Article Text

Abstract
Objective Tumor volume and regression after external beam radiotherapy have been shown to be accurate parameters to assess treatment response via magnetic resonance imaging (MRI). The aim of the study was to evaluate the prognostic value of tumor size reduction rate after external beam radiotherapy and chemotherapy prior to brachytherapy.
Methods Patients with locally advanced cervical cancer treated at two French comprehensive cancer centers between 1998 and 2010 were included. Treatment was pelvic external beam radiotherapy with platinum based chemotherapy followed by brachytherapy. Records were reviewed for demographic, clinical, imaging, treatment, and follow-up data. Anonymized linked data were used to ascertain the association between pre-external and post-external beam radiotherapy MRI results, and survival data.
Results 185 patients were included in the study. Median age at diagnosis was 45 years (range 26–72). 77 patients (41.6%) were International Federation of Gynecology and Obstetrics stage IB2-IIA disease and 108 patients (58.4%) were stage IIB-IVA. Median tumor size after external beam radiotherapy and chemotherapy was 2.0 cm (range 0.0–8.0) and median tumor size reduction rate was 62.4% (range 0.0–100.0%). Tumor size and tumor reduction rate at 45 Gy external beam radiotherapy MRI were significantly associated with local recurrence free survival (P<0.001), disease free survival, and overall survival (P<0.05). Tumor reduction rate ≥60% was significantly associated with a decreased risk of relapse and death (HR (95% CI) 0.21 (0.09 to 0.50), P=0.001 for local recurrence free survival; 0.48 (0.30 to 0.77) P=0.002 for disease free survival; and 0.51 (0.29 to 0.88), P=0.014 for overall survival).
Conclusions Tumor size reduction rate >60% between pre-therapeutic and post-therapeutic 45 Gy external beam radiotherapy with concurrent chemotherapy was associated with improved survival. Future studies may help to identify patients who may ultimately benefit from completion surgery, adjuvant chemotherapy, and closer follow-up.
- imaging tool
- uterine cervix cancer
- concomitant chemoradiotherapy
- treatment response assessment
- risk of recurrence
Statistics from Altmetric.com
- imaging tool
- uterine cervix cancer
- concomitant chemoradiotherapy
- treatment response assessment
- risk of recurrence
HIGHLIGHTS
Magnetic resonance imaging after external beam radiotherapy may help identify patients at risk of recurrence.
Residual tumor size after external beam radiotherapy is associated with decreased survival.
Tumor size reduction >60% after external beam radiotherapy predicts improved survival.
Introduction
Cervical cancer is the fourth most common cause of cancer related death among women worldwide.1 Although cervical cancer is often curable if detected early, more than one-third of patients are diagnosed with locally advanced disease. Prognosis and treatment depend on the stage, which was mainly based on physical examination until the last 2018 classification of the International Federation of Gynecology and Obstetrics (FIGO).2 Magnetic resonance imaging (MRI) is a useful tool in the evaluation of the local and regional spread of disease.3 Guidelines from the European Society for Medical Oncology, the National Cancer Institute, and the American Society of Clinical Oncology recommend the use of pelvic external beam radiotherapy with concurrent low dose platinum based chemotherapy followed by brachytherapy as standard treatment for locally advanced cervical cancer patients.
The response to chemoradiotherapy in patients with locally advanced cervical cancer may be adequately evaluated by the use of MRI. One study on sequential MRI performed before, during, and after chemoradiotherapy showed that pre-therapeutic tumor volume and tumor regression ratio, after 45 Gy external beam radiotherapy, were the strongest predictors of local recurrence.4 Mayr et al identified that residual tumor volume ≥20% at MRI after 45 Gy external beam radiotherapy, and ≥10% after the end of chemoradiotherapy, were significantly associated with decreased disease specific survival.5 However, there are a paucity of data regarding the actual timing and specifics on MRI tumor measurements.
The aim of our study was to determine the prognostic and therapeutic value of tumor size reduction rate at MRI after 45 Gy external beam radiotherapy with concurrent chemotherapy prior to brachytherapy.
