Article Text

Abstract
Objective There is recent evidence that demonstrates worse oncologic outcomes associated with minimally invasive radical hysterectomy when compared with open radical hysterectomy, particularly in patients with tumors >2 cm. The aim of our study was to retrospectively evaluate the oncological outcomes between laparoscopic and open radical hysterectomy in International Federation of Gynecology and Obstetrics(FIGO) 2009 stage IB1 (FIGO 2009) cervical cancer patients with tumor size ≤2 cm.
Methods A retrospective review of medical records was performed to identify patients who underwent either laparoscopic or open radical hysterectomy during January 2010 and December 2018. Inclusion criteria were: (1) histologically confirmed cervical cancer including all histological types; (2) FIGO 2009 stage IB1; (3) tumor size ≤2 cm (determined by pelvic examination, magnetic resonance imaging or transvaginal ultrasound); (4) had undergone radical hysterectomy (type II or III) with pelvic and/or para-aortic lymphadenectomy as primary surgical treatment; (5) had follow-up information. Patients with FIGO 2009 stage IA1 or IA2, tumor size >2 cm, or who received neo-adjuvant chemotherapy before surgery, those with cervical cancer incidentally found after simple hysterectomy, or with insufficient data were excluded. Concurrent comparison between the laparoscopic and open cohorts was made for disease-free survival and overall survival.
Results A total of 325 cervical cancer patients were included; of these, 129 patients underwent laparoscopic surgery and 196 patients had open surgery. The median follow-up times were 51.8 months (range 2–115) for laparoscopic surgery and 49.5 months (range 3–108) for open surgery. Patients in the laparoscopic group had significantly worse 5 year disease-free survival than those in the open group (90.4% vs 97.7%; p=0.02). There was no significant difference in 5 year overall survival between groups (96.9% vs 99.4%, p=0.33). The Cox proportional hazards regression analysis indicated that laparoscopic surgery was associated with lower disease-free survival compared with open surgery (adjusted hazard ratio 4.64, 95% CI 1.26 to 17.06; p=0.02). In patients with non-squamous cell carcinoma or with grade II–III, laparoscopic surgery had a significantly worse 5 year disease-free survival compared with the open surgery group (74% vs 100%, p=0.01, and 88.8% vs 98.0%, p=0.02, respectively).
Conclusion Laparoscopic radical hysterectomy was associated with worse disease-free survival for stage IB1 (FIGO 2009) cervical cancer patients with tumor size ≤2 cm compared with open radical hysterectomy. Further studies may shed additional light on the impact of minimally invasive surgery in this low-risk patient population.
- cervical cancer
- laparoscopes
- laparotomy
Statistics from Altmetric.com
HIGHLIGHTS
Laparoscopic radical hysterectomy was associated with worse disease-free survival for stage IB1 cervical cancer patients with tumor size ≤2 cm.
Laparoscopy was an independent poor prognostic factor for disease-free survival with an adjusted hazard ratio of 4.64.
In patients with non-squamous cell carcinoma or with grade II–III, laparoscopic surgery had a worse disease-free survival compared to the open surgery group.
Introduction
Cervical cancer is the fourth most commonly diagnosed cancer and the leading cause of cancer death among women in the world.1 For patients with early-stage cervical cancer who do not wish to preserve fertility, radical hysterectomy with pelvic lymphadenectomy remains the standard treatment. A series of retrospective studies2–8 suggested that laparoscopic surgery and open surgery had comparable oncologic outcomes, with less perioperative complications in laparoscopic surgery. Based on these studies, minimally invasive radical hysterectomy became the standard of care for early-stage cervical cancer in centers with technical resources and trained specialists.
However, a recent prospective, randomized, international multicenter, phase III trial, the Laparoscopic Approach to Cervical Cancer (LACC) trial, suggested that minimally invasive surgery was associated with an unexpectedly higher rate of recurrence and a worse disease-free survival rate when compared with open surgery in patients with stage IA1 (lymphvascular invasion) to IB1 cervical cancer.9 In addition, a retrospective study encompassing 2461 patients from the National Cancer Database (NCDB) also showed a higher risk of death in the minimally invasive group than the open surgery group.10 These two studies have led to a change in the National Comprehensive Cancer Network (NCCN) guidelines (version 3, 2019).11 The current NCCN guidelines and European Society of Gynaecological Oncology (ESGO)12 guidelines recommendation is for open radical hysterectomy as the standard surgical approach for early-stage cervical cancer.
