survival Outcomes of Patients with Tumor Size <2 cm
There were 392 patients with tumor size <2 cm, of which 212 patients underwent abdominal radical hysterectomy and 180 patients underwent laparoscopic radical hysterectomy. The abdominal radical hysterectomy group experienced a recurrence rate of 5.7% and a death rate of 3.8%; the laparoscopic radical hysterectomy group experienced a recurrence rate of 4.4% and a death rate of 2.2%. Significant differences were found between the two groups in FIGO stage (p=0.03) and stromal invasion depth (p=0.01) after evaluating the associations between surgical approach and clinicopathologic characteristics, as presented in Table 3. There were no significant differences between the two groups in disease-free survival and overall survival (online supplementary file S1) before matching.
Characteristics of patients with tumor size <2 cm
After 1:1 propensity score matching (online supplementary file S2), 294 patients were included in the survival analysis (abdominal radical hysterectomy 147, laparoscopic radical hysterectomy 147). There were no significant differences found in all characteristics between the two groups (Table 3). The results of survival analysis showed that there were no significant differences in disease-free survival (5 year rate, 94.3% in abdominal group and 97.3% in laparoscopic group; HR 0.71, 95% CI 0.24 to 2.16; p=0.59) (Figure 2E) and overall survival (5 year rate, 97.6% in abdominal group and 99.3% in laparoscopic group; HR 0.59, 95% CI 0.11 to 3.13; p=0.53) (Figure 2F) between the abdominal radical hysterectomy and laparoscopic radical hysterectomy groups.
Discussion
In this multicenter matching study, patients with early-stage cervical cancer who underwent laparoscopic radical hysterectomy experienced significantly shorter disease-free survival but not overall survival than patients who underwent open abdominal radical hysterectomy. In the patients with tumor size ≥2 cm, the laparoscopic radical hysterectomy group was also associated with significantly shorter disease-free survival but not overall survival than open abdominal radical hysterectomy. In addition, in patients with tumor size <2 cm, the two groups showed similar disease-free survival and overall survival. However, the sample size in the subgroup of patients with tumor size <2 cm was not enough for power analysis. These results implied that for the surgical treatment of patients with early-stage cervical cancer, priority should be given to the open abdominal radical hysterectomy.
In the last two decades, accumulating evidence suggested that patients who underwent minimally invasive surgery experienced comparable outcomes to open abdominal procedures, no matter whether they had benign or malignant disease.22–25 However, before the LACC trial, there were no randomized trials investigating the safety and efficacy of minimally invasive surgery in cervical cancer. Several retrospective studies involving patients with early-stage cervical cancer have revealed that minimally invasive surgery is superior to open abdominal surgery, with less blood loss, shorter hospital stay, and lower postoperative morbidity.26 27 But for the long-term survival outcomes, retrospective studies have yielded controversial results between the two surgical approaches. A meta-analysis involving 1539 patients revealed that there were no significant differences in 5 year overall survival (HR 0.91, 95 % CI 0.48 to 1.71; p=0.76) and 5 year disease-free survival (HR 0.97, 95 % CI 0.56 to 1.68; p=0.91) between the laparoscopic radical hysterectomy and abdominal radical hysterectomy groups in patients with cervical cancer.27 Nevertheless, in our previous single-center study, we found that the overall survival of laparoscopic radical hysterectomy was significantly shorter than that of abdominal radical hysterectomy in patients with locally advanced cervical cancer (HR 3.36, 95% CI 1.16 to 9.68; p=0.017).28 The LACC trial is a phase III, prospective, randomized controlled study comparing minimally invasive versus open abdominal radical hysterectomy in cervical cancer patients, and includes a large number of centers around the world.6 Because it is an important task to judge the superiority and inferiority of different surgical approaches for cervical cancer, further evidence is needed in order to weigh the pros and cons. We intended to provide further insight into the surgical treatment of patients with early-stage cervical cancer.
