Article Text

Abstract
Sentinel lymph node (SLN) biopsy has been investigated as an alternative to conventional pelvic and para-aorticlymphadenectomy for the surgical staging of endometrial cancer. Clinical trials have established the accuracy of sentinel nodes in the detecting metastatic disease. Novel advancements in tracers from the historically favored blue dyes and radio labeled colloids to near infrared imaging of fluorescent dyes has improved the ability to detect sentinel nodes and increased options for surgeons. The uterine cervix has been shown to be a feasible and accurate injection site for tracer, though the potential for under-evaluation of the para-aortic nodes remains a controversy, particularly for high-risk cancers. Additionally, sentinel node evaluation provides qualitatively different information than traditional staging techniques by identifying lymph nodes outside of traditional sampling locations and through the identification of very low volume meta static disease implants, such as isolated tumor cells. It is unclear how this altered staging information should be interpreted, guide the prescription of adjuvant therapy and its impact on long term clinical outcomes such as recurrence and survival. In this review we will discuss the evidence that has supported the use of the SLN technique in the staging of endometrial cancer, the options for surgical technique and the implications of managing the results of staging pathology.
Statistics from Altmetric.com
We have seen many advancements in the surgical management of endometrial cancer over the past decade with an emphasis on minimizing patient morbidity. The therapeutic virtue of routine lymphadenectomy was challenged in randomized controlled trials from Europe, and algorithms of selective lymphadenectomy were shown to be effective in sparing many women lymphadenectomy while still providing comprehensive staging information when most relevant.1–3 The adoption of the sentinel lymph node (SLN) technique for endometrial cancer has emerged as an option for surgical staging that hopefully will decrease morbidity while preserving, and possibly enhancing, staging information.
Surgical Staging of Endometrial Cancer
The use of lymphadenectomy for endometrial cancer was established as a response to observational studies which confirmed a high rate (22%) of occult metastatic disease when surgical staging is applied which includes removal and pathologic analysis of lymph nodes from the pelvic and para-aortic basins.4 The accurate identification of nodal metastases became particularly relevant when it was recognized that the use of chemotherapy was superior to radiation therapy in the survival of women with advanced endometrial cancer.5 However, subsequent randomized controlled trials have identified that lymphadenectomy alone does not improve survival for women with endometrial cancer, particularly in populations of low-risk histology and when nodal status is not used to determine adjuvant therapy.1 2 Additionally, lymphadenectomy is associated with morbidity including intra-operative complications, lymphedema, and nerve dysfunction.6 This risk is enhanced by the fact that the uterus is a central organ with bilateral lymphatic drainage, and potential drainage via pelvic and aortic pathways, thereby increasing the number of nodal regions that require surgical exploration. The omission of lymphadenectomy does not avoid patient morbidity because it increases the likelihood that morbid adjuvant therapies, such as radiation, are prescribed.7
What is SLN Biopsy?
The concept of SLN biopsy refers to the selective and directed sampling of the first-in-chain lymph nodes that drain from a malignant tumor. Dyes or tracers are injected around the tumor bed or into the affected organ, absorbed by the lymphatic pathways, and concentrated into corresponding lymph nodes. They are then visualized with specialized equipment, or in real time with visualization which guides the surgeon to the location of the tumor’s drainage pathway. Theoretically, the SLN is the node most likely to harbor metastatic disease. By selectively removing this node, it can focus lymph node resection, spare patients from the removal of large volumes of unnecessary or irrelevant nodal information, and allow more concentrated efforts by pathologists (such as ultra-staging) to detect metastases. It is particularly useful as an aid in the staging of cancers with potentially variable lymphatic drainage to multiple nodal basins. This is not a novel concept and has been well established in the treatment of breast cancers, and more recently vulvar cancer.8 9 In these cancers, clinical trials had been performed to confirm that the SLN biopsy meets the threshold of sensitivity for detection of metastases, namely that this technique has a high probability of identifying metastases when they exist.
Early Investigation
SLN biopsy for endometrial cancer was first described by Dr Thomas Burke of M D Anderson Cancer Center in 1996.10 Dr Burke and his group described a pilot feasibility study in which 15 patients with moderate to high-grade endometrial cancers undergoing laparotomy for hysterectomy received injections of isosulfan blue into the uterine fundus. They provided a description of the drainage pathways of uterine cancers that had previously only been inferred by the common locations of metastatic disease.
