Article Text

Abstract
Background Radical hysterectomy with pelvic lymphadenectomy represents the standard treatment for early-stage cervical cancer. Results from a recent randomized controlled trial demonstrate that minimally invasive surgery is inferior to laparotomy with regards to disease-free and overall survival.
Primary Objective To investigate the oncologic safety of robot-assisted surgery for early-stage cervical cancer as compared with standard laparotomy.
Study Hypothesis Robot-assisted laparoscopic radical hysterectomy is non-inferior to laparotomy in regards to recurrence-free survival with the advantage of fewer post-operative complications and superior patient-reported outcomes.
Trial Design Prospective, multi-institutional, international, open-label randomized clinical trial. Consecutive women with early-stage cervical cancer will be assessed for eligibility and subsequently randomized 1:1 to either robot-assisted laparoscopic surgery or laparotomy. Institutional review board approval will be required from all participating institutions. The trial is coordinated from Karolinska University Hospital, Sweden.
Major Inclusion/Exclusion Criteria Women over 18 with cervical cancer FIGO (2018) stages IB1, IB2, and IIA1 squamous, adenocarcinoma, or adenosquamous will be included. Women are not eligible if they have evidence of metastatic disease, serious co-morbidity, or a secondary invasive neoplasm in the past 5 years.
Primary Endpoint Recurrence-free survival at 5 years between women who underwent robot-assisted laparoscopic surgery versus laparotomy for early-stage cervical cancer.
Sample Size The clinical non-inferiority margin in this study is defined as a 5-year recurrence-free survival not worsened by >7.5%. With an expected recurrence-free survival of 85%, the study needs to observe 127 events with a one-sided level of significance (α) of 5% and a power (1−β) of 80%. With 5 years of recruitment and 3 years of follow-up, the necessary number of events will be reached if the study can recruit a total of 768 patients.
Estimated Dates for Completing Accrual and Presenting Results Trial launch is estimated to be May 2019 and the trial is estimated to close in May 2027 with presentation of data shortly thereafter.
Trial Registration The trial is registered at ClinicalTrials.gov (NCT03719547).
- cervical cancer
- surgical oncology
Statistics from Altmetric.com
INTRODUCTION
Cervical cancer has become a rare disease in the industrialized world but remains one of the most common cancers in developing countries.1 Radical hysterectomy with pelvic lymphadenectomy is the standard of care for patients with early-stage disease. The procedure can be performed either by laparotomy or minimally invasive techniques. Laparoscopic radical hysterectomy was first described in 1992 and is widely recognized as one of the most challenging surgical procedures in gynecological oncology.2 In 2005, robot-assisted laparoscopic surgery was approved by the Food and Drug Agency for gynecological indications. The technique gained rapid popularity and has replaced conventional laparoscopy in many institutions. In the Nordic countries, laparoscopic radical hysterectomy never gained acceptance and in 2018, more than 80% of radical hysterectomies were performed with robot-assisted laparoscopic surgery in Sweden. Several studies suggest that the learning curve is significantly shorter for robot-assisted laparoscopic surgery than for conventional laparoscopy, which may be related to improved instrumentation in the robotic platform.3 In addition, retrospective analyses including two meta-analyses suggest that the oncologic safety of open surgery and robot-assisted laparoscopic surgery are comparable.4 5 However, results from a recent randomized trial have questioned the safety of minimally invasive surgery for cervical cancer. In the international Laparoscopic Approach to Cervical Cancer (LACC) trial, the final study population comprised 631 women with early-stage cervical cancer, randomized to either open radical hysterectomy or minimally invasive surgery.6 In the minimally invasive surgery group, the majority of women were treated by conventional laparoscopy (84%) whereas only 16% of the women underwent robot-assisted laparoscopic surgery. After a median follow-up of 30 months, minimally invasive surgery was inferior to laparotomy with a HR of 3.7 (95% CI 1.63 to 8.58) for recurrence and 6.0 (95% CI 1.77 to 20.3) for overall survival. The authors speculate that the use of intra-uterine manipulators, the CO2 gas, or intra-corporeal colpotomy may account for the surprising outcomes. The results from the LACC trial were, in part, supported by population-based data from the United States, demonstrating that minimally invasive surgery was associated with significantly worse survival outcomes than in women treated by open access.7 In contrast to the LACC trial, a majority of women in the minimally invasive group were treated with robot-assisted laparoscopic surgery.
