Article Text

Abstract
Pelvic and para-aortic lymphadenectomy is routinely performed in early ovarian cancer to define the stage of the disease. However, it may be associated with increased blood loss, operative time, and length of hospitalization. The sentinel lymph node technique has been shown to be safe and feasible in vulvar, uterine, and cervical cancer. Data detailing feasibility and outcomes of sentinel lymph node mapping in ovarian cancer are scarce.
To summarize the studies evaluating the feasibility of sentinel lymph node detection from the ovary, examining the technique and detection rate.
A systematic search of the literature was performed using PubMed and Embase from June 1991 to February 2019. Studies describing the sentinel lymph node technique and lymphatic drainage of the ovaries were incorporated in this review. Ten articles were selected, comprising a total of 145 patients. A variety of agents were used, but the primary markers were technetium-99m radiocolloid (Tc-99m), patent blue, or indocyanine green, and the most common injection site was the ovarian ligaments.
The overall sentinel lymph node detection rate was 90.3%.
We propose a standardized technique sentinel lymph node mapping in ovarian cancer, using indocyanine green, or Tc-99m and blue dye as alternative tracers, injected in both the suspensory and the infundibulopelvic ligament of the ovary.
- ovarian cancer
- sentinel lymph node
Statistics from Altmetric.com
HIGHLIGHTS
Sentinel lymph node mapping of the ovary seems feasible with an overall detection rate of 90%.
The utero-ovarian and the infundibulopelvic ligaments are the most common sites of injection.
The sensitivity and false-negative rate of ovarian sentinel nodes should be investigated in a prospective study.
INTRODUCTION
Pelvic and para-aortic lymphadenectomy remains a standard recommendation in the surgical management of apparent early-stage epithelial ovarian cancer, since the presence of lymph node metastases upstages the disease, requiring a different prognostic and therapeutic stratification.1 The rate of lymph node involvement in early epithelial ovarian cancer is relatively low, ranging from 6% to 30% (mean 14%).2 Lymphadenectomy may increase blood loss, operating time, and length of hospitalization. In addition, it may be associated with significant complications, such as lymphocyst formation and lymphedema.3–5 In order to reduce the associated morbidity of lymphadenectomy, sentinel lymph node mapping has evolved and become the standard of care for many gynecologic cancers.6–10
In ovarian cancer, the principle of sentinel lymph node mapping would not seem to provide value in advanced disease; however, one might consider that it would be ideal in early disease. Vanneuville et al reported the first description of sentinel lymph node identification in the ovary in 1991.11 Over the past decade, a number of authors have reported the feasibility of its use in early-stage ovarian cancer by injecting a number of different tracers into both ovarian ligaments (proper ovarian ligament and the infundibulopelvic ligament). Such studies have been characterized by small numbers of patients and by a broad range of technical approaches. Standardization of this procedure is needed before it can be tested in large multi-center studies. This review evaluates the feasibility of sentinel lymph node detection of the ovary by summarizing the published literature, comparing differences in techniques and detection rates of sentinel lymph nodes.
METHODS
A systematic search of the literature published in English was performed using PubMed and Embase, extending from June 1991 to February 2019. Two researchers (PL and FD'O) performed an independent search of the databases and selected abstracts. The search terms included 'sentinel lymph node', 'ovarian cancer', 'ovary', 'ovarian tumors'. The search string used was 'sentinel lymph node AND ovarian cancer OR ovary', 'sentinel lymph node OR ovary OR cancer'. The list of articles was supplemented by crosschecking the reference lists of the chosen articles to identify additional relevant publications. Inclusion criteria for this review were studies describing the sentinel lymph node technique and lymphatic drainage of the ovary in the English language literature, patients who had either benign or malignant disease, and patients in whom sentinel lymph node mapping of the ovary was performed even in the absence of ovarian cancer. All studies from the same research group were reviewed to identify overlapping cases. The exclusion criteria were in vitro or cadaveric studies, case reports, video articles, technical notes, review articles not reporting original data, and duplicate publications.
The following information was recorded and analyzed as main indicators: number of patients and surgical approach (minimally invasive surgery or laparotomy). Moreover, the details of the surgical procedure performed were also reported: type of injection, type and dosage of the tracers, time interval between injection and sentinel lymph node identification, sentinel lymph node mapping detection rates, and location of sentinel lymph node(s).
