Article Text

Abstract
Objectives To compare clinicopathologic characteristics and prognosis for different histologic subtypes in early cervical cancer.
Methods Patients who underwent radical surgery for stage IA2–IIA2 cervical cancer with squamous cell carcinoma, adenocarcinoma, or adenosquamous carcinoma between March 2006 and February 2014 at our institution were retrospectively evaluated. The two-sample t-test was used to compare the mean values of continuous variables. The Chi-square test was used to assess differences in the distribution of categorical variables. Survival curves were generated by the Kaplan-Meier method using log-rank test. Univariable and multivariable analyses were performed using Cox regression analysis.
Results Of 5181 patients evaluated, 4510 had squamous cell carcinoma, 488 had adenocarcinoma, and 183 had adenosquamous carcinoma. Compared with squamous cell carcinoma, adenocarcinoma was associated with earlier stage, smaller tumor size, less lymphovascular space invasion (26.7% vs 37.9%), less deep (>2/3 depth) stromal invasion (30.4% vs 36.2%), and more ovarian metastasis (4.2% vs 0.7%) (all p<0.001). Compared with adenosquamous carcinoma, adenocarcinoma was associated with earlier stage (p=0.011), smaller tumor size (p<0.001), less lymphovascular space invasion (26.7% vs 41.5%, p<0.001), and less peripheral nerve infiltration (5.7% vs 15.4%, p<0.001). Except for more peripheral nerve infiltration in adenosquamous carcinoma (15.4% vs 8.4%, p=0.002), no significant differences in other clinicopathologic characteristics were noted between squamous cell carcinoma and adenosquamous carcinoma. Five-year recurrence-free survival was 85.1%, 78.2%, and 72.3% for squamous cell carcinoma, adenocarcinoma, and adenosquamous carcinoma, respectively (p<0.001). Corresponding 5-year overall survival was 89.7%, 83.1%, and 79.6%, respectively (p<0.001). In multivariable analysis, adenocarcinoma and adenosquamous carcinoma were independent prognostic factors for worse recurrence-free survival for adenocarcinoma versus squamous cell carcinoma (HR 2.594 (95% CI 2.030 to 3.316), p<0.001) and for adenosquamous carcinoma versus squamous cell carcinoma (HR 2.105 (95% CI 1.517 to 2.920), p<0.001), and overall survival for adenocarcinoma versus squamous cell carcinoma (HR 2.976 (95% CI 2.226 to 3.977), p<0.001) and for adenosquamous carcinoma versus squamous cell carcinoma (HR 2.295 (95% CI 1.579 to 3.338), p<0.001).
Conclusion Squamous cell carcinoma, adenocarcinoma, and adenosquamous carcinoma carried distinctive patterns of clinicopathologic characteristics. Adenocarcinoma and adenosquamous carcinoma had worse survival outcomes than squamous cell carcinoma.
- adenocarcinoma
Statistics from Altmetric.com
Highlights
Compared with adenosquamous carcinoma, adenocarcinoma was associated with earlier stage, smaller tumor size, less lymph0vascular space invasion, and less peripheral nerve infiltration.
No significant differences were observed in parametrial invasion, lymph node metastasis, and vaginal margin involvement among the three groups.
Adenocarcinoma and adenosquamous carcinoma were independent prognostic factors of poorer recurrence-free survival and overall survival compared with squamous cell carcinoma.
Introduction
Although the incidence of, and mortality from, cervical cancer have declined in most developed countries, it remains one of the leading causes of cancer deaths in most developing countries, including China.1 2 Squamous cell carcinoma, adenocarcinoma, and adenosquamous carcinoma are the three most common histologic subtypes of uterine cervical cancer, accounting for about 95% of all histologic types.3 In contrast to squamous cell carcinoma, which has progressively decreased in incidence and mortality in recent decades, the incidence and mortality of adenocarcinoma has increased during the same period.4–8 In the same time period, the incidence of adenosquamous carcinoma decreased but the proportion increased.8
Several studies have reported that histologic type could independently influence survival outcomes. Patients with adenocarcinoma and adenosquamous carcinoma had a worse prognosis than squamous cell carcinoma patients, implying that adenocarcinoma/adenosquamous carcinoma was a potential risk factor for cervical cancer and patients with adenocarcinoma/adenosquamous carcinoma should be treated more aggressively.9–12 Nevertheless, other studies have drawn contradictory conclusions.13 14 In addition, adenocarcinoma and adenosquamous carcinoma are different from squamous cell carcinoma in their clinicopathologic characteristics, ovarian metastasis for instance.15 16 However, little is known about the specific biologic characteristics of adenosquamous carcinoma since few previous studies distinguished adenosquamous carcinoma from adenocarcinoma.