In Sweden, treatment of cervical cancer is centralized to seven university hospitals and data from all radical hysterectomies are entered into a national quality registry since 2011 (Swedish Quality Register for Gynecologic Cancer, SQRGC). Based on 822 cases of radical hysterectomies 2011–2017, no difference in either disease-free survival or overall survival could be observed in the Swedish cohort (submitted for publication). Similar results have been obtained from the Danish quality register (personal communication).
In summary, the LACC trial does not reflect current practice in many countries, including the Nordic countries. The healthcare systems have gradually adopted robot-assisted laparoscopic surgery and its perceived safety is supported by data from Nordic population-based quality assurance databases. However, the LACC trial is currently the only randomized controlled trial—exploring the oncologic safety of minimally invasive surgery, and to establish the safety of current practice, a new randomized controlled trial is needed. Given the excellent outcomes in the open arm of the LACC trial, it is unlikely that robot-assisted laparoscopic surgery can generate superior outcomes. In the Robot-assisted Approach to Cervical Cancer (RACC) trial, we hypothesize that robot-assisted laparoscopic surgery is non-inferior to laparotomy but associated with less morbidity, shorter hospitalization, and superior patient-reported quality of life. In addition, we will investigate if sentinel lymph node biopsy using indocyanine green as tracer, has sufficient diagnostic accuracy to replace conventional lymphadenectomy in women with early- stage cervical cancer.
METHODS AND ANALYSIS
Trial Design
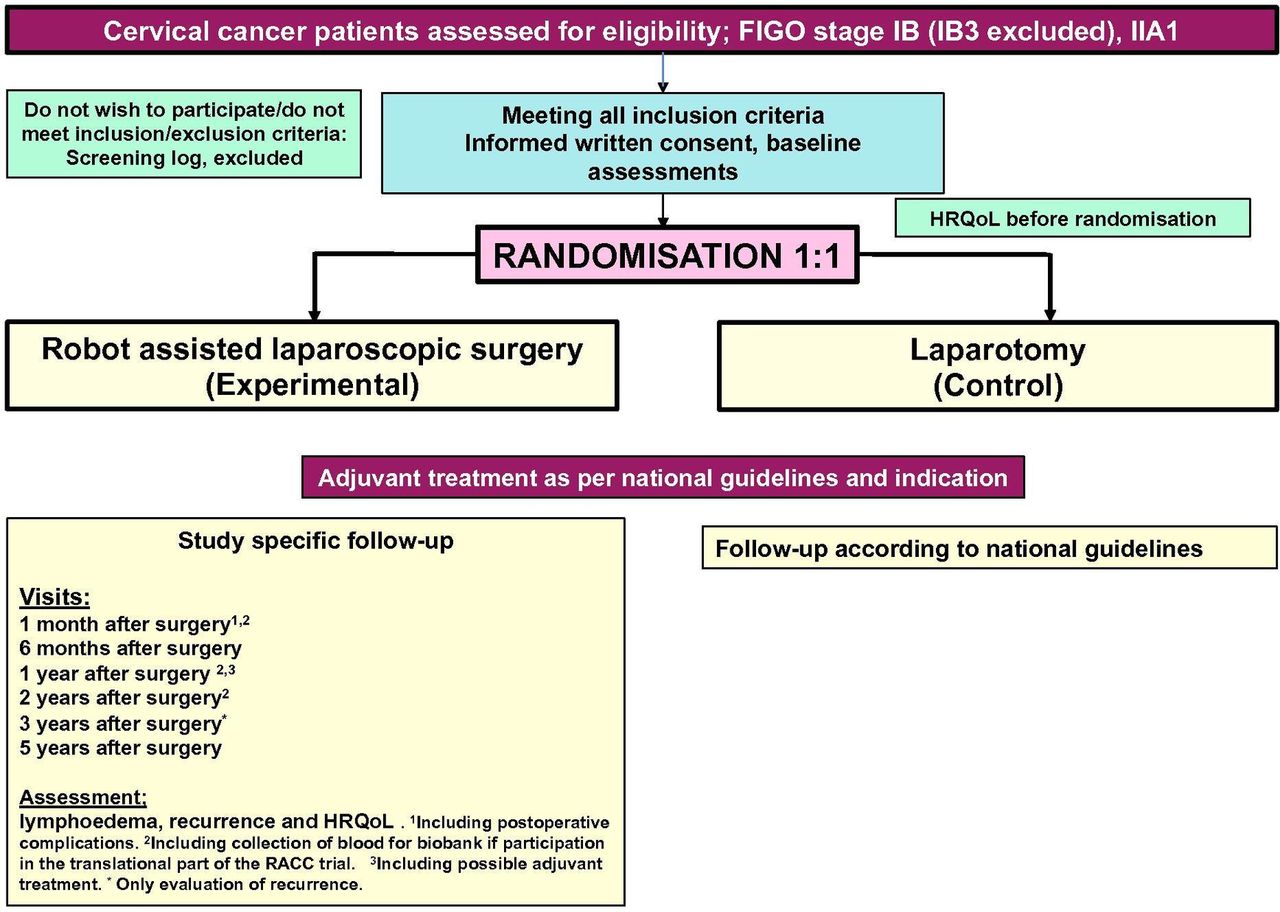
The RACC trial is a prospective, international, multi-institutional, open-label randomized controlled trial. Figure 1 gives the study schema of the RACC trial (Figure 1). Women with early-stage cervical cancer will be assessed for eligibility and subsequently randomized 1:1 to either robot-assisted laparoscopic surgery or laparotomy. Informed consent is