Subsequently, a number of retrospective studies have confirmed the inferior oncologic outcomes of laparoscopic surgery, especially in patients with International Federation of Gynecology and Obstetrics (FIGO) 2009 stage IB1 with tumor size 2–4 cm.13 14 However, there is great dispute over whether laparoscopic surgery is safe for patients with tumor size ≤2 cm. Therefore, we aimed to compare the oncological outcomes between laparoscopic radical hysterectomy and open radical hysterectomy in patients with stage IB1 and tumor size ≤2 cm.
Methods
A total of 744 cervical cancer patients with stage IB1 who underwent laparoscopic radical hysterectomy or open radical hysterectomy from January 2010 to December 2018 from three institutions were included. Our study was approved by the institutional review boards of each institution. Patients were included for analysis if they met the following criteria: (1) histologically confirmed cervical cancer including all histological types; (2) FIGO 2009 stage IB1; (3) tumor size ≤2 cm (determined by pelvic examination, magnetic resonance imaging (MRI) or transvaginal ultrasound); (4) had undergone radical hysterectomy (type II or III radical hysterectomy and pelvic and/or para-aortic lymphadenectomy) as primary surgical treatment; (5) had follow-up information. Patients with FIGO 2009 stage IA1 or IA2, tumor size >2 cm, or who received neo-adjuvant chemotherapy before surgery, those with cervical cancer incidentally found after simple hysterectomy, or with insufficient data were excluded. The final analysis included 325 patients who met the eligibility criteria: 244 patients from the First Affiliated Hospital of Wenzhou Medical University, 39 patients from the First People’s Hospital of Foshan, and 42 patients from the Taizhou Hospital of Zhejiang Province.
Adjuvant treatment was indicated after radical hysterectomy if any of the pathologic risk factors identified below were noted. Postoperative radio-chemotherapy was recommended for patients with positive pelvic nodes, positive surgical margin, or positive parametrium. In addition to high-risk factors, radiotherapy ± chemotherapy was also recommended for patients who had a stromal invasion >2/3 and lymphovascular space invasion, or patients with stromal invasion 1/3–2/3, lymphovascular space invasion, and tumor size equal to 2 cm. Chemotherapy was recommended for patients who had grade III and tumor size equal to 2 cm.
We used Student's t-test and Mann-Whitney U test to compare continuous variables and Pearson's χ2 test or Fisher's exact test to compare categorical variables. We presented categorical variables as frequency (percentage). Analyses of survival curves were performed by the Life Table method, and comparisons were made by the Kaplan-Meier methods with log-rank test, with calculation of a hazard ratio (HR), an accompanying 95% confidence interval (95% CI), and a p value. In multivariate analyses, we calculated HRs and 95% CIs using Cox proportional hazards regression models. All p values were two-sided, and we considered values of p<0.05 to be statistically significant. Statistical analyses were performed using Statistical Package for the Social Sciences (SPSS) statistical software (version 23.0; SPSS Inc, Chicago, IL)
Results
A total of 325 patients with final pathology confirmed tumor size ≤2 cm were included for analysis, after excluding 30 patients who were lost to follow-up (18 in the open surgery group and 12 in the laparoscopy group). The evaluation of tumor size was combined with pelvic examination, transvaginal ultrasound and/or MRI. The MRI and pathological measurements indicated no significant difference between the mean maximal tumor diameters (0.92±0.81 cm vs 0.95±0.75 cm; p=0.91). However, there were differences in pelvic examination and ultrasound compared with pathological measurements (p<0.001). The accuracy was estimated by the degree of agreement with a difference of 0.3, 0.5, or 1.0 cm. Based on pathological measurements, MRI seems to have a higher accuracy than pelvic examination and ultrasound (online supplementary table S1). Of these patients, 129 patients underwent laparoscopic surgery and 196 patients underwent open surgery (Table 1). The patients undergoing laparoscopic surgery were more likely to be younger, have a lower rate of lymph node metastasis, and exhibit a lower level of serum squamous cell carcinoma antigen compared with those who underwent open surgery (p<0.05) (Table 1). There were no significant differences between the two groups for histologic type, grade, lymphovascular invasion, depth of invasion, or parametrial involvement (Table 1).
