Article Text

Abstract
Introduction With the global incidence of ovarian cancer set to rise by 55% to 371 000 per year by 2035, current 5-year survival rates below 50%, and 15% of women with ovarian cancer dying within 2 months of diagnosis, urgent action is required to improve survival and quality of life.
Objective To deal with the evidence gap relating to the experience of women with the disease around the globe and identify opportunities to drive progress.
Methods The study included a review of global trends in incidence, mortality, and survival (October 2017); qualitative interviews with women and clinicians in 16 countries (December 2017); and an online survey for women available in 15 different languages (open for 2 months, March to early May 2018). Women were eligible to participate if they had been diagnosed in the previous 5 years and were proficient in one of the 15 languages offered.
Results A total of 1531 women from 44 countries took part in the analysis. On average, 69.1% of women were not aware of ovarian cancer before their own diagnosis, varying from 50.9% (Hungary) to 86.4% (Brazil). A total of 78.3% of symptomatic women sought medical help, varying from 62.8% (Japan) to 87.7% (UK). Fewer than half of the women visited a doctor within 1 month (46.3%) of experiencing symptoms, varying from 38.5% (USA) to 77.3% (Germany), and a quarter of women waited 3 months or more. On average, 43.2% of women were diagnosed within 1 month of visiting a doctor, ranging from 30% (UK) to 62.3% (Italy). The average estimated time from experiencing symptoms to diagnosis was 31 weeks, but this ranged from 21.3 (Germany) to 39.7 (Brazil). Rates of post-diagnosis genetic testing ranged from 5.0% (Japan) to 79.1% (USA). Clinicians indicated that access to specialist treatment in high-volume centers varies greatly by country and region.
Conclusion The findings of this study identify some of the major challenges and opportunities to improve the time to diagnosis and management of women with ovarian cancer. These problems vary widely by country, and reducing the variability is an important first step towards improving outcomes for women with ovarian cancer.
- ovarian cancer
- ovary
- quality of life (pro)/palliative care
Statistics from Altmetric.com
HIGHLIGHTS
The time from first visiting a doctor to diagnosis varied widely by country (11 to 23.6 weeks).
A total of 51.1% of women underwent post-diagnosis genetic testing, ranging from 5% (Japan) to 79.1% (USA).
Access to specialist care in high-volume centers is variable by country and region.
INTRODUCTION
An estimated 600 000 women worldwide are living within 5 years of their diagnosis of ovarian cancer (global 5-year prevalence).1 Less than half are expected to survive beyond 5 years, and in some countries the 5-year survival rate is much lower.2 Even in highly developed economies with advanced healthcare systems, such as the USA, it is estimated that one in six women with ovarian cancer die within 3 months of diagnosis.3 By 2035, the incidence is expected to rise 55%, and mortality to reach over 250 000 cases per year, driven by increased life expectancy, population growth, and increased risk arising from economic development.4 5 Therefore, effort to improve survival and quality of life for women with ovarian cancer is an ever increasing and pressing global challenge.
The World Ovarian Cancer Coalition (the coalition) is a not-for-profit organization registered in Canada, comprising 135 patient advocacy group members in 37 countries. It was founded in 2016 by a group of international ovarian cancer patient advocacy leaders. The coalition commissioned this study to deal with the evidence gap relating to the experience of women with ovarian cancer globally, and to identify priorities for the short and medium term to improve survival and quality of life for women with the disease worldwide.