required from all participating women. The surgical procedure comprises total radical hysterectomy according to the Querleu-Morrow classification (type B or C) and pelvic lymphadenectomy.8 The use of intra-uterine manipulators is not allowed; closure of the vagina before colpotomy is recommended but not mandatory. In addition, the sensitivity and negative predictive value of pelvic sentinel lymph node biopsy will be investigated using cervical injection of indocyanine green. To avoid any imbalance in the detection of low-volume disease based on ultra-staging between the arms, sampling (with subsequent ultra-staging) will be performed in non-mapped hemi-pelvises according to the most frequent sites of nodal metastases.9 Intra-operative complications will be classified according to Kaafarani et al and the CLASSIC classification.10 11 Post-operative complications are classified according to the Clavien-Dindo nomenclature.12 Patient-reported outcomes will be assessed at baseline (before randomization), and post-operatively at 1 month, 6 months, 1 year, 2 years, and 5 years using four different instruments: the EORTC QLQ-C30, QLQ-CX24, EQ5D, and LYMQOL. Objective assessment of lymphedema will be performed using Common Terminology Criteria for Adverse Events (CTCAE) 3.0. Finally, healthcare costs will be assessed for both modalities.

{kind=link}
Study schema of the RACC trial. HRQoL, health-related quality of life.
To date, 16 sites from across Scandinavia and Germany are expected to participate in the RACC trial with the potential to add additional sites as needed. The trial is funded by Stockholm County Council (Sweden).
Participants
Inclusion Criteria
Histologically confirmed primary adenocarcinoma, squamous cell carcinoma, or adenosquamous carcinoma of the uterine cervix.
Women with histologically confirmed FIGO stage IB (IB3 excluded) and IIA1 (with minimally tumor growth in the upper vagina).
Women undergoing either a type B or C radical hysterectomy according to Querleu-Morrow classification.
Eastern Cooperative Oncology Group (ECOG) performance status of ≤2.
Age >18 years.