Supplemental material
Clinicopathologic characteristics of patients with FIGO stage IB1 and tumor size ≤2 cm
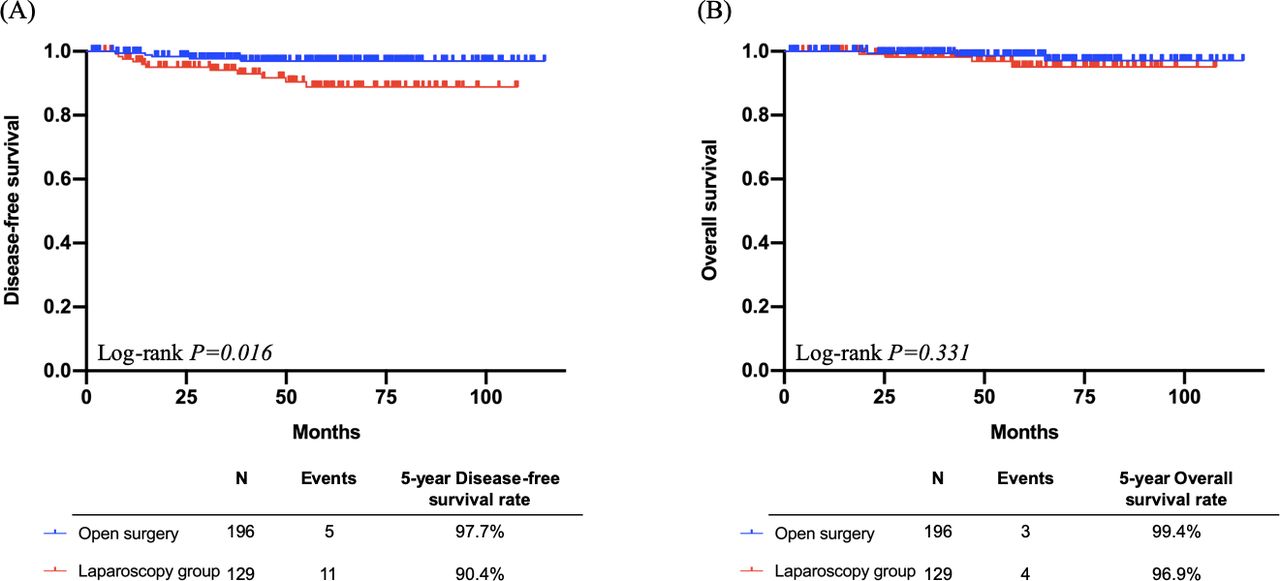
The median follow-up times were 51.8 months (range; 2–115) for laparoscopic surgery and 49.5 months (range; 3–108) for open surgery. A total of seven deaths occurred, four in the laparoscopic group and three in the open surgery group. There was no significant difference in 5 year overall survival between the groups (96.9% vs 99.4%; p=0.33). However, patients in the laparoscopic group had significantly worse 5 year disease-free survival than those in the open surgery group (90.4% vs 97.7%; p=0.02). Patients who underwent open surgery and laparoscopic surgery had recurrence rates of 2.3% and 9.6%, respectively (Figure 1).