METHODS
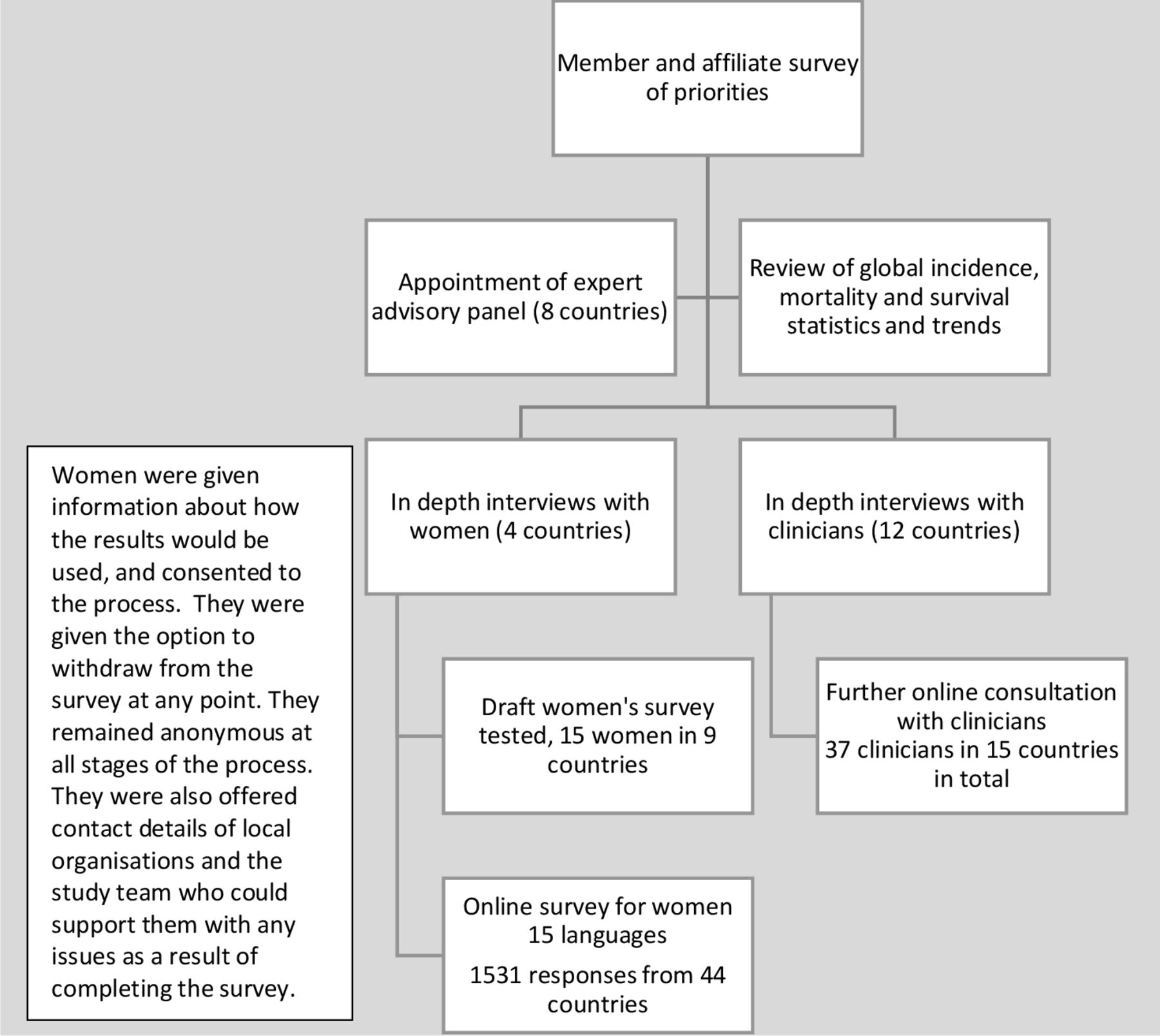
Members of the coalition were surveyed to identify priorities for the care of women with ovarian cancer, and to recommend clinicians and women who could contribute to the study development or the global expert advisory panel (the panel). Evidence relating to global incidence, mortality, survival, attitudes, and practices was collated and reviewed. Semi-structured interviews with women and clinicians were conducted and thematic analysis undertaken. The countries were chosen to capture a wide range of economic development, healthcare systems, and provision for women with ovarian cancer. An online survey for women was then developed as shown in Figure 1, and further consultation with clinicians undertaken. Ethics approval was not sought as the study was not run through any institutions, but due care was taken to protect women taking part.

Development process of the Every Woman Study.