Given the rising incidence of adenocarcinoma and the limited knowledge about adenosquamous carcinoma, studies of the differences in histopathologic characteristics and survival outcomes for the different histologic subtypes of cervical cancer are of particular importance. The goal of our study was to investigate the clinicopathologic and survival differences based on squamous cell carcinoma, adenocarcinoma, and adenosquamous carcinoma histology in stage IA2–IIA2 cervical cancer after radical surgery.
Methods
Clinical Data
All consecutive International Federation of Gynecology and Obstetrics (FIGO) stage IA2–IIA2 cervical cancer patients who underwent (modified) radical hysterectomy/trachelectomy and pelvic lymph node dissection with or without para-aortic lymph node dissection from March 2006 to February 2014 at Fudan University Shanghai Cancer Center were retrospectively analyzed. Patients with metastatic or incidentally diagnosed cervical cancer and patients with additional malignancies were excluded. Furthermore, we excluded patients who were treated with neoadjuvant chemotherapy because of its potential impact on pathologic findings in surgical specimens. The histologic types were classified based on hematoxylin-eosin staining and supported by immunohistochemistry staining according to the WHO classification of tumors of the female reproductive organs. Only patients with squamous cell carcinoma, adenocarcinoma, and adenosquamous carcinoma were included in our study. Stages were assigned based on FIGO staging of cancer of cervix uteri (2009). Differences in clinicopathologic characteristics and survival outcomes were compared among the three groups. The study was approved by our institutional review board.
Adjuvant therapy was administered mainly based on pathologic findings. Patients with only one intermediate-risk factor including large tumor size (diameter ≥4 cm), more than 1/2 depth of cervical stromal invasion, and lymphovascular space invasion were administered chemotherapy or remained under observation at the physician’s discretion. Patients with two or more intermediate-risk factors and patients with one or more high-risk factors (positive pelvic lymph nodes, parametrial invasion, and positive vaginal resection margins) were administered adjuvant radiation therapy or concurrent chemoradiation therapy. In patients who received concurrent chemoradiation therapy, platinum-based regimens were used.
Recurrence and death were the two main events evaluated. Recurrence was assumed clinically when physical examination or imaging suggested recurrence, or pathologically. Recurrence-free survival was defined as the period from the time of surgery to the occurrence of relapse. Overall survival was defined as the period from the time of surgery to the time of death. Data for patients who had not had an event were censored.
Statistical Analysis
Two-sample t-test was used to compare the mean values of continuous variables. Chi-square test was used to assess differences in the distribution of categorical variables. Fisher's exact test was used if the expected frequency was <5. Survival curves were generated by the Kaplan-Meier method using the log-rank test. Univariable and multivariable analyses were performed using Cox regression analysis. All statistical analyses were performed using Statistical Product and Service Solutions (SPSS) software (version 23.0, SPSS, Chicago, IL, USA). A p value <0.05 was considered statistically significant.
Results
Patient characteristics are summarized in Table 1. A total of 5181 patients were evaluated in our study, and comprised 4510 (87.0%) patients with squamous cell carcinoma, 488 (9.4%) patients with adenocarcinoma, and 183 (3.5%) patients with adenosquamous carcinoma. Median age was 46 (IQR 40–53) years. FIGO stage distribution of all patients was: IA2 1.2%, IB1 47.9%, IB2 7.5%, IIA1 30.8%, and IIA2 12.6%. Of the 5181 patients, 4985 (96.2%) underwent radical hysterectomy, compared with 54 (1.0%) who underwent modified radical hysterectomy and 142 (2.7%) who underwent radical trachelectomy. Out of the total number of patients, 749 (14.5%) accepted para-aortic lymph node dissection and 3685 (71.1%) accepted oophorectomy.