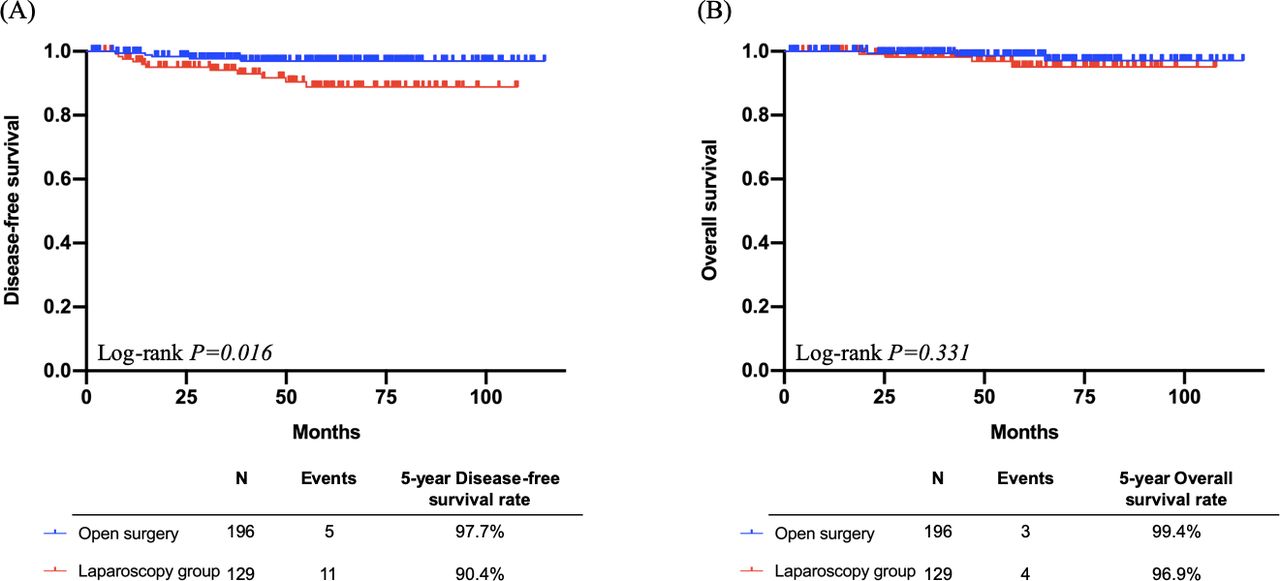
Survival outcomes of laparotomy surgery and laparoscopy surgery in patients with FIGO stage IB1 and tumor size ≤2 cm. FIGO, International Federation of Gynecology and Obstetrics.
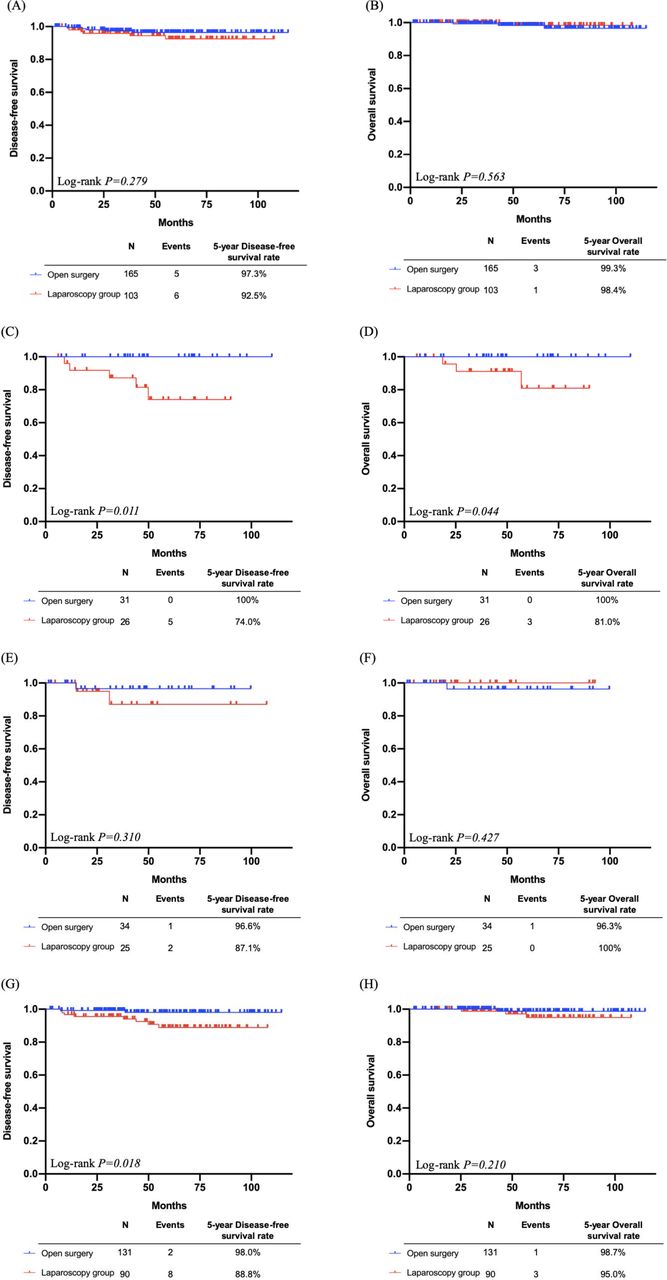
We compared the survival outcomes between the open surgery group and the laparoscopic group according to histologic type and grade (Figure 2). In patients with squamous cell carcinoma, the disease-free survival and overall survival were all similar between the two groups (p=0.28 and p=0.56, respectively) (Figure 2A&B). In patients with non-squamous cell carcinoma, the laparoscopic group had a significantly worse 5 year disease-free survival compared with the open surgery group (74% vs 100%; p=0.01) (Figure 2C), and worse 5 year overall survival (81% vs 100%; p=0.04) (Figure 2D). In patients with grade I, disease-free survival and overall survival were similar between the two groups (p=0.31 and p=0.43, respectively) (Figure 2E&F). In patients with grade II or grade III, the laparoscopic group showed significantly worse 5 year disease-free survival compared with the open surgery group (88.8% vs 98.0%; p=0.02), whereas 5-year overall survival was similar between the two groups (p=0.21) (Figure 2G&H). The Cox proportional hazards regression analysis identified laparoscopy as an independent poor prognostic factor for disease-free survival (adjusted HR 4.64, 95% CI, 1.26 to 17.06; p=0.02) (Table 2).
{kind=link}
{kind=link}
Comparisons of survival outcomes for (A,B) squamous cell carcinoma, (C,D) non-squamous cell carcinoma, (E,F) grade I, and (G,H) grade II–III.
Factors associated with disease-free survival in patients with FIGO stage IB1 and tumor size ≤2 cm
At the end of the follow-up time, 16 patients had a recurrence (11 in the laparoscopic group and five in the open surgery group). Recurrences in patients in the open surgery group were located at the vault (n=3), pelvis (n=1), and distant metastasis (n=1, lung). Recurrences in patients in the laparoscopic group were located at the vault (n=2), pelvis (n=1), distant metastasis (n=7, lung=2, bone=1, liver=1, multi-organ=3), and other (n=1) (online supplementary table S2).