Coalition board members, member organizations, some clinical groups, and other organizations helped to inform women about the survey, primarily by email and social media. Women were self-selecting and could participate if they had been diagnosed with ovarian cancer in the previous 5 years. They did not need to have active disease. Results were collected between March and early May 2018 until at least 1530 valid entries had been received. This figure represented the point at which, with a global 5-year prevalence of 600 000 for ovarian cancer, the results would achieve a confidence level of 95% with a CI of ±2.5%. Duplicate answers, insufficient answers, and responses from women diagnosed more than 5 years previously were discounted. Two tailed hypothesis testing was carried out at 95% confidence level and the significance threshold was set at p<0.05. Results were then reviewed by the panel who made a series of recommendations.
RESULTS
A total of 1531 entries from women in 44 countries were suitable for inclusion. Basic demographic information is shown in Table 1. Epithelial serous ovarian cancer was the most common type among participants, representing 34% of all cases. Endometrioid and clear cell ovarian cancers were the next most common. Overall, 12.5% of women did not know type of ovarian cancer they had; in Hungary this figure was 29.3%. One-third of respondents were in the 41–50 age group, one-third in the 51–60 age group, and the rest were evenly split between older and younger participants. Age and stage of diagnosis were affected by the histological type of ovarian cancer—for example, those with endometrioid, clear cell, mucinous and borderline tumors were more likely to be diagnosed with stage I than the average for all, and those with endometrioid, mucinous, borderline, and germ cell tumors were more likely to be diagnosed in those under the age of 50. In Japan, women were diagnosed with serous ovarian cancer more commonly at an earlier age, with 45.2% in the 41–50 age group (p=0.001 z=2.88), compared with 29.2% average for all serous, and just 13.5% of women in Canada (p=0.004, z=−3.52). A similar difference was found in the age profile for women in Japan with endometrioid and clear cell cancers.
Characteristics of the women in the study (n=1531)
Statistically significant variations in key points up to diagnosis, by country, p<0.05
Women with serous ovarian cancer were least likely to be diagnosed with stage I in the UK in comparison with the average for other countries (3.1% vs 9.4%, p=0.011, z=−2.54). For clear cell and endometrioid cancers, women in Japan were more likely to be diagnosed at stage I and the USA least likely (Japan 69.7%, p=0.018, z=2.38; average, 57.25%; USA, 37.2%, p=0.011 z=−2.53).
Women were asked to gauge their knowledge of ovarian cancer before their diagnosis choosing from ‘never heard of it, heard of it but knew nothing, knew something, to knew a lot’. Just 5% of women chose this last category. Over two-thirds had either not heard of it or knew nothing (69.1%), with variations by country shown in Table 2. On average, only 8.7% of women did not experience symptoms before diagnosis. This varied from 12.6% (p=0.023, z=2.27) of women with stage I disease, to 4.6% of women with stage IV (p=0.014, z=−2.47). On average, women reported four or more symptoms, at least three of which were the ones most commonly associated with ovarian cancer. This was irrespective of country, stage, and type of ovarian cancer. On average, women diagnosed with stage IV disease reported five symptoms.
Eight in 10 women who experienced symptoms consulted a doctor at some point about their symptoms, but this varied widely by country (Table 2). Of those who consulted a doctor, fewer than half went within 1 month of experiencing symptoms (46.3%), a quarter waited more than 3 months, and one in 10 waited more than 6 months. Those who had reported ‘knowing a lot’ about ovarian cancer were more likely to visit within 3 months (85.4% vs 74.8% average for all, p=0.044, z=2.02). Those who pay for some or all of their own care were least likely to seek help from a doctor of any type (72.2% vs 81.6%, p=0.048, z=1.98).
Under half of the women were diagnosed within 1 month of visiting a doctor (average 43.2%, UK 30%, Italy 62.3%, Table 2). Those who had reported ‘knowing a lot’ about ovarian cancer were more likely to be diagnosed within 1 month (58.3%, p=0.035, z=2.1). Figure 2 shows the estimated time from experiencing symptoms to diagnosis by country. It varied widely with Germany having the shortest time (21.3 weeks) and Brazil the longest (39.7 weeks). Women were asked about the first two diagnostic tests they underwent. CA125 and transvaginal ultrasound were most commonly cited by 25.4% and 21.2% of respondents, respectively, but this varied widely by country (Table 3A).

