Article Text

Abstract
Objective The aim of this study was to evaluate if varying levels of compliance with an enhanced recovery after surgery (ERAS) protocol impacted post-operative outcomes (length of stay, complications, readmissions, and re-operations) in gynecologic surgery at a tertiary center.
Methods We included 584 patients who had open gynecologic surgery between November 1, 2014 and December 31, 2016. Patients were categorized into subgroups according to their date of surgery from the time of the ERAS protocol implementation. Patients were categorized by their per cent compliance into two groups:<80% versus ≥80%. We analyzed compliance with the elements of the protocol over time and its relation with post-operative outcomes, length of stay, post-operative complications, readmission, and re-operations rates. We modeled the probability of having a post-operative complication within 30 days of surgery as a function of overall compliance.
Results Overall compliance was 72.3%. Patients with compliance ≥80% had significantly less complications (P<0.001) and shorter length of stay (P<0.001). Readmission and re-operation rates were not impacted by compliance (P=0.182, P=0.078, respectively). Avoidance of salt water overload, early mobilization, early oral nutrition, and early removal of Foley catheter were significantly associated with less post-operative complications within 30 days.
Conclusions Compliance with an ERAS pathway exceeding 80% was associated with lower complication rates and shorter length of stay without impacting on re-operations or readmissions.
- ERAS
- compliance
- gynecologic surgery
- postoperative outcomes
Statistics from Altmetric.com
HIGHLIGHTS
This investigation was performed to further characterize the impact of compliance with ERAS elements on postoperative outcomes in patients undergoing open gynecologic surgery.
This study also characterizes how all the ERAS elements were implemented over time.
Compliance levels exceeding 80% were associated with significantly less complications (p<0.001) and shorter length of stay (p<0.001). Reoperation and readmission rates were not impacted by compliance.
Introduction
Implementation of an enhanced recovery after surgery (ERAS) program in gynecologic surgery has been associated with a reduction in length of stay, decreased opioid intake after surgery, and an improvement in patient reported outcomes associated with functional recovery.1 Benefits from ERAS programs across different surgical specialties have been demonstrated2 3 for post-operative outcomes and also for healthcare systems by decreasing costs and adding value to patient care.4 5
ERAS pathways are a multimodal and multidisciplinary approach applied across many teams. Individual ERAS components are implemented at different phases during the patient’s journey through the pre-operative, intra-operative, and post-operative phases of care. These combined factors may adversely impact compliance, both by the healthcare team and patient. Moreover, implementation of an ERAS pathway is associated with a major shift in clinical routines, from old practices to new standardized patient care pathways.
There is evidence from previous studies in colorectal,6 gastric,7 and orthopedic surgery8 showing that compliance with ERAS pathways is associated with improved clinical outcomes. There is a knowledge gap regarding whether or not the degree of adherence and compliance of each element directly or indirectly impacts on patient outcomes. The aim of this study was to evaluate compliance for each element of an ERAS protocol for patients undergoing open gynecologic surgery at a tertiary center and to determine if the time of implementation of the protocol impacted post-operative outcomes.
Materials and Methods
Study Design
The ERAS program for gynecologic surgery at our institution was implemented in November 2014 as a quality improvement practice change. Patients who underwent elective open gynecologic surgery in the Department of Gynecologic Oncology and Reproductive Medicine at the University of Texas MD Anderson Cancer Center and were treated according to the standardized ERAS program between November 1, 2014 and December 31, 2016 were included in this analysis. The indication for surgery was benign or malignant disease. Patients were excluded if they underwent emergency surgery or a pelvic exenteration, or if gynecologic surgery was not the primary surgery. During the pre-operative, intra-operative, and post-operative periods, 20 ERAS elements to measure compliance were established based on the practice guidelines for gynecologic surgery by the ERAS society.9–11 The institutional review board at the University of Texas MD Anderson Cancer Center approved the protocol (PA16-0939).
To explore if compliance with ERAS elements changed over time, we defined three time periods according to the patient’s date of surgery from the time of ERAS implementation: period 1 (P1)−November 1, 2014 to July 31, 2015; period 2 (P2) August 1, 2015 to March 3, 2016; and period 3 (P3) March 4, 2016 to December 21, 2016. The time periods were selected to have approximately the same number of cases. Over the course of this study, the surgical staff, anesthesiologists, and nursing staff remained largely unchanged. In addition, during this time, there were no major changes to the guidelines of the ERAS pathway at our institution nor was there implementation of new initiatives that could have impacted on the results of this study.