Discussion
Our results demonstrated worse disease-free survival in patients with stage IB1 and with tumor size ≤2 cm undergoing laparoscopic radical hysterectomy compared with the open radical hysterectomy. These findings are very consistent with those of the LACC trial9 and the recent population database analysis10 published in the New England Journal of Medicine. However, in those studies the authors remarked that no specific conclusions could be made regarding patients with tumors ≤2 cm given the fact that the studies were not powered to answer this question. In our study, inferior disease-free survival was noted in the laparoscopic group compared with the open surgery group, but there was no significant difference for overall survival. This finding may be secondary to the fact that patients with recurrences in the laparoscopic group could have been salvaged with either chemoradiotherapy or chemotherapy alone.
In the setting of cervical cancer patients with tumor size >2 cm, there are several studies which confirmed that laparoscopic surgery has a worse survival rate than open surgery. In the large retrospective study from the NCDB with 3686 cervical cancer cases, Melamed et al10 reported that minimally invasive surgery was associated with a higher risk of death than open surgery for patients with tumor size ≥2 cm (HR 1.66, 95% CI 1.19 to 2.30). Kim et al15 studied 593 patients with early-stage cervical cancer and found that cervical cancer patients who underwent minimally invasive surgery had significantly worse progression-free survival than those in the open surgery group with tumor size >2 cm and ≤4 cm (p=0.044). In addition, Cusimano et al14 reported that minimally invasive surgery was associated with a higher rate of recurrence and death compared with the open surgery group in cervical cancer with stage IB1, and that the harm associated with this approach may be independent of surgeon volume.