Methods
Patients and Treatment
Patients with locally advanced cervical cancer (2009 FIGO stage IB2 to IVA) and negative aortic staging treated at Oscar Lambret Cancer Center, Lille, and Claudius Regaud Cancer Center, Toulouse, France, between November 1998 and November 2010, were retrospectively included. Institutional review board approval was obtained from both centers. Patients who's post 45 Gy external beam radiotherapy MRI results were not available were excluded. Preoperative workup included, in all cases, physical examination, cervical biopsy, and MRI and fluorodeoxyglucose positron emission tomography/computed tomography (PET/CT) evaluation. Laparoscopic retroperitoneal para-aortic lymph node staging was performed in patients with no aortic nodal uptake on preoperative PET/CT. Pre-therapeutic MRI results did not modify either FIGO staging or therapeutic strategy.
All patients underwent pelvic external beam radiotherapy combined with 5 courses of concomitant weekly 40 mg/m2 cisplatin chemotherapy. Radiotherapy was delivered to the whole pelvis in 25 fractions of 1.8 Gy for a total dose of 45 Gy within 5 weeks. Gynecologic examination and MRI 1.5 T with gadolinium were performed during the first week after completion of 45 Gy external beam radiotherapy prior to brachytherapy. Diffusion weighted imaging, and T1 and T2 weighted sequences with axial and sagittal planes acquired obliquely axed on the cervical canal were performed. Cervical tumor presented high signal intensity on T2 weighted sequences. Tumor size was defined as the largest tumor dimension measured on MRI T2 weighted sequences (in cm).
To evaluate the therapeutic response to 45 Gy external beam radiotherapy with concomitant chemotherapy, the reduction rate in tumor size was calculated. This rate was defined as the ratio between tumor size at MRI before treatment and post 45 Gy external beam radiotherapy. Subsequent treatment varied depending on the type of response at the MRI evaluation. MRI tumor measurements were performed by radiologists experienced in gynecologic oncology imaging. Adequate response was arbitrarily considered when the reduction rate in tumor size was ≥50%. In the case of an adequate response, treatment was completed with additional pulsed dose rate intracavitary brachytherapy for a total equivalent dose of 80–90 Gy in the cervix. Additional boosts were given after brachytherapy in cases of pelvic lymph node and/or parametrial involvement in pre-therapeutic MRI for a total equivalent dose of 60 Gy. When intensity modulated radiation therapy was available, simultaneous integrated boost was performed on metastatic pelvic lymph nodes, at doses of 57.5 Gy in 25 fractions. In the case of a poor response (tumor size reduction rate <50%), completion treatment was left to the discretion of the attending radiotherapist: 35 Gy brachytherapy alone or 15 Gy preoperative brachytherapy followed by completion surgery, which ranged from radical hysterectomy to pelvic exenteration after 6 weeks in order to achieve removal of the residual tumor with clear margins. Follow-up included clinical examination every 4 months for 2 years and every 6 months for the 3 following years.
Statistical Analysis
Data were summarized by frequency and percentage for qualitative variables, and by median (range) for continuous variables. Local recurrence free, disease free, and overall survival were calculated from the date of post-radiotherapy MRI and were estimated by the Kaplan–Meier method with 95% CI and HR, using the following first event definitions: local relapse alone for local recurrence free survival, relapse of any kind or death from any cause for disease free survival, and death from any cause for overall survival. Univariate analysis was performed using the log rank test for qualitative variables and the Cox proportional hazards model for continuous variables. A minimum P value approach was used to dichotomize tumor size reduction rate. Tests were two sided and P values <0.05 were considered statistically significant. All statistical analyses were conducted using STATA 13.0 software.