Following this initial description, further single-institution series were reported whose goals were to describe the feasibility of the technique and explore the optimal injection site.11–13 Surgeons at Memorial Sloan Kettering Cancer Center, led by Dr Abu-Rustum, significantly contributed to the development of the SLN technique in endometrial cancer through their early incorporation of SLN biopsy into routine surgical staging of endometrial cancer, producing large descriptive series of patient outcomes.14 15 In their work they identified that not only was this a feasible technique, but they described an algorithm for mapping and node retrieval that optimized the ability to detect metastatic disease. In their described algorithm they propose that surgeons first rule out apparent metastatic disease including suspicious nodes. If a SLN is not identified on both sides of the pelvis, a side-specific complete lymphadenectomy should be performed on the unmapped side. Doing this reduces the incidence of false-negative SLNs.15 Dr Abu-Rustum’s group observed that they could improve their false-negative rate from 15% to 2% when they retrospectively applied this alogorithm to their data. The positive effect of applying the algorithm was also seen in other prospective SLN mapping studies in which 'side-specific' analysis found very low false-negative rates (0%–5%) when the algorithm was applied.16 17 The algorithm emphasizes the importance of bilateral SLN detection because failure to identify metastases seems greatest when SLNs are absent on one or both sides. Therefore, bilateral mapping became a measure of feasibility of SLN techniques in order to minimize the number of patients subjected to completion lymphadenectomies.
Feasibility, Technique Development, and Variation
Initial studies described a heterogeneous array of SLN mapping techniques including use of different types of tracers or dyes and injection sites. This left unanswered questions for clinicians about which technique was the most feasible. While there remains no consensus regarding technique and choice of tracer, clear trends have certainly emerged.
Dye/Tracer
Traditionally SLN biopsy for malignancy has been performed with a combined or singular injection of radiolabeled colloids (such as technetium 99 (Tc99)) and visible blue dyes (such as isosulfan blue, patent blue, or methylene blue). Tc99 is usually injected and identified pre-operatively with nuclear medicine scans such as lymphoscintigraphy or single photon emission computed tomography-computed tomography (SPECT-CT). Gamma probes can be used intra-operatively to detect the presence of lymph nodes through auditory signaling. Blue dyes are injected at the commencement of surgery and can visually, in real-time, guide surgical dissection to find the sentinel node, which is then confirmed with the gamma probe.
Given their historical use in other cancers, the combination of blue dye and radiolabeled colloid were initially common choices for use in endometrial cancer staging.12 18 Some particular challenges that were encountered in the use of these dyes and tracers included the discomfort of a separate pre-operative injection, co-ordination of care with nuclear medicine departments, and the costs associated with the equipment, dyes, and additional procedures.
Indocyanine green (ICG) (Akorn, Inc. Il) is a diagnostic drug used for perfusion imaging, and more recently approved for cholangiography. It is typically injected intravenously, and when excited by a laser it emits a wavelength in the near infrared range that can be detected by specialized near-infrared imaging devices. When injected interstitially, it is carried by lymphatic pathways to lymph nodes similar to blue dyes and Tc99. In 2010 ICG was first described as a tracer for use in SLN mapping for gynecologic cancers, initially cervical cancer, and then 2 years later for endometrial cancer.19 20 Its ease of detection and quick uptake are virtues of this tracer.
The feasibility of any particular SLN mapping tracer or dye is measured by the observed SLN detection rate. The endometrium can drain to either hemipelvis or aortic side, therefore bilateral SLN detection is necessary in order to achieve an adequate evaluation. Table 1 details the results of a series of the largest studies of SLN biopsy for endometrial cancer evaluating alternative tracers and dyes.21–28
Sentinel lymph node overall and bilateral detection rates with various tracers
It appears that single-agent ICG or the combination blue dye with Tc99 appear to share the highest detection rates, typically greater than 90% overall detection and greater than 80% bilateral detection. Blue dyes used alone are associated with the lowest detection, approximately 70%, and particularly bilateral detection rates which rarely exceed 50%. Low bilateral detection rates are problematic because in accordance with the previously described SLN algorithm, these patients will require a side-specific completion lymphadenectomy at a higher rate. This failure in comprehensive mapping may offset the benefits of the simplicity of the blue dye technique.