Data Collection
Data were collected retrospectively and managed using a REDCap (Research Electronic Data Capture) database hosted at the University of Texas MD Anderson Cancer Center as part of the quality improvement study (QI-6033).12 Data including demographic and clinical characteristics, surgical procedure, intra- and post-operative (up to 30 days) complications, length of stay, readmissions, re-operations, and post-operative management (including pain medications, fluids, diet, and mobilization) were collected. The Clavien–Dindo grading system was used to characterize post-operative complications.13 Complications within 30 days after surgery were classified as gastrointestinal, genitourinary, central nervous system, cardiovascular, hematologic, and wound related complications. Complications were also identified as mild (grades 1–2) or severe (grades 3–4). For patients with multiple complications of the same type, the final result was characterized according to their highest grade of post-operative complication. The current malignancy was not included in the calculation of the Charlson Comorbidity Index to more accurately reflect pre-cancer comorbid conditions.
Statistical Analysis
Descriptive statistics were used to summarize the demographic and clinical characteristics of patients. For each patient, per cent compliance was calculated as the number of interventions fulfilled divided by 20 (total number of ERAS elements). Overall mean compliance was estimated with 95% confidence intervals. Patients were categorized by their per cent compliance (<80% compared with ≥80%). We used the same cut-off values as previously reported by Wong-Lun-Hing et al14 where compliance was classified as 'full', 'partial', or 'poor' when ≥80%, ≥50%, or <50%, respectively, of the 20 ERAS elements were met. In our cohort, very few patients had a compliance rate of <50% so the partial and poor groups were grouped together as 'partial'. Associations with peri-operative outcomes were compared among levels of compliance using Fisher’s exact test for categorical variables and the Wilcoxon rank sum test for continuous variables.
Independent of the previous analysis, patients were categorized according to their surgery date from the time of ERAS implementation. Patient demographics and clinical characteristics were compared using Fisher’s exact test for categorical variables and the Mann–Whitney U test for continuous variables. Within each period, the proportion of patients compliant with each ERAS component was tabulated and compared using a Fisher’s exact test.
Patients were classified as having any (one or more) post-operative complication within 30 days or no complications. Logistic regression models were used to model the probability of a post-operative complication within 30 days as a function of per cent compliance. Separate univariate logistic regression models were used to model the probability of post-operative complications as a function of each ERAS component. Similarly, separate logistic regression models were used to model the probability of readmission and re-operation as a function of per cent compliance.
Assuming a standard deviation in the per cent compliance of 25% (taking the range of 0–100% divided by 4), with 584 patients, we were able to estimate mean compliance with 2.0% precision. P values <0.05 were considered statistically significant. No adjustments were made for multiple comparisons. All statistical analyses were performed using SAS 9.4 for Windows (SAS Institute Inc, Cary, North Carolina, USA).
Results
A total of 584 patients underwent elective open gynecological surgery (P1=194 patients, P2=191 patients, and P3=199 patients). Subgroups were comparable in terms of age, pre-operative hemoglobin and albumin, BMI, Charlson Comorbidity Index, and ethnicity (Table 1). A larger proportion of patients with ASA scores III–IV was observed in the third period compared with the other periods (P=0.046). The distribution of races varied among the periods. On the third period, there was a lower proportion of African Americans and a marginally larger percentage of patients reported 'other' race (P=0.043). There were no differences in neoadjuvant treatment, indication for surgery, and primary disease site. Even though period 2 had a significantly higher proportion of patients with previous abdominal surgery (P=0.038) and lower operative time (P=0.003), there were no differences in the surgical complexity, estimated blood loss, or administration of intra-operative blood products among periods (P=0.147, P=0.074, and P=0.137, for periods 1, 2 and 3, respectively) (Table 1).