{kind=link}
{kind=link}
Estimated total time from experiencing symptoms to diagnosis in weeks, by country (n=1093). dx, diagnosis.
Statistically significant variations in diagnostic testing, treatments, genetic testing, clinical trials and information needs by country p<0.05
There is published evidence of the benefit of assessment, surgery, and treatment by ovarian cancer specialists—namely, gynecologic oncologists, in high-volume centers.6 In the development phase of the women’s survey, testers were uncertain if they had received this care, so instead clinicians were asked about their perceptions. They saw this as a vital step towards improving treatment outcomes, yet reported very wide differences between countries, from none or just a few individual centers (Hungary, Romania, India, South Africa); some regional structures (Spain, Italy); to highly established national systems (Australia, UK, Germany). Even where specialist centers exist and are well-staffed with multidisciplinary teams, many women are not referred there as often as they should. Clinicians in Germany estimated that just 50–60% of women received specialist care, in contrast to the UK where clinicians estimated the figure as 90%.
A total of 20.7% of women had chemotherapy before surgery with variations shown in Table 3A. The majority (94%) of women had surgery (primary or interval debulking), with no variation for age or stage, but in Hungary that figure was just 59%. Rates of surgery for recurrent ovarian cancer and rates of second surgery after incomplete first operations also varied, as did the use of intra-peritoneal chemotherapy. Some countries had access to targeted therapies, such as bevacizumab or poly (ADP-ribose) polymerase inhibitors, but their use was not yet widespread at the time this survey was conducted.
During development of the study, clinicians highlighted the advent of treatment with poly (ADP-ribose) polymerase inhibitors as a ‘game changer’ for women with identified mutations in their BRCA 1 or 2 genes, yet national guidance on testing and counseling was limited. Even where it did exist, implementation was far from comprehensive. Before diagnosis, only 7.6% of women had undergone genetic testing, but in Germany this figure was 15.6% (p=0.011, z=2.56). After diagnosis, half of the women had undergone testing (51.1%), varying from 5% in Japan to 79.1% in the USA (Table 3B). One in 10 women were not aware if they had a family history of ovarian cancer (10.3%), but 18.4% had family members who had previously been affected. Of these, 77.4% had just one affected relative. Of all respondents, 6.3% had a first-degree relative who had been diagnosed with ovarian cancer.
Fewer than one in four women were asked about joining a clinical trial, with wide variation by country (Table 3B). One in 10 women initiated the discussion themselves. Over 95% of women said they would be interested in future clinical trials and eight in 10 women said they would consider traveling to another hospital to participate. Over half of the respondents did not get all the information about the condition that they needed at the point of diagnosis (53.1%), and only one in five said they found all the information they needed at any point (19.7%). Variations are shown in Table 3B. Verbal information was more common than written information, and rarely went beyond generic and treatment-specific information. For one in seven women (14.3%), the doctor who told them they had ovarian cancer spent less than 5 minutes with them relaying the news about their diagnosis. The most common amount of time spent on this discussion was between 5 and 15 minutes (36%). Those who felt they did get all the information they needed were more likely to have spent a longer time with their doctor or more likely to have been given written information.
Mental health was as important to women with ovarian cancer as their physical health for their quality of life, yet this was often overlooked. Nine in 10 women have been left with long-term side effects of treatment, which include both physical and mental health problems. Fatigue was the most commonly experienced side effect (55%), followed by peripheral neuropathy (50.9%). Over a third of women (34.6%) reported anxiety, 25% depression, and a similar proportion sleep loss. Just 28% of women had been offered support by a healthcare professional for their mental health. Women were vulnerable at the point of diagnosis and also after treatment, recurrence, and if their disease was incurable.