The recently published FILM (Fluorescence Imaging for Lymphatic Mapping) trial definitively addressed the question of whether ICG was non-inferior to single-agent blue dye.27 The FILM trial was an international, multi-center, randomized, open-label, phase III trial comparing use of ICG and laparoscopic near-infrared imaging to detect SLNs (any or bilateral) as compared with the standard therapy determined to be single-agent blue dye among patients with clinical stage I endometrial cancer. All patients received both tracers with half of the population randomized to ICG analysis first, and the other half randomized to blue dye mapping first. Analysis of the 175 patients (87 and 89 in the respective groups) in an intent to treat basis showed that overall detection of SLNs was significantly higher for ICG than blue dye (96% vs 74%) as was bilateral detection (78% vs 31%), with p=<0.0001 for both analyses.
While blue dye alone should not be utilized for SLN biopsy due to inferior rates of bilateral detection, the available evidence supports the use of a combination of blue dye with Tc99 as a reasonable alternative to ICG, particularly if specialized near-infrared imaging equipment is unavailable. While this combination was not explored in the FILM trial, a European study addressed this in a retrospective, multi-institution review of 147 patients with blue dye combined with Tc99 compared with 195 patients who received ICG alone.28 With respect to overall detection rates, ICG did not differ significantly from the combined blue dye + Tc99 technique, with both above 96%; however, there was a significantly higher bilateral detection rate for the group in which ICG was used (84.1% vs 73.9%; p=0.007).
Detection rates may be the most important determinant of the feasibility of a technique, but there are other factors for surgeons to consider when choosing a technique. Limitations in accessing the necessary equipment may be one determinant as both Tc99 and ICG require specific devices to detect their signal. The literature supports the scenario whereby if surgeons have access to near-infrared imaging devices, then the use of ICG as a single agent may be best for both feasibility and patient satisfaction. It is likely that as near-infrared imaging devices become more ubiquitously available, there will be a limited role for the traditional methods of mapping utilizing radiolabeled colloids.
Patient obesity also impacts tracer selection and technique feasibility. While obesity is an independent predictor of failed bilateral SLN mapping, the use of ICG has been shown to mitigate this negative effect when compared with single-agent blue dye.21 29 30 In a retrospective review of 472 patients who had undergone SLN mapping for endometrial cancer, patients with failed bilateral mapping had a significantly higher mean body mass index (p=0.001).30 The failure to map bilaterally with increasing body mass index was somewhat mitigated by the use of ICG dye as bilateral mapping was higher for ICG (85%) compared with blue dye (54%) across all BMI groups (p=0.002). Among patients in the highest body mass index group (>40 kg/m2), SLNs were detected bilaterally in 69% of patients with ICG and only 25% of patients with blue dye. This improved detectability may be due to the ICG signal’s ability to penetrate through tissue with minimal dissection.
It is, in fact, possible to combine all three types of tracers within the same injection as a technique to take advantage of the benefits of all three tracer types. How et al described mixing blue dye (0.8 mL) with ICG (0.1 mL of 0.25 mg/mL) and Tc99 (0.1 mL).25 In their prospective analysis of 100 patients, they observed a 76% bilateral detection rate with this combination. This is comparable to what has been observed with single-agent ICG, and therefore there may be limited benefit to the use of all three tracers. The addition of blue dye to ICG can help surgeons to visualize the SLN during dissection if they feel uncomfortable operating in the near-infrared modality necessary for ICG visualization.
Injection Site
The choice of injection site for the tracer is another question that has been explored for SLN mapping in endometrial cancer. Options for injection sites include the cervix or uterine fundal sites such as uterine serosa, fundal myometrium, and the endometrium (peri-tumoral). Advocates of the uterine fundal site injections argue that these sites are logical choices given their proximity to the tumor and the anticipation that these would reproduce the drainage of the endometrium most accurately, particularly to the para-aortic region. Use of these injection sites dominated early SLN research and they are particularly popular during open procedures.10 11 13 Fundal and serosal injections likely lost favorability as minimally invasive surgery increasingly became the most popular surgical route for endometrial cancer staging because serosal and fundal injections are relatively more complex using laparoscopic instrumentation. The cervix, however, is easily accessible and can be reliably injected with minimal additional equipment, even in minimally invasive surgeries, and therefore the cervix soon became a popular site for injection.