Results
A total of 185 patients were included in the study. Median age at diagnosis was 45 years (range 26–72) and median body mass index was 22.7 kg/m2 (range 15.4–49.0). Seventy-seven patients (41.6%) were FIGO stage IB2-IIA and 108 patients (58.4%) stage IIB-IVA. Median pre-therapeutic tumor size at the MRI evaluation was 5.0 cm (range 2.0–15.7). Compared with physical examination, MRI at diagnosis found a more locally advanced disease in 55 patients (29.7%) and a less locally advanced disease in 25 patients (13.5%). The histological types were squamous cell carcinoma in 154 patients (83.7%), adenocarcinoma in 22 patients (12.0%), mixed tumor in 5 patients (2.7%), undifferentiated carcinoma in 2 patients (1.1%), and adenosquamous carcinoma in 1 patient (0.5%). All patients had a laparoscopic para-aortic lymph node staging before starting treatment and none had aortic lymph node involvement. Pelvic lymphadenectomy was also performed at the same time as aortic staging in 18 patients (9.8%), of whom 10 had pelvic lymph node involvement (Table 1).
Demographic data
All patients received 45 Gy external beam radiotherapy with concurrent chemotherapy. Among them, 155 patients (83.8%) were treated with platinum based chemotherapy while 30 patients (16.2%) received a combination of cisplatin and fluorouracil, cisplatin and gemcitabine, or carboplatin alone. Fifty-two patients (28.1%) received an additional boost of external radiotherapy as lymph node or parametrial involvement was seen on pre-therapeutic MRI. Among them, 14 (26.9%) were treated with intensity modulated radiation therapy integrated boost.
Median tumor size after external beam radiotherapy and chemotherapy was 2.0 cm (range 0.0–8.0) and median tumor size reduction rate was 62.4% (range 0.0–100.0). A total of 132 patients (71.4%) were considered adequate responders—tumor size reduction rate ≥50%. A complete therapeutic response with no residual tumor was observed in 53 (40.2%) of these 132 patients at the post 45 Gy external beam radiotherapy MRI evaluation. Among the adequate responders, 118 (89.4%) received the standard