Exclusion Criteria
Any histology other than adenocarcinoma, squamous cell carcinoma, or adenosquamous carcinoma of the uterine cervix.
Tumor size >4 cm, estimated by either MRI or clinical examination.
FIGO stage II–IV (except IIA1).
Women with a history of pelvic or abdominal radiotherapy.
Women who are pregnant.
Women with evidence of metastatic disease by conventional imaging studies, enlarged pelvic or aortic lymph nodes >2 cm, or histologically positive lymph nodes.
Serious concomitant systemic disorders incompatible with surgery (at the discretion of the investigator).
Women unable to withstand prolonged lithotomy and steep Trendelenburg position.
Women with secondary invasive neoplasm in the past 5 years (except non-melanoma skin cancer, breast cancer T1 N0 M0 grade 1 or 2 without any signs of recurrence or activity).
Women with iodine allergy cannot be part of the sentinel node part of the trial but are allowed randomization for the primary outcome.
Primary Endpoint
Primary Objective
This trial aims to compare the oncologic safety of robot-assisted laparoscopic surgery with standard laparotomy. Primary outcome measure: 5-year recurrence-free survival.
Secondary Objectives
To evaluate overall survival, intra-operative and postoperative outcomes 30 days after surgery, healthcare costs, quality of life and lymphedema, and the diagnostic accuracy of pelvic sentinel lymph node biopsy in women with early-stage cervical cancer. In addition, a translational part exploring biomarkers for disease recurrence is planned.
Quality Assurance of Participating Centers and Surgeons
Participating Centers
To ensure that quality standards are met, a site quality assessment form, including institutional experience with robot-assisted laparoscopic surgery, annual volume of surgical gynecological oncology cases and cervical cancer, must be completed. In addition, 10 anonymous surgery reports from both radical hysterectomies and advanced ovarian cancer primary surgeries accompanied by their histopathology reports within 24 months, have to be sent to the trial steering committee for review. Moreover, surgical variables (eg, operation time, blood loss) and complications within 30 days after surgery according to Clavien-Dindo must be reported. Furthermore, the infra-structure to participate in the trial must be satisfactory and data on institutional algorithm and indication for adjuvant treatment and what it constitutes must be reported. The total annual number of robotic procedures at each site must exceed 100. In addition, the institution's ability to perform pathologic ultra-staging is considered.
For centers participating in the sentinel node part of the trial, on-site training can be arrange by the trial steering committee if the methodology is not established. All tissue specimens removed must be reviewed by a gynecological oncology reference pathologist. Central pathology review will not be performed.
During the study, it is at the discretion of the coordinating investigators and trial steering committee to close centers with a higher than average rate of post-operative major complications from further accrual, temporarily or irrevocably after consultation with the Data Safety Monitoring Board.
Participating Surgeons
All included surgeons outside the primary investigating center must be approved by the coordinating investigators. In the site identification and quality assessment form, the participating surgeons' experience and annual caseload will be reported for review. It is at the discretion of the coordinating investigators to select or deselect individual surgeons from participating in the trial. Audits on site or videos of procedures can be requested at the discretion of the coordinating investigators. Only surgeons stated in the quality assessment form are allowed to be lead surgeons; amendments during the trial can be made.
For robot-assisted laparoscopic surgery, all included surgeons must have a previous experience of at least 20 radical hysterectomies and pelvic lymphadenectomies. For laparotomy, all included surgeons must have a previous experience of at least 20 pelvic lymphadenectomies and an annual caseload of at least 10 surgeries for advanced pelvic surgery, including pelvic lymphadenectomy. Previous experience of at least 10 open radical hysterectomies is mandatory.
Sample Size and Interim Analysis
Sample Size
The sample size is based on the hypothesis that robot-assisted laparoscopic surgery will not worsen recurrence-free survival at 5 years by more than a maximum of 7.5%. Assuming a 5-year recurrence-free survival of 85% for patients treated with standard treatment (radical hysterectomy and pelvic lymphadenectomy by laparotomy), this corresponds to a hazard rate of 1.57. The chosen non-inferiority margin is based on the margin used in the LACC trial and other similar trials.