Several studies have compared hysteroscopic with cervical-site injections. Table 2 gives the reported detection rates (overall, para-aortic, and isolated para-aortic) for the five larger reported prospective series that compare hysteroscopic or subserosal injection to cervical injection.31–35 Certainly rates of para-aortic node detection are higher in studies utilizing fundal-site injections (hysteroscopic or subserosal). However, there appear to be greater overall detection rates and more consistent results with cervical injections. Additionally, there is significant variability in detection of para-aortic nodes with fundal injection sites with the detection of para-aortic nodes ranging between 10% and 75%. This may be a function of the difficulty in comprehensively assessing the para-aortic region in all patients, as well as inconsistency in surgeons’ reporting of whether a SLN was a true first-in-chain SLN or an upper echelon node. First-in-chain nodes refer to the SLN that is found closest to the site of injection. It is the first node to take up dye from the origin channels in the parametrium, though it frequently communicates with subsequent nodes along the same channel, so-called upper echelon nodes. Theoretically, the first-in-chain SLN has the highest likelihood of containing metastatic disease as it is the first to receive lymphatic drainage from the tumor. Therefore, it is the most critical SLN to identify and remove. There are likely multiple factors including tracer choice, injection site, and surgeon compulsivity that contribute to accurate detection of para-aortic SLNs and nodal metastases.
Rates of sentinel lymph node detection following uterine fundal versus cervical injection
Cervical injection is straightforward, reproducible, and does not require complex additional time, equipment, imaging, or skills. Therefore, while there is no consensus regarding the optimal injection site, the cervix is likely to become the chosen preferred site for clinicians due to its high feasibility and detection rates, with a caveat that surgeons should pay close attention to the para-aortic region particularly in high-risk patients.
Establishing the Accuracy of SLN Biopsy for Endometrial Cancer
Once the SLN technique for endometrial cancer was shown to be feasible, its accuracy in detecting metastatic disease as compared with conventional lymphadenectomy needed to be established. In order to estimate the accuracy of the technique, studies require large numbers of patients subjected to both SLN evaluation and comprehensive lymphadenectomy. These studies report their findings with measures of sensitivity (the proportion of patients with metastatic disease who have positive SLNs), negative predictive value (the proportion of patients with negative SLN results who do not have metastases), and false-negative rate (the proportion of patients with metastatic disease who will have negative SLN specimens, or failure to identify disease with the test).
In 2011 the results of the SENTI-ENDO study from France were published.17 This trial was the first multi-institutional prospective study to address the question of accuracy of the SLN technique in endometrial cancer. SENTI-ENDO included 125 evaluable patients of whom 111 mapped at least one SLN following cervical injection of blue dye and Tc99. This study reported 100% sensitivity and negative predictive value of the SLN per hemipelvis. Consequently, the SLN accurately identified metastatic disease within the hemipelvis in which it was located. However, when analyzed at the patient level, rather than by pelvic side, the sensitivity dropped to 84% representing three missed pelvic node metastases on the contralateral side to a negative SLN. The results of this study reinforced what had been reported by Dr Abu-Rustum’s group at Memorial Sloan Kettering with respect to the importance of performing comprehensive nodal assessments in nodal basins that fail to map a SLN. While all patients in SENTI-ENDO received a pelvic lymphadenectomy, only 12% underwent routine para-aortic nodal evaluation despite more than a third of the patients having deeply invasive tumors or cervical involvement. This raised the possibility that the results overstated the accuracy of the SLN study by under-assessing the non-SLN regions.
Similar to the preceding SENTI-ENDO study, the FIRES (Fluorescent Imaging for Robotic Endometrial cancer Sentinel lymph node biopsy) study36 was a prospective, multi-institutional trial, this time in the United States, and included patients who had undergone both complete lymphadenectomy and SLN biopsy using a standardized technique. Unlike SENTI-ENDO, the FIRES study was powered at the whole-patient level, rather than the hemipelvic level. Of the 293 enrolled patients who mapped at least one SLN, 37 lymph node-positive patients were identified among whom one patient had positive non-SLNs but negative SLNs, representing a false-negative SLN result. This study estimated that the technique was associated with a sensitivity of 97.2%, negative predictive value of 99.6%, and false-negative rate of 2.8%. Interestingly, there was a low rate of bilateral detection (52%). One explanation for the low bilateral detection rate observed in the FIRES study was the learning curve due to the fact that all but one participating surgeon were novices with the SLN mapping technique at the study’s inception. However, despite this limitation, the unilaterally detected SLNs were very effective at identifying metastatic disease. These results can only be extrapolated to patients who map to at least one SLN. In the FIRES study, 47 patients failed to map any SLNs and five of those patients (11%) harbored occult lymph node metastases. As such these results support the use of the SLN algorithm to identify all patients with metastases.