The results of our study showed that in the entire cohort and in patients with tumor size ≥2 cm, the laparoscopic radical hysterectomy group had a shorter disease-free survival than the open abdominal radical hysterectomy group. The reason why minimally invasive surgery is correlated with poorer prognosis in cervical cancer patients has been discussed in previous studies.6 10–23 For instance, the use of an intrauterine manipulator, the type of intra-abdominal colpotomy and the flow of gas into the abdominal cavity, as well as the non-standardized learning curves among surgeons, might lead to the inferior survival outcomes of minimally invasive surgery.29–31 In addition, no significant difference was found in overall survival between the laparoscopic radical hysterectomy and abdominal radical hysterectomy groups in our study, and the discrepancy between disease-free survival and overall survival may be due to the early detection of recurrences, adequate salvage therapy, and lost to follow-up bias. In patients with tumor size <2 cm, we found that the laparoscopic radical hysterectomy and abdominal radical hysterectomy groups had similar disease-free survival and overall survival. But it should be acknowledged that the sample size in this subgroup was not enough for power analysis. There are some reasons, except type II error, that may explain the similar disease-free survival and overall survival in patients with tumor size <2 cm. It should be noted that the impact of the intrauterine manipulator on the tumor may cause the tumor cells to spread. In the past, some laparoscopic operations did not seal the vagina before vaginal excision, which may also cause tumor cells to spread. However, small tumors may be less affected by these factors than large tumors; this may explain the similar survival outcomes between the laparoscopic radical hysterectomy and abdominal radical hysterectomy groups in patients with small tumors.
The strengths of our study include the fact that we enlarged the sample size based on our previous single-center study by including patients of an additional six hospitals and performed 1:1 propensity score matching to adjust for the confounders. Moreover, the 2018 FIGO stage for cervical cancer divided the stage IB into IB1, IB2, and IB3, adding the tumor size cut-off of 2 cm.32 However, the LACC trial was not powered to evaluate whether tumor size could have affected the oncologic outcome.6 In our study, we conducted the subgroup analysis according to the tumor size (<2 cm vs ≥2 cm) and the survival outcomes were compared between the laparoscopic radical hysterectomy and abdominal radical hysterectomy in the two subgroups after 1:1 propensity score matching.
Nevertheless, our study also has some disadvantages. First, given the retrospective nature of the study, non-random assignment of patients to groups resulted in selection bias. Second, involvement of the surgical margin was not routinely evaluated in each patient, thus we excluded this variable. Third, the sample size was relatively small in the subgroup of patients with tumor size <2 cm, which resulted in deficient power to determine the difference. The results of power analysis showed the power equal to 0.4 when we take the α value to 0.2. However, it is the largest sample size we can collect at present; future research attempting to prospectively analyze enough patients with tumor size <2 cm would be interesting. Lastly, because the laparoscopic radical hysterectomy became gradually popular in southwest China by 2010, we included patients between 2013–2016 to ensure that surgeons in each hospital had good surgical experience of performing laparoscopic radical hysterectomy; thus the follow-up time of this study was relatively short.
In conclusion, our retrospective multicenter study demonstrated that laparoscopic radical hysterectomy had a shorter disease-free survival but not overall survival than abdominal radical hysterectomy in patients with early-stage cervical cancer; therefore, priority should be given to open abdominal radical hysterectomy when conducting surgical treatment.
Acknowledgments
We thank all participating hospitals, namely Affiliated Hospital of Southwest Medical University, Affiliated Hospital of Zunyi Medical University, Affiliated Hospital of North Sichuan Medical College, People’s Hospital of Deyang City, Panzhihua Municipal Central Hospital and The First People’s Hospital of Neijiang City, as well as all patients.
References
Footnotes
Twitter @no
Contributorship statement Study conception and design: ZyL, TwyH. Data interpretation: NL, DN. Data collection and analysis: TwyH, YH. Manuscript writing and revising: TwyH, ZyL. Manuscript review: all authors.
Funding This study was supported by grants from the Sichuan Youth Foundation of Science of Technology (Grant number: 2015JQ0026).
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. The analyzed data sets generated during the study are available from the corresponding author on reasonable requests.