To show that the 5-year recurrence-free survival in the robot-assisted laparoscopic surgery arm is not worse than 77.5% compared with the expected 5-year rate of 85% in the standard arm, the study needs to observe 127 events with a one-sided level of significance (α) of 5% and a power (1-β) of 80%. It is estimated that with 5 years of recruitment and 3 years of follow-up, the necessary number of events will be reached if the study can recruit 768 patients. The non-inferiority margin at 5 years correspond to a hazard ratio (HRRALS vs Standard) of 1.57. If, at the time of the statistical analysis, the upper two-sided 90% CI—this corresponds to a one-sided test at the 5% level—falls below 1.57, non-inferiority will be concluded.
The sample size is based on an observed recurrence-free survival of 85% from the SQRGC 2011–2017. However, the sample size ultimately depends on the true recurrence-free survival in the RACC trial. The following sensitivity analysis demonstrates the changes in sample size depending on true recurrence-free survival (Table 1).
Estimated sample size depending on true recurrence-free survival (RFS)
Interim Analysis
An independent safety and monitoring committee will review the data and carry out an interim analysis 3 years after the first patient is randomized or when 300 patients have been included in the study, whichever comes first. The purpose of this interim analysis is to assess the overall failure (recurrence/death) rate, to assess the recruitment to the study, and to make sure that none of the treatment groups appear to fare worse than the other.
Randomization
After verification of eligibility, signed informed written consent and baseline health-related quality of life questionnaires completed, patients will be randomized to either robot-assisted laparoscopic surgery or laparotomy by equal allocation, 1:1. The randomization procedure will be pre-stratified for participating centers. Randomization will be performed centrally by the Clinical Trials Unit at the Center for Clinical Cancer Studies, Theme Cancer, Karolinska University Hospital, Stockholm, Sweden. At the time of randomization, inclusion and exclusion criteria are entered into the randomization/registration application, which is a web-based instrument (ALEA).
Statistical Methods
The primary endpoint will be calculated from the date of randomization to the date of histology-verified local recurrence, the date of distant recurrence, or date of death (any cause), whichever comes first. For event-free patients, survival time will be calculated from the date of randomization to the date of last clinical follow-up.
Recurrence-free survival will be graphically displayed as Kaplan-Meier curves.
Differences in survival times will be tested using a stratified (center) log-rank test. The effect of treatment on time to failure will be estimated using a stratified (center) proportional hazards regression model. Results will be presented as a HR13 together with a 90% CI,9 which corresponds to the one-sided hypothesis. As this is the main endpoint in the study, a graph illustrating the estimated HR and 90% CI together with the non-inferiority margin (HR=1.57) will also be presented. All analyses of recurrence-free survival will be performed according to the intention-to-treat principle but may also be presented in accordance with protocol. Ad hoc stratified analyses will be performed for tumor size.
DISCUSSION
The unexpected results of the LACC trial have questioned the safety of minimally invasive surgery for cervical cancer.6 With an almost four times higher likelihood of disease recurrence, surgeons must now decide whether they should abandon minimally invasive surgery for this indication. As a minimum, patients must now be informed of the results from the LACC trial before a decision on surgical modality can be made. The results from the LACC trial are also supported by data extracted from the Surveillance, Epidemiology, and End Results program, showing that survival after radical hysterectomy for cervical cancer decreased annually by 0.8% after the introduction of robot-assisted laparoscopic surgery in 2005 in the United States.7
The promise of improved patient outcomes after minimally invasive surgery has been supported by multiple, retrospective studies suggesting that several parameters, including blood loss, complications, and shorter hospitalization, are superior after minimally invasive surgery compared with laparotomy.13–15 In addition, no reports before the LACC trial have indicated that the oncologic safety is compromised after minimally invasive surgery for cervical cancer. Indeed, two large, international randomized controlled trials have demonstrated similar survival for women with endometrial cancer after both open surgery and minimally invasive surgery.16 17 The confusion among surgeons is enhanced by the lack of plausible causes for the potentially worse outcomes after minimally invasive surgery for cervical cancer. Multiple reasons have been suggested, including the use of intra-uterine manipulators, intra-abdominal dehumidification by the CO2 gas or intra-corporeal colpotomy with subsequent tumor spillage in the pelvis. However, none of these potential causes are supported by the literature and remain speculative.