Cervical cancer with tumor size ≤2 cm is considered a low-risk type. There are some studies16 17 confirming that patients with stage IB1 and tumor size <2 cm had a better 5 year overall survival, ranging from 95.2–97%. The better survival led to the update of the 2018 FIGO surgical stage for cervical cancer.18 However, there was still a debate over those patients with tumor size ≤2 cm and whether laparoscopic radical hysterectomy would lead to a poorer survival or not. Interestingly, a number of studies have shown that patients with tumor size ≤2 cm who underwent laparoscopic surgery had comparable survival to those undergoing open surgery. Kim et al19 reported that among the matched patients with tumor size ≤2 cm on pre-operative MRI who underwent laparoscopic radical hysterectomy had similar 5 year overall survival (98.6% vs. 96.4%; p=0.6) and 3 year progression-free survival (90.0% vs. 93.1%; p=0.8) compared with those undergoing open surgery. In another multicentric retrospective study from Italy,20 among patients with tumor ≤2 cm, laparoscopy showed disease-free survival superimposable to open surgery (HR 0.56, 95%CI 0.27 to 1.18; p=0.13). However, in both of these studies, the median follow-up time of the open surgery group was longer than that of the laparoscopic group (133.4 vs 46.8 months, p <0.001; 76 vs 47 months, p=0.068, respectively).
More recently, there have been numerous studies demonstrating that laparoscopic surgery was associated with worse survival compared with open surgery for patients with tumor size ≤2 cm. First, Odetto et al21 included 108 patients with stage IA1 with lymphovascular invasion to IB1 and reported that the recurrence rate in patients with tumor size ≤2 cm was 12% (7/58); three of these seven patients relapsed with carcinomatosis, which was higher than that found in the LACC trial (8.4%) including patients with tumor size <4 cm. Paik et al22 reported that laparoscopic surgery was associated with a lower disease-free survival rate (HR 12.987, 95%CI 1.45 to 116.24; p=0.003) than open surgery, but no significant difference was noted in overall survival (p=0.56) in patients with tumor size <2 cm. Uppal et al23 reported 264 patients with tumors ≤ 2 cm on final pathology, 2/82 (2.4%) recurred in the open radical hysterectomy group and 16/182 (8.8%) in the minimally invasive group (p=0.06). In the risk-adjusted analysis, the minimally invasive group approach was noted to be independently associated with a higher likelihood of recurrence (aHR 6.31, 95% CI 1.24 to 31.9; p=0.03). However, a subset of patients with prior conization and no visible tumor before radical hysterectomy had low risk of recurrence with either technique. The authors suggested this group might be an ideal cohort to be studied in future clinical trials. In our study, the 5-year overall survival was 99.4% in the open surgery group and 96.9% in the laparoscopic group (p=0.33); however, the laparoscopic group had a significantly lower 5-year disease-free survival compared with the open surgery group (p=0.016). Multivariate analysis results also demonstrated that laparoscopic surgery is an independent poor prognostic predictor for disease-free survival (HR 4.64, 95% CI 1.26 to 17.06; p=0.02). Besides this, the rate of lymph node metastasis was higher in patients who underwent open surgery than in those who had laparoscopic surgery (p=0.02). Patients who underwent laparoscopic radical hysterectomy would be predicted to have longer survival than those undergoing open surgery on the basis of the rate of lymph node metastasis. However, this was not the case.
In terms of tumor size measurement, our results also suggest that MRI seems to have higher consistency and accuracy with pathology. Several studies suggested that using MRI to measure tumor size has proven to be more accurate than pelvic examination.24–26 However, Lee et al27 reported that for patients with stage IB to II cervical cancer, pelvic examination was superior to MRI or CT in the evaluation of tumor size. The accuracy of different methods for measuring tumor diameter is still controversial.
There are several potential reasons that may account for the inferior survival outcomes of laparoscopic surgery. The use of a uterine manipulator may increase the risk of tumor spillage.28 In addition, the different approaches to handle the vaginal margin might also influence the risk of recurrence. Kong et al28 reported that the recurrence rate was 16.3% in the minimally invasive group with intracorporeal colpotomy, which was higher than that with vaginal colpotomy (5.1%, p=0.06), and the rate of a positive surgical margin was higher in the intracorporeal colpotomy group. Meanwhile, the 2 year disease-free survival was 93.7% in the vaginal colpotomy group but 80.8% in the intracorporeal colpotomy group. These findings emphasize the importance of avoiding tumor spillage and diminishing tumor handling during minimally invasive surgery. Some studies have suggested that carbon dioxide (CO2) could increase the proliferation of cervical cancer cells and cause tumor spillage.28 29 Further investigation is warranted to better comprehend the mechanism of inferior oncological outcomes of laparoscopic surgery.