The results of the SENTI-ENDO and FIRES studies were supported by a large meta-analysis study.37 Among nearly 5000 patients from 55 accumulative studies, the sensitivity of SLN mapping in detecting metastatic disease reached 96% with a pooled negative predictive value of 99.7%. These low false-negative rates are comparable to, if not better than, those observed in breast cancer (10%) and vulvar cancer (8%), both cancers in which SLN is an accepted staging modality.8 9
SLN Biopsy for High-Grade Cancers
The results of the FIRES study were encouraging for surgeons because they demonstrated the clinically acceptable diagnostic accuracy of this technique. However, there was some concern about whether these results could be extrapolated to patients with high-grade cancers, who are at higher risk for pelvic and isolated para-aortic nodal metastases.
This question, namely whether SLN biopsy can be safely applied to patients with high-grade cancers, has been addressed in several observational studies and prospective trials. Table 3 summarizes the results of these trials with respect to numbers of patients with high-grade cancers and sensitivity and negative predictive data.16 36 38–41 Whether or not para-aortic nodes were evaluated is also listed because this is an important determinant as to whether these studies were able to address the occurrence of isolated aortic metastases.
Accuracy of sentinel lymph node biopsy in high-grade endometrial cancer
The largest, dedicated clinical trial that has addressed this question was conducted by Soliman et al.38 This single institution, prospective trial enrolled 101 evaluable patients with exclusively high-grade cancers. The authors defined high risk as serous, clear cell, carcinosarcoma and FIGO (International Federation of Gynecology and Obstetrics) grade 3 endometrioid histology, patients with biopsy-proven cervical involvement or deeply invasive (on imaging) grade 1 or 2 disease. They performed SLN mapping with cervical injection of the surgeons’ choice of tracer. All patients received pelvic lymphadenectomy and 95% of the patients received a para-aortic lymphadenectomy above the level of the inferior mesenteric artery, with approximately half (46%) undergoing lymphadenectomy to the level of the renal vessels, 18% to the level of the inferior mesenteric artery, and 29% above the inferior mesenteric artery but below the renal vessels. SLNs were detected in 89% of patients, with 58% found bilaterally. One false-negative SLN result was observed among the 20 node-positive patients who mapped at least one SLN, yielding a 5% false-negative rate and a 95% sensitivity for the technique in this high-grade, high-risk population.
Similar results were identified in a study of 42 patients with high-grade cancers by Papadia et al, which included patients with poorly differentiated endometrioid, clear cell, serous, carcinosarcoma, or neuroendocrine histology who had undergone SLN mapping in addition to complete pelvic and infrarenal para-aortic lymphadenectomy.39 Their observed SLN false-negative rate was 10%, with the sole false-negative result occurring in a clinically suspicious lymph node in the para-aortic chain with associated negative pelvic SLNs. If the SLN algorithm had been applied, which mandates removal of all clinically suspicious nodes, this patient’s node would not have been missed. This result is comparable to the subgroup from the FIRES cohort, 29% of whom had high-grade cancers.36 Of the 100 patients with high-grade cancer and SLNs detected, there was one false-negative SLN. Rates of aortic evaluation were also high in this study, with aortic nodes removed in 74% of patients with high-grade cancers.
The oncologic outcomes, such as survival, for patients with high-grade non-endometrioid cell types have also been reported using retrospective analyses of high-volume institutions. In a review of 136 patients with carcinosarcoma, 48 of whom had staging with SLN biopsy, 88 of whom had staging with complete lymphadenectomy, there was no difference in median progression-free survival observed.42 It should be noted that the lymphadenectomy group represented a historical cohort and had significantly longer duration of follow-up. Additionally, while both groups received similar rates of adjuvant therapy, there were differences in the patterns of prescribed therapies, likely a reflection of the use of a historical cohort and an increasing trend towards the use of adjuvant chemotherapy.