Patient demographics and clinical characteristics*
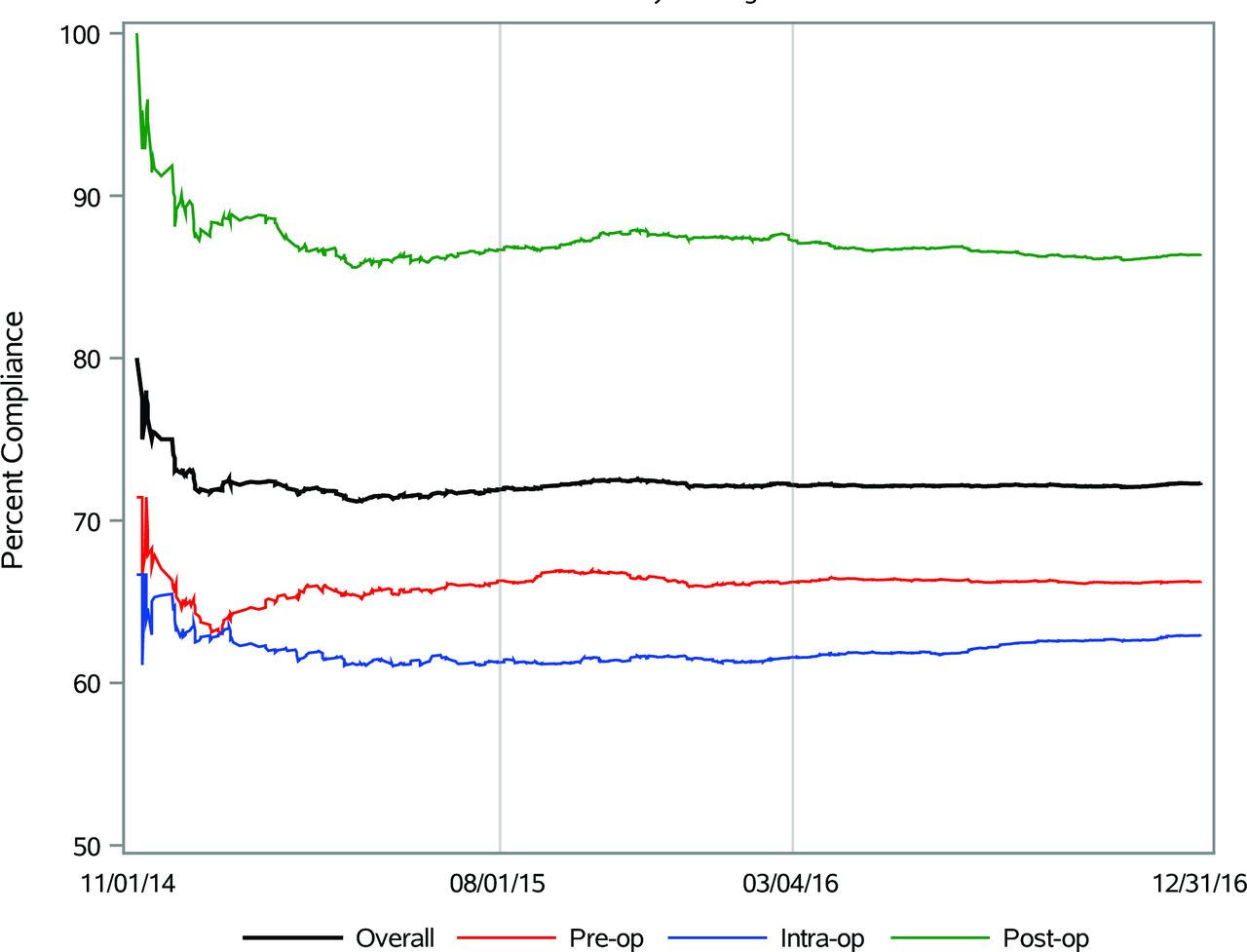
Compliance with the ERAS pathway over time is illustrated in Figure 1. The overall average compliance was 72.3% (95% CI 71.7% to 72.9%). There was an initial peak and drop, although 5 months after implementation (which corresponds to 80 patients) the lines flattened and compliance with the ERAS pathway remained stable for all peri-operative parameters. The intra-operative component had the least variation over time and also the lowest compliance at any time, while the post-operative phase had the highest compliance at any given time.

{kind=link}
Cumulative compliance with the enhanced recovery after surgery (ERAS) pathway in subsequent patients.