DISCUSSION
The findings of this study identify some of the challenges and opportunities for improving the early diagnosis and management of women with ovarian cancer. In particular, the variations in metrics that occur between countries offer an opportunity to improve outcomes for women. This is the first time that patient experience on such a scale and depth has been recorded in ovarian cancer. The wealth of data offers an extraordinary opportunity to compare and contrast experiences and drive improvements in care and quality of life worldwide. It serves as a benchmark for future work, and allows clinicians, researchers, policy makers, and patient groups globally, nationally, and locally to consider how they can contribute to overcoming this increasingly urgent global problem.
This study has several limitations. Despite having 1531 responses from women in 44 countries diagnosed in the period 2013 to February 2018, most of the respondents came from few, mainly high-income countries. Although the initial interviews were able to capture and articulate some of the challenges faced by low- and middle-income countries, it remains an important ambition of the coalition to increase the accessibility of the survey for women from such countries when the study is repeated. Recruitment to the study was through email and social media platforms, with some advertising in hospitals. Thus, entrants were self-selecting, which could bias the results. The panel felt that women in the study were a younger, healthier, and wealthier group than they had expected so the results may be more positive than the true situation. This was because the study data contrasted starkly with data on short-term mortality. One study of 9491 women with stage III or IV disease in the USA (1995–2007) showed that a quarter of women died within 3 months of diagnosis.3 The National Cancer Intelligence Network in the UK examined the records of 16 943 women diagnosed with ovarian cancer between 2006 and 2008. They found that 15% died within 2 months of diagnosis.7 More recent official data from 2018 shows that 20% of women in England are unable to receive any form of treatment for ovarian cancer, primarily because they are too ill.8 Because just 3.6% of respondents in the Every Woman Study had been diagnosed within the previous 3 months, the panel felt that this reinforced their view that the study results represent the ‘best possible’ case.
Despite the limitations, the panel considered the results presented compelling information that could provide a basis for action. In particular, they noted that every country has a different mix of problems and what one country does well, another lags behind. The panel acknowledged that although there is still an urgent need for a step change in the level of investment in research for better treatments and tools for early diagnosis globally, there are significant opportunities to improve survival and quality of life for women in the immediate and short term by dealing with these variations. For example:
Women in Germany had the shortest time to diagnosis, but much less access to specialist clinicians who are key to successful treatment.
Women in the UK have almost universal access to specialists, but the lowest proportion of women diagnosed within a month of visiting a doctor.
Women in Japan had one of the shortest times to diagnosis, but very little access to genetic testing, and were least likely to get the information they needed at diagnosis.
Women in the USA were most likely to wait more than 3 months before consulting a doctor about symptoms, but most likely to undergo genetic testing.
Women in Hungary were most likely to know something or a lot about ovarian cancer before their diagnosis, but were much less likely to be offered surgery to treat their disease.
The panel made a number of key recommendations based on need that will form the basis of a Global Ovarian Cancer Charter that is to be launched in 2020:
To raise awareness of the disease as an increasingly pressing global challenge in order to build political support and funds for action.
To reduce delays in diagnosis by raising awareness of symptoms so that women seek help quickly, and family doctors and gynecologists are better able to determine who needs prompt diagnostic tests and specialist assessment.
To improve understanding of the drivers of short-term mortality, including women’s healthcare experiences before diagnosis and their biological, performance, and treatment status.
To improve knowledge about family history among women and doctors—in particular, the role of timely genetic testing and counseling to enable primary prevention and access to new targeted treatments.
To raise awareness of the importance of specialist treatment among women, family doctors, and gynecologists.
To improve data relevant to diverse populations, within trials and studies such as this, but also to improve cancer registration worldwide.
To improve women’s access to good quality relevant information and support in their own language that reflects their need for support to live well with the disease.
The World Ovarian Cancer Coalition would like to thank the many women who took part in the survey, a number of whom have since died; their members for their co-operation in developing the survey and encouraging women to participate, and the clinicians who were consulted.
Footnotes
Twitter @Frances39329305
Funding The study was funded by the World Ovarian Cancer Coalition, with no direct grants received towards the work. Some pro-bono translation support was received from Tesaro, Roche and Merck Pfizer Alliance, but they had no input into the content of the study.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data may be available from the World Ovarian Cancer Coalition, subject to approval.