The timing of randomized controlled trials for procedural interventions is one of the most critical aspects to consider when a trial is later scrutinized.18 If the trial is conducted “too early”, type II errors may occur since procedures require maturation before they can be evaluated. Conversely, a randomized controlled trial initiated “too late” may lead to the perception among clinicians that the procedure has become standard of care. The most difficult parameter to assess in oncologic outcomes is, without doubt, surgical proficiency. In the LACC trial, an attempt was made to secure high-quality standards and all participating surgeons had to submit both edited and non-edited videos before they were allowed to enter the trial. However, assessing surgical proficiency is highly subjective since no objective quality standards for a radical hysterectomy exist. Most women in the minimally invasive surgery arm of the LACC trial were operated on by conventional laparoscopy and to a much lesser extent, robot-assisted laparoscopic surgery. The proportion of laparoscopic radical hysterectomy versus robot-assisted laparoscopic surgery reflects the timing of the trial and the latter had only been approved for gynecological indications 3 years before the study initiation. It is therefore reasonable to assume that the robot-assisted laparoscopic surgery procedures in the LACC trial were performed by early adopters in their early learning curve. Laparoscopic radical hysterectomy is widely recognized as one of the most difficult surgical interventions in gynecological oncology and has gradually been replaced by robot-assisted laparoscopic surgery (or never implemented at all). Most surgeons would most likely agree that robot-assisted laparoscopic surgery provides substantial benefits compared with conventional laparoscopy, including the ability to better use wrist movements owing to the improved dexterity in the robotic platform. This notion is supported by several studies demonstrating a shorter learning curve for robot-assisted laparoscopic surgery compared with conventional laparoscopy.3 19 20 Today, the majority of minimally invasive surgery radical hysterectomies are performed by robot-assisted laparoscopic surgery in Nordic countries.
Following the alarming results from the LACC trial, data from the SQRGC have been extracted. Entering data in the SQRGC is mandatory in Sweden and the nationwide coverage exceeds 99% of all procedures. Based on 852 women treated between 2011 and 2017, no difference was observed for disease-free survival between minimally invasive surgery (n=628) and laparotomy (n=263). It should be noted that all women in the former group were treated with robot-assisted laparoscopic surgery since laparoscopic radical hysterectomy has never gained acceptance in Sweden. Similar data have been obtained from the Danish Gynecological Cancer Database. Although non-randomized, the population-based data derived from these quality registers are in contrast with the results from the LACC trial. To establish the safety of robot-assisted laparoscopic surgery, a new randomized controlled trial is needed.
In summary, the international RACC trial will evaluate whether robot-assisted laparoscopic surgery is a safe alternative to laparotomy for the treatment of early-stage cervical cancer. In addition, the RACC trial will assess whether conventional lymphadenectomy can be replaced by a sentinel lymph node biopsy using indocyanine green as the tracer. The trial is expected to start accrual in May 2019.
References
Footnotes
Contributors HF, KP, SS, and JP are members of the RACC steering committee and designed the trial. AGZE, PTJ, and JM are national coordinators and contributed to the final design of the trial. PD-K, UO, LW, KS, ESL, and RK are local principal investigators. All authors were involved in revising the article critically for important intellectual content and final approval of the version to be submitted.
Funding This study was funded by Stockholms Läns Landsting (http://dx.doi.org/10.13039/501100004348).
Competing interests HF, RK, and JP are proctors for Intuitive Surgical Inc.
Patient consent for publication Not required.
Provenance and peer review Commissioned; externally peer reviewed.