RESULTS
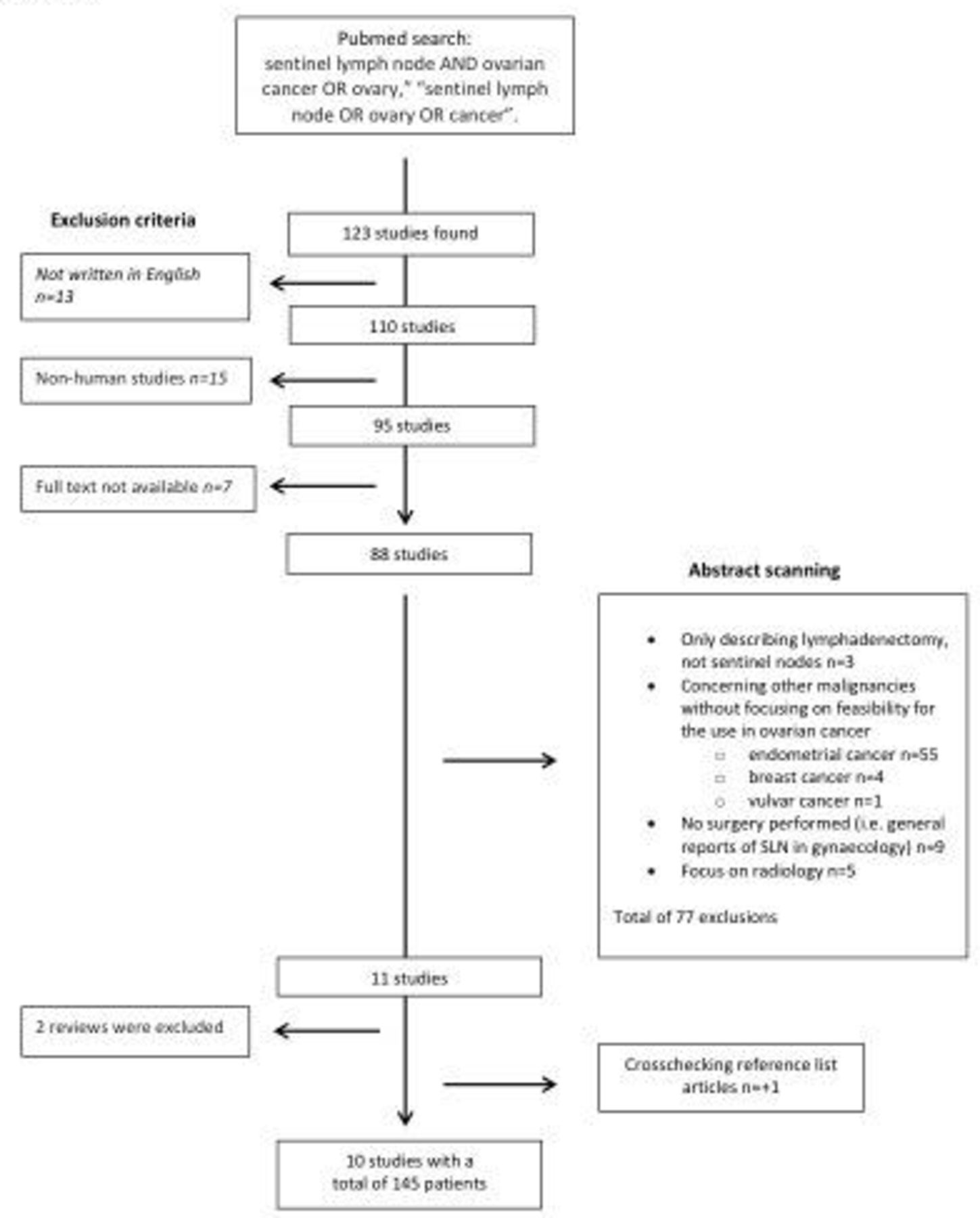
A total of 123 studies were identified and 110 were in English language. After applying additional exclusion criteria, 10 articles were selected (Figure 1). These studies included a total of 145 patients who underwent sentinel lymph node ovarian mapping evaluation (Table 1). The indication for surgery in 92 patients was gynecological cancer (59 ovarian cancer, 29 endometrial cancer, 3 cervical cancer, and 1 Fallopian tube tumor), 9 patients had a borderline ovarian tumor, while 44 patients with a suspicious ovarian mass had benign ovarian tumors confirmed at final pathology. A full lymphadenectomy was performed only when patients were diagnosed with a malignant tumor. A total of 113 (78%) patients underwent laparotomy while minimal invasive surgery was performed in 32 (22%) patients.