Patient characteristics (n=5181)
Compared with squamous cell carcinoma, patients with adenocarcinoma were younger (45.35±10.890 years vs 46.83±10.067 years, p=0.002) and were more likely to present with earlier stage, smaller tumor size, less lymphovascular space invasion (26.7% vs 37.9%), less deep (>2/3 depth) stromal invasion (30.4% vs 36.2%), and more ovarian metastasis (4.2% vs 0.7%) (all p<0.001) (Table 2). When compared with adenosquamous carcinoma, adenocarcinoma was associated with earlier stage (p=0.011), smaller tumor size (p<0.001), less lymphovascular space invasion (26.7% vs 41.5%, p<0.001), and less peripheral nerve infiltration (5.7% vs 15.4%, p<0.001). Except for more peripheral nerve infiltration in adenosquamous carcinoma (15.4% vs 8.4%, p=0.002), no significant differences in other clinicopathologic characteristics were observed between squamous cell carcinoma and adenosquamous carcinoma. When comparing high-risk factors, no significant differences were observed in parametrial invasion, lymph node metastasis, and vaginal margin involvement among the three groups (all p>0.05).
Comparison of demographic and histopathologic characteristics in squamous cell carcinoma, adenocarcinoma and adenosquamous carcinoma groups
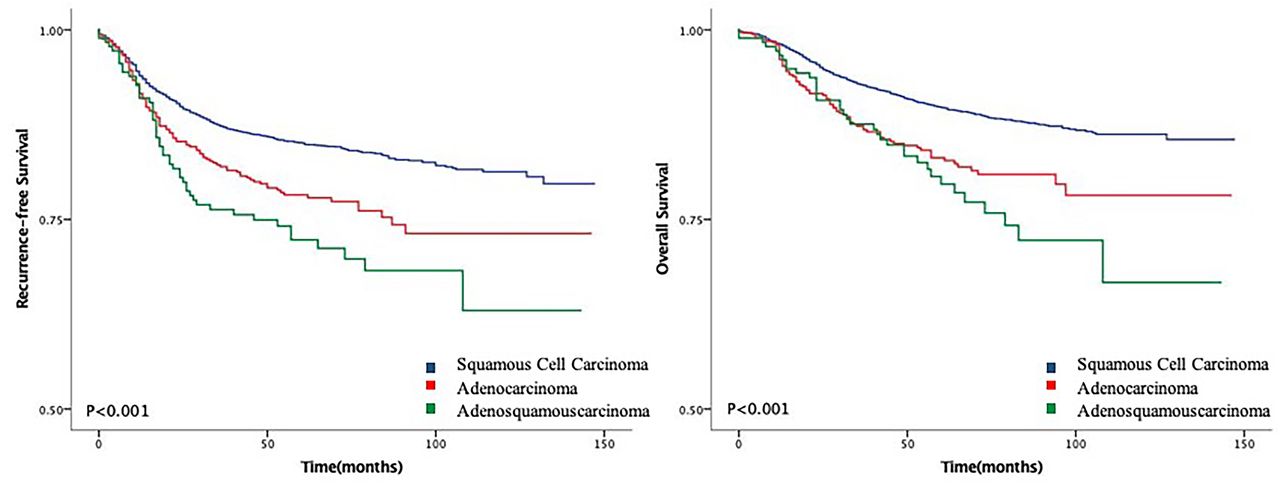
The median follow-up time was 59 (IQR 32–82) months. A total of 4622 (89.2%) patients were still alive at last follow-up, and 559 (10.8%) deaths were documented. In the Kaplan-Meier analysis, squamous cell carcinoma patients presented longer recurrence-free survival and better overall survival compared with adenocarcinoma (p recurrence-free survival <0.001, p overall survival <0.001, respectively) and adenosquamous carcinoma (p recurrence-free survival <0.001, p overall survival <0.001, respectively) patients (Figure 1). There was no significant difference between adenocarcinoma and adenosquamous carcinoma patients in both recurrence-free survival (p=0.106) and overall survival (p=0.245). Five-year recurrence-free survival rates of the three groups were 85.1% (95% CI 83.9% to 86.3%) for squamous cell carcinoma, 78.2% (95% CI 74.3% to 82.1%) for adenocarcinoma, and 72.3% (95% CI 65.4% to 79.2%) for adenosquamous carcinoma, respectively. Corresponding 5-year overall survival rates were 89.7% (95% CI 88.7% to 89.9%), 83.1% (95% CI 79.6% to 86.6%), and 79.6% (95% CI 72.9% to 86.3%), respectively.