According to these findings, many gynecologic oncologists have modified their approaches. In a retrospective study which evaluated patients through a sequential comparison, Kanao et al30 used the "no-look no-touch" technique in cervical cancer patients with stage IB1 to prevent direct exposure of the cervical cancer to the surgical field by use of a uterine manipulator. Their results showed that there was no significant difference in overall survival, disease-free survival, and loco-regional recurrence rate in the modified laparoscopic group and open surgery group (p=0.59, p=0.19, and p=0.57, respectively). In addition, Kohler et al31 reported that the 4.5 year disease-free survival rate was 95.8% and the 4.5 year overall survival rate was 97.8% in early stage patients who underwent vaginally-assisted laparoscopic radical hysterectomy, which could avoid use of a uterine manipulator and spillage of tumor cells, and were similar to the results of open surgery in the LACC trial.9 However, if the vaginal cuff created was not completely closed, the tumor cells would be exposed to CO2 and tumor spillage would still not be avoided. It should also be noted that in that study all patients underwent intraoperative lymph node frozen section, and if these were found to be positive for disease then the patients were excluded from the analysis.
In this study, we found that patients with non-squamous cell carcinoma or with grade II–III, laparoscopic surgery had a significantly worse 5 year disease-free survival compared with the open surgery group. Non-squamous tumors are well known to have worse survival outcomes compared with squamous cell carcinoma.32 33 Therefore, it has been suggested from retrospective studies that poorly differentiated tumors have an adverse prognostic factor for recurrence in cervical cancer.34 35 Therefore, it is not difficult to understand that non-squamous carcinoma and high-grade cervical cancers which have an aggressive tumor nature, together with the risk of laparoscopic surgery, will lead to worse survival outcomes. Especially in this study, we only included patients with tumor size ≤2 cm. Therefore, the good prognosis of these tumors may mask the adverse effects of surgical approaches during the follow-up period of this study.
The strength of our study is that we conducted research on low-risk early stage cervical cancer patients, especially cervical cancer with FIGO 2009 stage IB1 and tumor size ≤2 cm. In addition, our follow-up information is complete, which increases the credibility of our study. Limitations include the retrospective nature of the study with a limited sample size, which might introduce inevitable selection bias and confounders. In addition, we did not have a pathology review of the surgical specimens collected. Lastly, our study does not provide details on the robotic radical hysterectomy approach.
In conclusion, laparoscopic radical hysterectomy was associated with worse oncological outcomes for cervical cancer patients with tumor size ≤2 cm compared with open radical hysterectomy. Further studies may shed additional light on the impact of minimally invasive surgery in this low-risk patient population.
Infographic
![[ijgc-2019-000994supp002_INFOGRAPHIC.jpg]](https://ijgc.bmj.com/content/ijgc/30/5/564/DC2/embed/inline-supplementary-material-2.jpg?download=true){kind=link}
Acknowledgments
The authors thank Qingdong Lin, PhD for providing medical writing support. The authors also thank Jingwei Zheng, PhD for providing statistical processing support.
References
Footnotes
XC and NZ are joint first authors.
XC and NZ contributed equally.
Contributors XC, NZ and XY: Conceptualization, data curation, writing original draft preparation, manuscript preparation, supervision. PP-Y, J-HC, XW-N: Data Collection. HQZ, KZ, Y-YZ and H-LS: Data analysis and interpretation. LVDM and H-HZ: Statistical analysis. All authors read and approved the final manuscript.
Funding This work was supported by funds from the National Natural Science Foundation of China No. 81503293 (XY), the Technology Development Funds of Wenzhou City No. Y20190014 (XY), and the Zhejiang Provincial Natural Science Foundation of China No. LY19H160028 (HZ).
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. The data of figures and tables can be published.