Flow chart of the study selection. SLN, sentinel lymph node.
Characteristics of the studies included in the revision (N=10)
Site of Injection
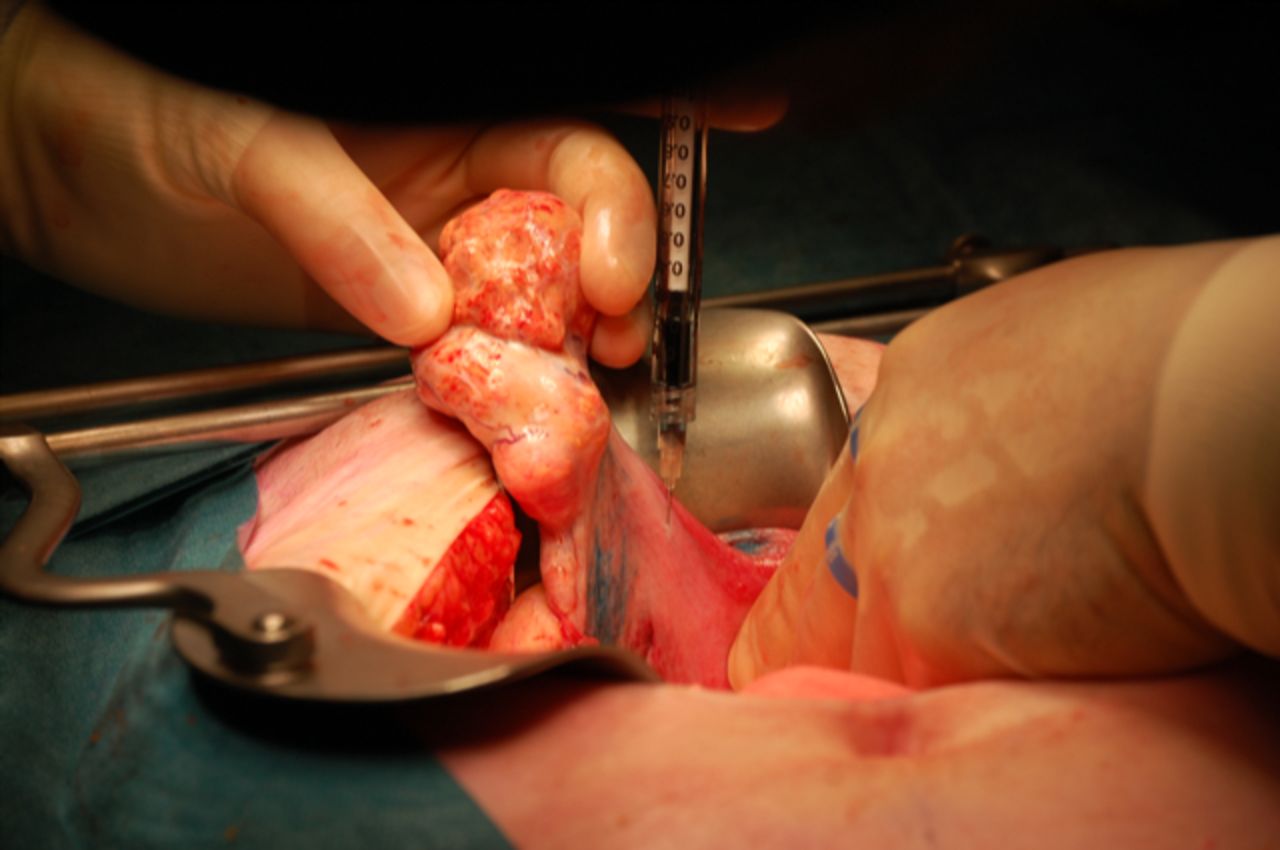
The sites of injection have varied as reported in the literature. The mesovarium was the site of injection in two studies including 14 and 20 patients, respectively.12 13 Two other studies including 16 and 5 patients, respectively, used the ovarian hilum as the injection site.14 15 The ovarian cortex has also been described as the site of injection in two studies, including 35 and 11 patients; respectively.12 16 The majority of the studies published thus far have used the proper ovarian ligament and the infundibulopelvic ligament as the site for injection (Figure 2).16–20 In total, four injections were given on the dorsal and