Significance of Para-Aortic Lymph Node Evaluation in the Era of SLN Biopsy
Traditional dogma emphasizes the importance of the para-aortic basin in the surgical staging of endometrial cancer. Its origins came from the observation that in approximately half of patients with pelvic lymph node metastases, there are concomitant para-aortic node metastases.4 Additionally, the para-aortic nodes may be the sole site of metastatic disease, which would be otherwise overlooked if only pelvic lymph node basins were evaluated. In reality, this occurs in approximately 2% of all patients with endometrial cancer, but at a substantially higher rate (16%) of patients with higher-risk features (such as high-grade lesions and deeply invasive lesions).3
The SLN biopsy technique has gained criticism for its under-evaluation of the para-aortic nodal basin as most SLNs are found in the pelvic regions, particularly after cervical injection. However, as discussed in earlier sections of this review, even in studies which feature comprehensive para-aortic node evaluation in high-risk patients, there are few examples of missed isolated para-aortic nodal disease.36 38 39 The improved evaluation of the pelvic nodes (either through ultrastaging of SLNs or by identification of nodes in atypical locations) may in fact minimize the number of missed 'isolated' para-aortic nodes that are in fact co-existing with previously under-diagnosed pelvic nodal metastases.
Surgeons are recommended to closely evaluate the para-aortic nodal basins for both SLNs or clinically suspicious nodes as part of the SLN algorithm. The decision to remove normal appearing, non-sentinel para-aortic nodes is at the discretion of the surgeon, determined by the perceived clinical benefit of the procedure.
Survival Outcomes in SLN Biopsy Patients
Lymphadenectomy has not been shown to improve survival in women with endometrial cancer.1 2 However, given the known importance of systemic adjuvant therapy for node-positive patients, and the poor reliability of clinical assessment of nodes, pathologic nodal evaluation remains important.4 5
The question of improved oncologic outcomes for SLN biopsy in endometrial cancer has not been studied in a well-designed randomized trial. A large patient population size enriched for high-risk patients would be necessary. In the absence of such data we look to observational studies that have addressed the question of oncologic outcomes associated with SLN biopsy.
The oncologic outcomes of 266 women with high-intermediate and high-risk endometrial cancer at two Italian centers was evaluated.43 Fifty-three percent had undergone lymphadenectomy, 23% SLN mapping with algorithm, and 25% no lymphadenectomy. No difference was measured in disease-free and overall survival.
A collaborative retrospective evaluation was conducted between two institutions: the Mayo Clinic whose practice was to perform selective comprehensive pelvic and aortic node dissections only for patients with 'high-risk' uterine features, and Memorial Sloan Kettering Cancer Center who performed SLN biopsy on all patients.44 In their pooled results of 1135 cases, no difference in 3-year disease-free survival rates (94.9% and 96.8%, respectively) was observed. The Mayo Clinic approach resulted in surgeons performing fewer pelvic node dissections with more total nodes removed, but had a significantly lower incidence of observed pelvic node metastases (2.6% compared with 5.1%). The Mayo group performed more aortic dissections than the group from Memorial Sloan Kettering Cancer Center; however, they identified the same proportion of para-aortic nodal metastases. The conclusion was that either staging strategy was reasonable. It should be noted that these were sequential cohorts and therefore these data may have been impacted by unmeasured confounders in treatment and outcomes arising in the two different time periods.
Consistent with the findings above, a Canadian group retrospectively evaluated the oncologic outcomes of 472 cases of endometrial cancer surgeries which included their most current 275 patients who had undergone staging with SLN biopsy, and a historical cohort of 197 patients who had undergone systematic lymphadenectomy.45 They observed no difference in recurrence-free survival between the two groups but a significantly lower incidence of pelvic side-wall recurrences in the SLN group (30% vs 71%). These data raised the possibility that SLN biopsy may not just be equivalent to conventional staging but may actually increase the detection of metastatic disease, resulting in optimal adjuvant therapy prescription. Superior detection of disease may result from the identification of aberrant lymphatic pathways and nodal basins not traditionally explored by conventional complete lymphadenectomies, and second through the application of ultrastaging techniques which can identify very low-volume metastases previously overlooked by conventional pathologic processing.