{kind=link}
Kaplan-Meier curves of recurrence-free survival and overall survival based on histologic types. Blue line, squamous cell carcinoma; red line, adenocarcinoma; green line, adenosquamous carcinoma. Squamous cell carcinoma patients presented longer recurrence-free survival and better overall survival compared with adenocarcinoma (p recurrence-free survival <0.001, p overall survival <0.001, respectively) and adenosquamous carcinoma (p recurrence-free survival <0.001, p overall survival <0.001, respectively) patients. There was no significant difference between adenocarcinoma and adenosquamous carcinoma patients in both recurrence-free survival and overall survival (p recurrence-free survival =0.106, p overall survival =0.245, respectively).
After adjustment, adenocarcinoma and adenosquamous carcinoma were independent predictors of poorer recurrence-free survival for adenocarcinoma versus squamous cell carcinoma (HR 2.594 (95% CI 2.030 to 3.316), p<0.001) and for adenosquamous carcinoma versus squamous cell carcinoma (HR 2.105 (95% CI 1.517 to 2.920), p<0.001), and overall survival for adenocarcinoma versus squamous cell carcinoma (HR 2.976 (95% CI 2.226 to 3.977), p<0.001) and for adenosquamous carcinoma versus squamous cell carcinoma (HR 2.295 (95% CI 1.579 to 3.338), p<0.001) compared with squamous cell carcinoma (Tables 3 and 4). The known negative influence of a large tumor size, the presence of deep stromal invasion, lymphovascular space invasion, parametrial invasion, positive vaginal resection margin, and lymph node metastasis on recurrence-free survival and overall survival were also confirmed in our study by both univariate analysis and multivariate analysis. Conversely, concurrent chemoradiotherapy had a significant positive influence on recurrence-free survival (HR 0.540 (95% CI 0.411 to 0.709), p<0.001) and overall survival (HR 0.529 (95% CI 0.379 to 0.738], p<0.001) compared with no further treatment.
Univariable analysis of clinicopathologic characteristics on recurrence-free survival and overall survival
Multivariable analysis of clinicopathologic characteristics on recurrence-free survival and overall survival
Discussion
In this large, single institutional study we demonstrated that different histologic subtypes of cervical cancer had distinctive clinicopathologic characteristics and survival outcomes. Both adenocarcinoma and adenosquamous carcinoma were independent predictors of poorer recurrence-free survival and overall survival compared with squamous cell carcinoma.