ventral side of the proper ovarian ligament and the infundibulopelvic ligament, close to the ovary and just underneath the peritoneum. In one study, the injection was performed in the remnants of both ligaments after the affected adnexa had already been resected (n=10), either during the same surgical procedure or during a second surgical intervention.20
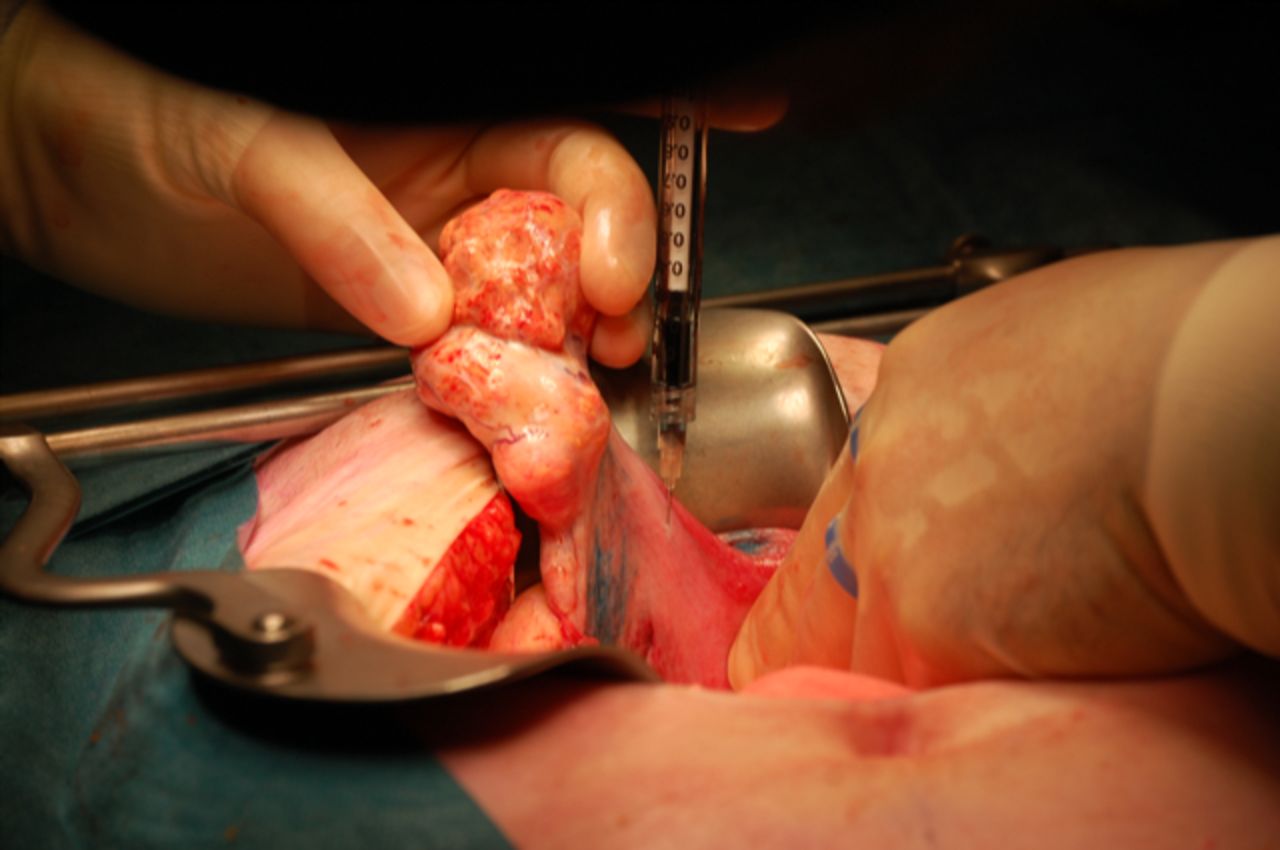
Radiocolloid and blue dye injection into the infundibulopelvic ligament of the ovary during a traditional open surgery.
In summary, the utero-ovarian ligament and the infundibulopelvic ligament were the site of injection in the majority of patients evaluated (N=69, 47.6%), the second most common site was the mesovarium (N=34; 23.4%), followed by the hilum of the ovary (N=21; 14.5%), and the ovarian cortex (N=21; 14.5%).