Alternative Lymphatic Drainage
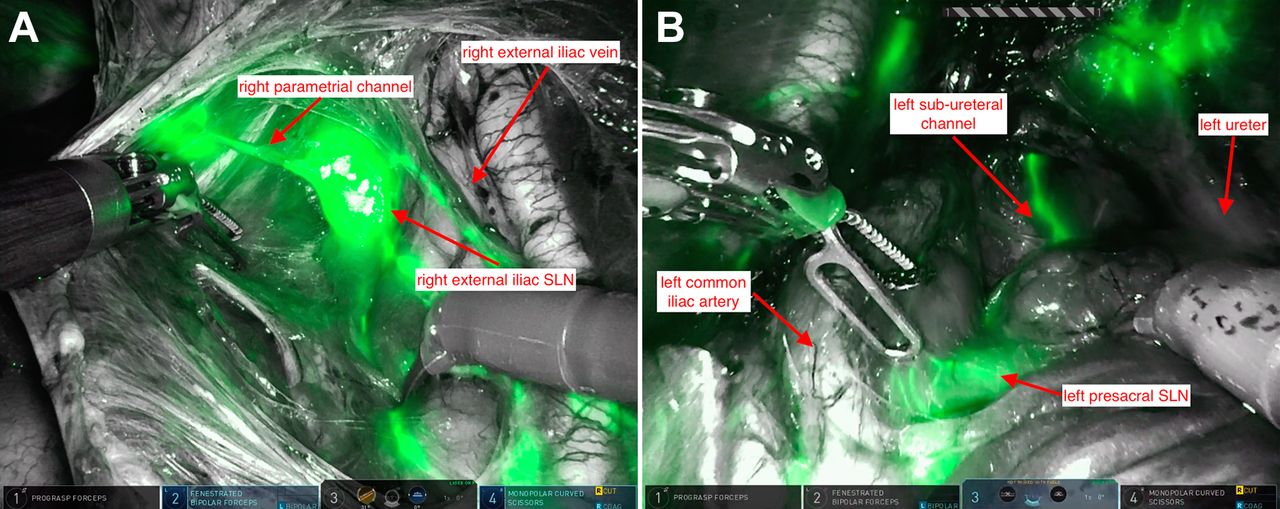
Two common major lymphatic pathways have been identified following cervical, hysteroscopic, or myometrial injections that traverse the parametrial lymphatic trunk (Figure 1).10 These two most common pathways include the more common laterally directed pathway in which lymphatics pass ventral to the uterine vessels and internal iliac artery before entering the nodes in the proximal obturator space (at the bifurcation of the external and internal iliac vessels) or on the medial surface of the external iliac vein (Figure 1A). A less common pathway turns cephalad, rather than laterally, as it exits the parametrium, and travels dorsal (or deep) to the ureter (Figure 1B). This channel typically enters a sentinel node on the sacral promontory. Identification of these channels requires careful dissection of the para-rectal space. It is important to note that there may be more than one true sentinel lymph node in a hemipelvis depending on the complexity and variability of a patient’s lymphatic pathways, as they can bifurcate prior to entering nodes.

{kind=link}
Common routes of lymphatic drainage detected with indocyanine green and da Vinci XiTM robotic surgical system (Intuitive Surgery Inc.). (A) Right parametrial channel to lateral side wall nodes. (B) Left sub-ureteral channel to pre-sacral nodes. SLN, sentinel lymph node.
In the FIRES study, participating surgeons were asked if the identified SLNs were located in chains that were within or outside of the traditional boundaries of lymphadenectomy.36 Approximately 17% of identified SLN’s were located outside of traditional lymphadenectomy basins with a similar proportion of patients with stage IIIC disease having nodal metastases identified exclusively in these atypical regions which would have been overlooked by conventional node dissections.
How et al evaluated their SLN mapping results for uncommon pathways of lymphatic drainage with SLN and the association with metastases.46 They similarly identified SLNs found in regions of the pre-sacrum, internal iliac, and parametrial locations, outside of traditional node dissection boundaries. These SLNs in atypical locations represented 13% of removed SLNs. Ten percent of patients with node-positive disease contained disease only in SLNs found in atypical regions, and therefore only detected with the SLN mapping procedure.