In the pre-operative phase, there were three elements whose overall compliance did not reach 50%. These elements were pre-operative counseling (42.1%), optimization (1.2%), and use of pre-operative midazolam (26.7%) (Table 2). Pre-operative optimization (defined as alcohol and smoking cessation, and glucose and anemia control) was the element with the lowest overall compliance (1.2%) among all the 20 ERAS elements that were implemented (excluding the minimally invasive surgery approach). Compliance with pre-operative counseling appeared to improve over time (P1=37.1%, P2=43.5%, and P3=45.7%) (Table 2) although the difference between periods was not statistically significant. Administration of pre-operative heparin decreased significantly during the second period and administration of midazolam increased over time (online supplementary figure 1). The use of short acting anesthetics increased significantly over time and the use of goal directed fluid therapy decreased (Table 2 and online supplementary figure 1). The highest overall compliance was noted in the post-operative period where there were 6 of 8 elements whose compliance was greater than 85%. We also analyzed if post-operative outcomes (length of stay, complications, readmissions, and re-operations) were different across the study periods. No differences were found (online supplementary Table 1).
Supplemental material
Supplemental material
Compliance with individual enhanced recovery after surgery (ERAS) protocol elements
The effect of compliance was also analyzed comparing patients with an overall compliance of >80% (n=134) with patients with compliance of <80% (n=450) (Table 3). Length of stay was significantly shorter in patients with >80% compliance (2 days versus 3 days; P<0.001). Patients with >80% compliance had significantly less complications (P<0.001). When considering complications by grade, mild to moderate complications (Clavien–Dindo grades I–IIIa) were less frequent in patients with higher compliance (P=0.004, P<0.001, and P=0.039, respectively) (Table 3) but there were no differences for severe complications (Clavien–Dindo grades IIIb–V) . Readmissions and re-operations were not impacted by level of compliance (<80% versus ≥80%) (P=0.143 and P=0.078, respectively). Patients in both groups (compliance <80% versus ≥80%) were comparable in demographics and clinical characteristics (online supplementary Table 2). Patients who were <80% compliant were younger than those with ≥80% compliance (P=0.022). Estimated blood loss and surgery time were higher in patients with <80% compliance; 300 mL versus 200 mL (P<0.001) and 226 min versus 195 min (P<0.001), respectively. There were no differences between the compliance (<80% versus ≥80%) groups for indication for surgery, surgical complexity, or administration of intra-operative blood products (online supplementary Table 2). We also analyzed the probability of having a post-operative complication (within 30 days of surgery) with ERAS element compliance. There was a statistically significant association between lower post-operative complications within 30 days and avoidance of salt–water overload, implementation of early mobilization, early oral nutrition, and early removal of Foley (Table 4).
Supplemental material
Peri-operative outcomes and compliance*
Association of having a post-operative complication within 30 day and compliance with each enhanced recovery after surgery (ERAS) component
Discussion
Our study showed that overall compliance rate for our ERAS program in gynecologic surgery was 72.3%. Recently, Bisch et al15 reported a mean compliance rate of 77% after implementation of an ERAS program in gynecologic oncology. In addition, we showed that compliance exceeding 80% is associated with lower complication rates and shorter length of stay without impacting on re-operations or readmissions. Similarly, Bergstrom et al16 noted a significant improvement in length of stay in patients with compliance rate ≥80%. A recent international multicenter observational study of more than 2000 patients undergoing planned gynecological surgery found an association between increased compliance with ERAS guidelines and shorter length of stay, regardless of the magnitude of the surgery.17 In addition, the same study also reported that the risk of having a complication was lower with greater compliance with ERAS guidelines.
In the setting of colorectal surgery, Gustafsson et al18 previously reported that adverse post-operative outcomes (30 day morbidity, symptoms and readmissions) were significantly reduced with increasing compliance. Similarly, another study in liver surgery6 showed an inverse correlation between compliance and length of stay.
Maintenance of compliance on an ERAS program is crucial to optimize patient outcomes. This requires constant auditing and analysis of the results to correct potential deviations from the pathway. It is necessary to ensure that all or most elements of peri-operative guidelines for ERAS are enforced. Pre-operative counseling is a major component of the success of an ERAS program. In our department, at the initiation of the program, we noted that pre-operative counseling was often poorly documented although being performed. Thus we were proactive in ensuring our staff were properly trained to not only offer the counseling but to also take the appropriate steps to document such counseling. One component of low compliance in our group was pre-operative optimization that encompasses alcohol and smoking cessation. On our service, we usually see patients within 1–2 weeks from surgery; hence time for implementation of these items is limited in our setting. In order to address this barrier, we have initiated a pre-habilitation program for patients with advanced ovarian cancer who are undergoing neoadjuvant chemotherapy where such optimization is implemented.