Type of Tracers
A variety of different types of tracers have been reported in the literature. In the majority of patients (N=109), technetium-99m (Tc-99m) was the most commonly used tracer (75.2%), either alone in 45 patients (41.3%),12 16 or in combination with patent blue in 64 women (58.7%).13 14 16 17 19 In two studies,17 19 the sentinel lymph nodes were labeled as ‘identified’ if the Tc-99m radiocolloid counts were at least 10-fold higher than the background radiation. One study considered a 'true' sentinel lymph node when it was at least three times higher than the background.16 In the study of Nyberg et al, a 'hot' node was considered when a threshold of 10-fold compared with the background was reached.13 One study used a charcoal solution (1 mL), composed of 10 mg of carbon particles, 20 nm in diameter, and 4 mg of polyvinyl pyrolidone, with a concentration of 0.05–0.2 mL.11
Finally, the injection of fluorescent tracer indocyanine green was reported in three studies including 25 patients (17%),.15 18 20 In two studies indocyanine green was injected alone (15 patients),15 18 whereas in one study indocyanine green was in combination with Tc-99m radiocolloid (10 cases).20 All investigators injected indocyanine green at a concentration of 1.25 mg/mL (25 mg phial with indocyanine green powder was diluted in 20 mL of sterile aqueous water) and 0.5–1 mL of this solution were injected.
Time Between Tracer Injection and Start of Sentinel Lymph Node Mapping
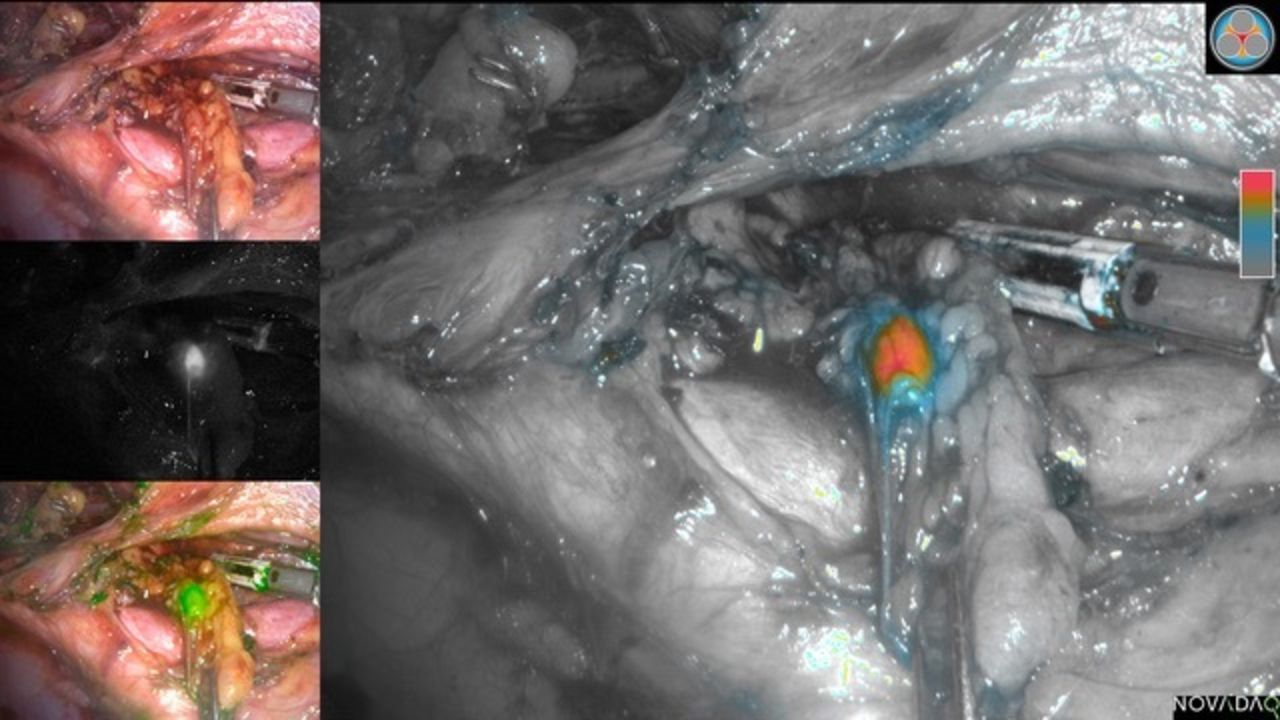
Seven studies reported the time between tracer injection and sentinel lymph node detection.11 12 14–17 19 The median time of detection was 15 min (range 2–15). In one study,12 a waiting time of 4–6 hours after injection was reported in lymphoscintigraphy analysis. Buda et al injected the tracer laparoscopically (Figures 3 and 4) and performed mapping directly after the injection.18 One study including five patients, reported a median waiting time of 2 min.12

Sentinel node mapping in the para-aortic region using indocyanine green and the Storz SPIES near-infrared technology with laparoscopy approach. (A) Final appearance of the upper aortic area. A, aorta; CV, caval vein; LRV, left renal vein; *, sentinel nodes. (B) Fluorescent view of the two sentinel nodes identified in the aortic region.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Inferior aortic sentinel node identification during laparoscopic lymphadenectomy with pinpoint Spy fluorescence camera.