Adenocarcinoma has been reported to be different from squamous cell carcinoma in clinicopathologic characteristics.17 In our study we observed that adenocarcinoma was associated with younger age of onset, earlier stage, smaller tumor size, less deep stromal invasion, and more ovarian metastasis compared with squamous cell carcinoma, as reported in previous studies.10 14 15 18 Moreover, our study also suggested that compared with squamous cell carcinoma, fewer patients with adenocarcinoma had lymphovascular space invasion. In addition, we reported the distinctive characteristics of adenosquamous carcinoma. Adenosquamous carcinoma histology had similar features to that of squamous cell carcinoma in regard to all clinicopathologic characteristics investigated in our study except for peripheral nerve infiltration, which was more frequently seen in adenosquamous carcinoma compared with squamous cell carcinoma. However, peripheral nerve infiltration was not an independent prognostic factor in our study. Whether it influenced survival independently remains controversial.19–22
The impact of histopathologic types of cervical cancer on prognosis remains controversial. Several previous studies reported that adenocarcinoma/adenosquamous carcinoma histology negatively impacted survival. Pure adenocarcinoma of the cervix was reported to entail a worse survival outcome than squamous cell carcinoma in patients with early cervical cancer.10 Both adenocarcinoma and adenosquamous carcinoma histology negatively impacted survival for stage IB1–IIA carcinoma in Galic’s study.18 However, some studies reached contradictory conclusions. Noh et al9 reported that adenocarcinoma histology was associated with poor survival outcomes in patients with FIGO stage IB–IIA cervical cancer but not adenosquamous carcinoma. The multi-institutional study of Winer et al14 compared early-stage cervical adenocarcinoma and squamous cell carcinoma and suggested equivalent recurrence and survival. In our study, adenocarcinoma was an independent predictor of worse recurrence-free survival and overall survival compared with squamous cell carcinoma, consistent with the studies of Lee et al10 and Noh et al.9 However, conflicting with Noh et al's study, which reported that prognosis of adenosquamous carcinoma histology was closer to that of squamous cell carcinoma histology than that of adenocarcinoma histology, we found that patients with adenosquamous carcinoma had worse survival outcomes than those with squamous cell carcinoma, and no significant difference was observed in survival outcomes between adenocarcinoma and adenosquamous carcinoma, although both the 5-year recurrence-free survival and overall survival of adenosquamous carcinoma were lower than those of adenocarcinoma. In consideration of the findings of worse survival outcomes of adenocarcinoma and adenosquamous carcinoma in this study and several previous studies, inclusion of histology as a risk factor in treatment may be indicated.
The molecular profiles of squamous cell carcinoma and adenocarcinoma were reported to be distinct.23 24 EGFR mutation was detected only in squamous cell carcinoma, and KARS mutation was detected only in adenocarcinoma.25 The mutation frequency of TP53 was significantly higher in adenocarcinoma compared with squamous cell carcinoma.26 The methylation pattern of the two histologic subtypes was also reported to be different.27 Besides, controversies still remained as regards differences between the immune profiles of squamous cell carcinoma and adenocarcinoma. An early study reported co-gain or co-amplification of PD-L1 and PD-L2 in 67% (32/48) squamous cell carcinoma and PD-L1 expression correlating with PD-L1 and PD-L2 co-amplification.28 In TCGA study, amplifications of PD-L1 and PD-L2 were detected in both squamous cell carcinoma and adenocarcinoma.29 Gadducci et al30 reported PD-L1 was more frequently positive in squamous cell carcinoma compared with adenocarcinoma. However, no significant differences in PD-L1 expression were noted in Enwere et al’s research.31 The different molecular and immunologic profiles observed for squamous cell carcinoma and adenocarcinoma could partially explain the distinctive clinicopathologic characteristics and prognosis of the two histologic subtypes, and more tailored treatment strategies are still awaited. Furthermore, due to the rarity of adenosquamous carcinoma, we have little knowledge of its molecular and immunologic profiles.
This study has several limitations. First, this study was a retrospective study with potential recall bias. However, it could be partially compensated by the large sample size and the long-term follow-up. In addition, since this study was a single institutional study and all the patients were Chinese women, the results may not be generalizable to other institutions or patients of other nationalities. However, a single institutional study also means that the patients accepted unified protocol of treatment and were more comparable.
In conclusion, we observed distinctive clinicopathologic characteristics in squamous cell carcinoma, adenocarcinoma, and adenosquamous carcinoma patients, and adenocarcinoma and adenosquamous carcinoma were associated with worse survival outcomes compared with squamous cell carcinoma in patients with early cervical cancer (FIGO stage IA2–IIA2) who underwent radical surgery. Different treatment strategies for adenocarcinoma and adenosquamous carcinoma of the cervix may be needed.
References
Footnotes
LC and HW are joint first authors.
Contributors All authors contributed to study design, data interpretation, and writing. Data analysis was primarily performed by LC.
Funding The authors gratefully acknowledge the contribution of the study investigator, Chunyan Song, without whom the study would not have been possible.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.