The intra-operative goals of the pathway at our institution emphasize multimodal analgesia, the use of short acting anesthetics, opioid sparing techniques, and goal directed fluid therapy. In our study, we noted that when evaluating intra-operative compliance there was an increase in the use of short-acting anesthetics over time. This increase in short-acting anesthetic use was mostly attributed to a greater emphasis by our anesthesia team to re-educate staff on the benefits of opioid sparing techniques and subsequent post-operative benefits of such an approach. We noted that the use of goal directed fluid therapy in our study decreased over time. Goal directed fluid therapy remains a topic of significant controversy in the field of anesthesia and more importantly in the context of ERAS programs.19–23 In our institution, there has been an overall decrease in the use of advanced hemodynamic monitoring, limiting the use of goal directed fluid therapy to patients undergoing major debulking surgery with potential for blood loss or for patients with multiple comorbidities in which the anesthesiology provider deems monitoring necessary. A recent study showed that similar outcome benefits can be obtained by rigorous attention to avoiding fluid overload and maintaining 'zero balance' compared with the use of Doppler monitoring.24
Previous data showed that adoption of post-operative guidelines as part of standard practice seems more challenging compared with pre- and intra-operative guidelines.25 It has been proposed that this may be due to the fact that this requires participation of a larger group of providers, such as nursing and mid-level providers.25 26 A dedicated educational and training program may provide opportunities for overcoming this barrier and, as such, in our department we instituted a series of education opportunities for all post-operative nurses to gain access to didactic teaching as well as written evidenced based data on the benefits of ERAS pathways. Additionally, standardized post-operative order sets were utilized. We attribute the high compliance in the post-operative setting in our study to such interventions.
Several steps are recommended in improving compliance when implementing an ERAS program. Firstly, thorough and frequent auditing is necessary to determine if items in the guidelines are being completed and measured appropriately. Secondly, strict definitions should be used when measuring compliance so that all involved are categorizing using the same data dictionary. Thirdly, implementation of order sets allows for consistent delivery of care as it is easier to maintain compliance when there is standardization for ordering medications such as antibiotics and pre-operative heparin.
The strengths of our study include the fact that we implemented our ERAS program in the Department of Gynecologic Oncology and Reproductive Medicine in November 2014 as a quality improvement initiative. All surgeons in the department agreed to aim for high levels of compliance with all components of the guidelines. In addition, all laparotomies were included in the ERAS program and implementation was not dependent on type of surgery or level of complexity. Also, we collected data for all patients who had undergone surgery since the date of implementation of the ERAS program. This database undergoes continuous auditing for data completeness and accuracy. Also, our study included the largest single site cohort of patients undergoing open gynecologic surgery under an ERAS pathway.
Our study also has a number of limitations. Even though one of the elements described in the ERAS guidelines is minimally invasive surgery, we first implemented the ERAS program at our institution in patients undergoing open surgeries exclusively; later we implemented the pathway on patients undergoing minimally invasive surgery. All patients included in this study underwent open gynecologic surgery and we knew upfront that the highest compliance level for a given patient would be 95%. Secondly, we have not determined whether compliance drives the resulting outcomes or if patients who suffer a complication ultimately deviate from many elements of the ERAS program and thus will be considered ‘non-compliant’. Limited observations of non-compliant patients with complications led to our inability to perform multivariate modeling to better understand associations between compliance and post-operative outcomes. Future steps are to identify which gynecologic open surgeries would benefit most from an ERAS program as well as which patient characteristics are associated with higher compliance rates.
Conclusion
In summary, compliance rates exceeding 80% should be the aim of ERAS programs as this is associated with more favorable peri-operative outcomes. Although a strict number of ERAS guideline items have not directly been associated with improved outcomes, the aim should be to achieve high levels of compliance with most items in the guidelines. Our study also showed that avoidance of salt–water overload, early mobilization, early oral nutrition, and early removal of Foley catheter are associated with fewer post-operative complications.
References
Footnotes
Contributors All authors have directly participated in the planning, execution, or analysis of our study and have read and approved the final version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The institutional review board at the University of Texas MD Anderson Cancer Center approved the protocol (PA16-0939).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.