Sentinel Lymph Node Mapping Detection Rates
Detection rate
Sentinel lymph nodes were found in 131 of 145 patients, an overall detection rate of 90.3% (range 40–100%). Detection rate was 88.1% when a radiocolloid (with or without blue dye) was used (N=109).11–14 16 17 19 20 When combining radiocolloid with indocyanine green the detection rate was 100% (N=10).20 Lastly, when indocyanine green alone was used, the detection rate was 93.3% (N=15).15 18 When considering the correlation between site of injection and detection rate, we noted that injection just underneath the peritoneum (ovarian ligaments, mesovarium, ovarian hilum) resulted in the detection of at least one 'hot' lymph node in the majority of patients (93.5%, N=124).11–20 In two studies, an injection into the ovarian cortex appeared to be less sensitive (71.4%, N=21).11 16 Table 2 shows the detection rate in the pelvic and aortic regions based on site of injection and dye injected. Mean detection rate in the pelvis was 44% (range 25–87.5%), whereas mean detection in aortic region was 82% (range 70–91%).
Detection rate in the pelvic and aortic regions based on site of injection and dye injected
With the exception of patent blue, all other tracers used resulted in a high detection rate of sentinel lymph nodes. In three studies, combining patent blue with Tc-99m, the number of sentinel lymph nodes identified with the addition of Tc-99m, were also identified with patent blue in 100%, 83%, and 20% in the studies, respectively.13 16 17
Sentinel Lymph Node Location
For the studies that made a distinction between the para-aortic and the pelvic region, in 69 out of 105 patients (65.7%) the sentinel lymph nodes were located in the para-aortic region only; in 13 patients (12.4%) in the pelvic region only; and in the remaining 23 patients (21.9%) in both the para-aortic and pelvic region.11 13 15–17 19 20 Two studies (n=26) reported the sentinel lymph node location to be above or below the level of the inferior mesenteric artery.14 18 Of 67 patients in whom the side location of the sentinel lymph nodes was recorded, they were identified in 63 (94%) patients only ipsilaterally, in two patients (3%) only contralaterally, and in two patients (3%) sentinel nodes were detected bilaterally.
Table 3 reports characteristics of sentinel lymph nodes and non-sentinel lymph nodes of patients with malignant ovarian tumor who underwent sentinel lymph node mapping and systematic lymphadenectomy. Among the 60 women with invasive cancer, only five studies13 15–18 reported data on sentinel lymph node characteristics. In 5/39 (12.8%) patients, lymph nodes were involved, including 8/69 (11.6%) positive sentinel lymph nodes and 5 (1.1%) of 458 non-sentinel lymph nodes. In the study of Lago et al, in which the tracer was injected in the ovarian stumps after resection of the adnexa, the sentinel lymph nodes were false negative in one patient.20 No para-aortic sentinel lymph node was identified, but after lymphadenectomy one para-aortic lymph node contained metastasis.
Node characteristics in patients with malignant ovarian tumor after SLN mapping and systematic lymphadenectomy (N=39)
DISCUSSION
This review shows that sentinel node detection from the ovary seems to be feasible with an overall detection rate of 90.3% (range 40–100%). However, a number of limitations of this approach must be highlighted. The studies differed in the exact location and number of injections and the tracer(s) used. The time interval between injection and identification of sentinel nodes was not clearly described in most studies. Furthermore, the number of studies identified and the overall sample size of patients included are too small to draw definite conclusions.