It is a reasonable hypothesis that improved detection of metastases in these atypical SLN locations may contribute to the observation of increased pelvic node metastases and decreased pelvic side-wall recurrences following SLN biopsy.45 47
Significance of Low-Volume Metastases
Traditional handling of lymph node specimens by pathologists typically involves bivalving specimens longitudinally and submitting each side for hematoxylin and eosin (H&E) processing. However, many advocate that SLNs should be subjected to more scrutiny, which is more feasible given the paucity of tissue that requires pathologic analysis. The technique advocated for SLN processing is called ultrastaging. In this process, SLNs which are greater than 3 mm are sectioned serially in a bread loaf fashion (ultra-sectioned). Paraffin-embedded specimens are taken from each slice, with one subjected to H&E processing and the other reserved for immunohistochemistry (IHC) stains to cytokeratin (typically AE3 and AE 4) if the H&E stained slides are found negative. The immunohistochemistry processing is better capable of detecting very low volume metastatic disease.
The Austral-Asian Journal of Cancer (AJCC) classifies lymph node metastases by virtue of size.48 Micrometastases range in size between 0.2 and 2 mm and are commonly found in the subcapsular region of the lymph node. These micrometastases may be identified with conventionally H&E stains, and historically have been detected with traditional processing and sectioning techniques, however the immunohistochemistry processing technique substantially enhances the ability to detect these small collections.
The lowest volume metastases are called isolated tumor cells. Unlike micrometastases, these individual malignant cells, or clusters of malignant cells less than 0.2 mm in dimension, are rarely if ever identified with traditional pathology processing, and therefore they are a novel phenomenon and present the greatest controversy in the new era of SLN biopsy for endometrial cancer. While the novel identification of previously undetected disease is enticing, it is unknown if this low-volume disease is clinically significant.
Isolated tumor cells make up approximately 40%–50% of the patients with node-positive disease in reported studies.17 36 37 Evaluation of a large series of patients with otherwise 'low-risk' disease such as grade 1 or 2 histology and minimal myometrial invasion demonstrated that use of ultrastaging doubled the identification of positive lymph nodes from 2.6% to 5.9%.49 Early retrospective data identified that recurrence-free and overall survival of patients with isolated tumor cells, most of whom were treated with adjuvant therapy, was favorable compared with those patients with macrometastases and was similar to patients without metastatic disease.50 This raised the question of whether these improved outcomes were secondary to identification and treatment, or because these metastatic foci are clinically insignificant.
Emerging data have suggested that low-volume metastatic disease, particularly isolated tumor cells, appear to be associated with otherwise favorable prognostic features. Patients with isolated tumor cells are less likely to harbor co-existing non-SLN metastases. Low-volume metastases are more likely to be associated with inner-half myometrial invasion, and grade 1 endometrioid histology.51
Investigators evaluated single-institution outcomes of 85 SLN-positive patients and categorized them according to volume of metastatic disease.52 Thirty-one patients housed isolated tumor cells in their SLNs. One third of the patients received adjuvant therapy with chemotherapy and radiation, one third received whole pelvic radiation, and one third (10) of patients received no therapy or vaginal brachytherapy. No patients who received no adjuvant therapy recurred. The recurrence-free survival for patients with isolated tumor cells was similar to that of patients with no metastatic disease and significantly superior to patients with macrometastatic disease. In particular, the prescription of adjuvant therapy was not controlled.
Certainly these retrospective data suggests that there is a real question regarding the clinical significance of isolated tumor cells, and possibly of the virtue of ultrastaging techniques as a whole. However, until this can be assessed by prospective trials, most clinician advocate continuing ultrastaging of SLNs for endometrial cancer, and making judicious treatment decisions based on the results. There are certainly good data to support the treatment of micrometastases in a manner similar to macrometastases, particularly as many of these lesions are detected via conventional pathologic processing. However, clinicians and patients could reasonably make treatment decisions based on uterine pathology features for patients with isolated tumor cells.
Conclusions
There has been much progress in the field of SLN biopsy for endometrial cancer in the past decade. SLN biopsy has emerged as a standard technique for the staging of endometrial cancer. The National Comprehensive Cancer Network Guidelines include SLN biopsy as a standard technique in the surgical staging of endometrial cancer, stating that “sentinel lymph node mapping may be considered”, and that this technique no longer carries the caveat that it remains under investigation.53 While there is high-level evidence supporting the accuracy of SLN biopsy and the optimal techniques, certainly there is little level 1 evidence supporting oncologic outcomes, impact on morbidity, and its influence on treatment algorithms. These are important clinical research questions to resolve in the coming decades as clinicians continue to reduce the morbidity and improve the accuracy of endometrial cancer staging.
References
Footnotes
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned, externally peer reviewed.