The role of lymphadenectomy in early ovarian cancer is important for assigning the stage of the disease, and also provides a tool for triaging patients who will need subsequent adjuvant therapy. However, the rate of positive nodes in early disease is approximately 14% (range 6–30%).7 Therefore, it is imperative to develop strategies that will allow surgeons to decrease the associated morbidity of pelvic and para-aortic lymphadenectomy when performing surgical staging of patients with early ovarian cancer.3–5 21 22
It has been shown that the two major lymphatic drainage pathways of the ovaries and tubes pass via the infundibulopelvic ligament and the proper ligament of the ovaries (ovarian ligament). A third minor pathway drains the ovaries via the round ligament to the inguinal lymph nodes.23 This correlates with the observation that in stage I–II ovarian cancer, lymph node metastases are found as isolated para-aortic nodes in 50% of patients, in the pelvic region in 20%, and in both the para-aortic and the pelvic region in the remaining 30%.2 24
In recent years, several feasibility studies have evaluated the technique of detecting sentinel lymph nodes in ovarian cancer by injecting the tracer(s) in the mesovarium and/or ovarian ligaments. Following the guidelines of the European Society of Gynaecological Oncology (ESGO) in ovarian cancer surgery, the operative standard in early-stage ovarian cancer is by (mid-line) laparotomy.25 For sentinel lymph node mapping, laparotomy should therefore be the first choice, particularly in the presence of large ovarian masses. According to these same guidelines, laparoscopic surgery for sentinel lymph node mapping should be considered only when a second surgery is necessary to determine staging of disease, or in the presence of small, suspicious ovarian nodules. However, others may view this approach as controversial and offer a minimally invasive approach in this clinical setting.26 27
Injection of the tracer should be performed preferably with the adnexa still in situ. Thus far, only one study, including 10 patients, has been reported on injection of the tracer in both infundibulopelvic and ovarian ligament stumps after the removal of the ovarian tumor.20 Although sentinel lymph nodes could be identified in all 10 patients, the frequency of pelvic sentinel lymph nodes alone was remarkably high (88%). Therefore, in this situation the reliability could be lower due to alteration of the lymphatic drainage after resection.
Ideally, an interval of 10–15 min should be allowed after injection, before starting the sentinel lymph node mapping. This ensures enough time for the tracer to spread to the lymph nodes (detection rate >90%). Injection of tracer both in the suspensory ligament and the infundibulopelvic ligament has been used in the majority of studies, and has shown a high detection rate (detection rate >90%). One study reported on spillage of dye from the sub-peritoneal injection site.19 To prevent this leakage, Lago et al placed clamps directly after the injection at the site of injection.20 The use of indocyanine green has been reported in three studies,15 18 20 and was associated with a high detection rate (96.7%), This tracer offers the added benefit that it avoids the radioactivity risk or radiocolloid injection by directly inject the dye in the operating room after the induction of general anesthesia for both open and minimally invasive approaches.
A prospective international study would be ideal to investigate the pathological sensitivity and false-negative rate of the sentinel nodes identified, and the possible differences in detection rate of sentinel nodes by open mapping compared with the minimally invasive approach in the presence of small ovarian masses or when retroperitoneal re-staging is planned.
Based on the results described above, we propose a standardized technique of one injection in both the suspensory and the infundibulopelvic ligament of the ovary in all patients with a high suspicion of an ovarian mass limited to the ovary. The preferred tracer, although not yet clearly defined, should be indocyanine green, even though its use has been reported in only a limited number of cases. However, recognizing that a number of centers will not have near-infrared fluorescent technology, one may propose the use of radiocolloid and blue dye as an alternative. Thereafter, the suspicious ovarian mass should be removed for frozen section analysis. After a minimum waiting time of 10–15 min, the sentinel node mapping should start and, if frozen section analysis confirms a malignancy, the staging procedure can start, including removal of the sentinel nodes identified.
Using the proposed standardized technique, a protocol is being prepared to launch an international multi-center collaborative study coordinated from Maastricht University Medical Center in The Netherlands as the lead site. The trial will be opened in several European centers. This study will explore the accuracy and benefits of the sentinel lymph node technique based on the injection of tracers in the ovarian ligaments in patients with clinical early-stage ovarian cancer.
Acknowledgments
All authors thank our friend Patricia Ann Sawchuk for her contribution to the language editing revision of the article.
References
Footnotes
Contributors FD'O and PL contributed equally to the articles research and writing. MDM searched and evaluated data from the literature. SL evaluated data and contributed to the review of the manuscript. RK and AB designed the review study, contributed, analyzed and discussed the data, wrote the draft and reviewed the final version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.