protocol with 35 Gy of additional brachytherapy. In the remaining 14 patients (10.6%) with an adequate response, the protocol treatment was not followed. Two patients (1.5%) received 20 Gy and 25 Gy brachytherapy, respectively. One patient (0.8%) received 35 Gy of additional external radiotherapy on the cervix. Two patients (1.5%) did not receive further treatment. Four patients (3%) underwent a surgical procedure and five patients (3.8%) had 15 Gy preoperative brachytherapy followed by completion surgery 6 weeks later (Figure 1).
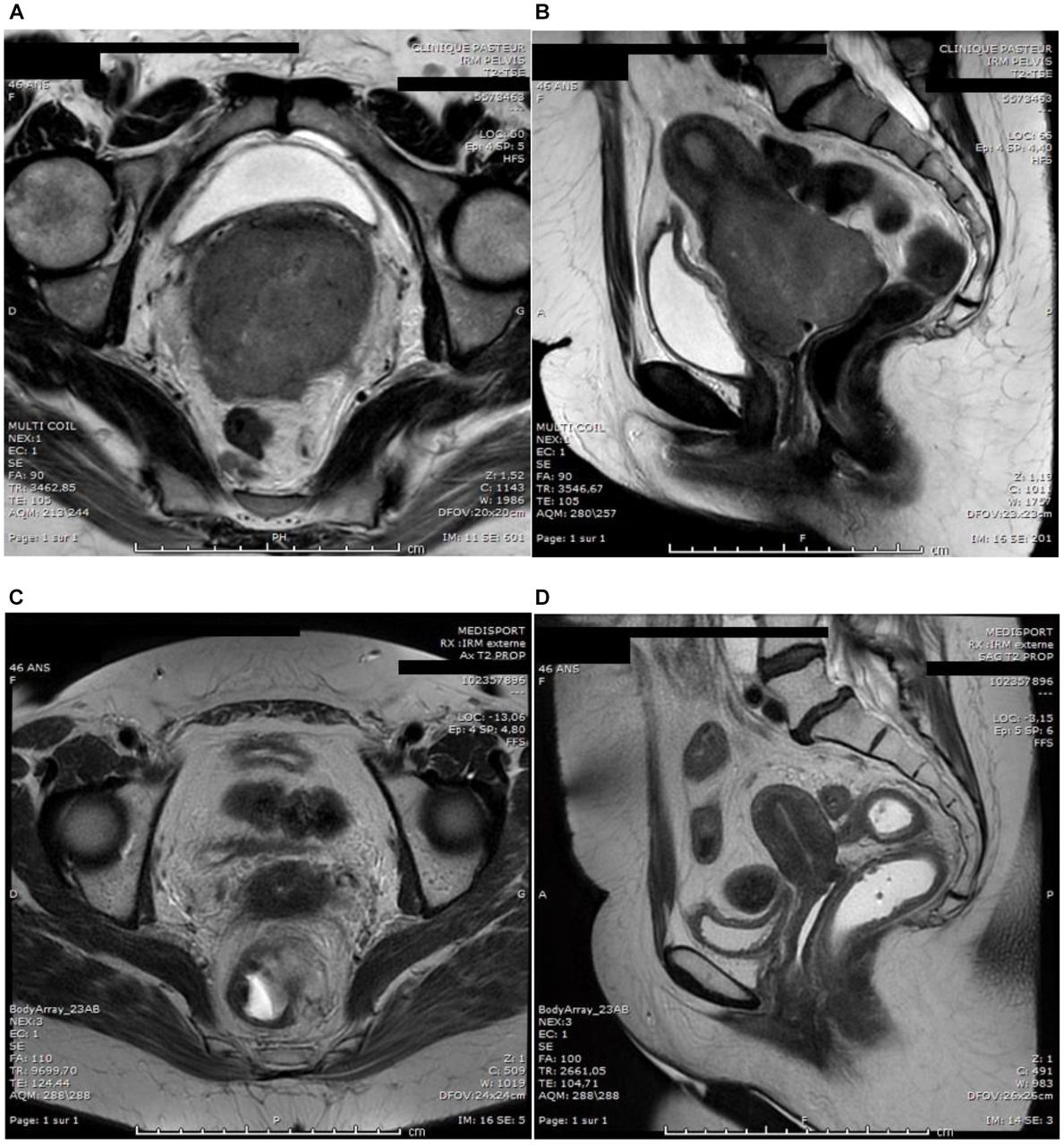
(A) Axial T2 weighted image of diagnostic magnetic resonance imaging with a cervical adenocarcinoma. (B) Sagittal T2 weighted image of the same patient. (C) Axial images after 45 Gy external beam radiotherapy and concurrent chemotherapy. (D) Sagittal images after 45 Gy external beam radiotherapy and concurrent chemotherapy.
Among the 53 (28.6%) poor responders (tumor size reduction rate <50%), 5 patients (9.4%) underwent preoperative 15 Gy brachytherapy followed by radical hysterectomy, 7 patients (13.2%) underwent completion surgery, and 41 patients (77.4%) received brachytherapy alone. Among these 41 patients, 33 patients (62.3% of the 53 poor responders) were managed with 35 Gy brachytherapy and complete response was observed at the end of the treatment. The other 8 patients (15.1% of the 53 poor responders) were treated with suboptimal brachytherapy due to uterine perforation in 4 cases and suboptimal dose (10 Gy or 20 Gy) of brachytherapy in the other 4 cases. The treatment strategy was modified by post-radiotherapy MRI in 12 of 185 patients (6.4%). Median delay between the end of external beam radiotherapy or brachytherapy and surgery was 59 days (range 26–120 days)—in 9 good responders and 12 poor responders. Median treatment duration of external beam radiotherapy with brachytherapy was 57 days (range 13–156).
After a median follow-up of 65.5 months (61.5–71.9), 53 patients (28.6%) were dead, 75 patients (40.5%) had recurrence of disease, and 31 (16.8%) had local recurrence. Five year overall survival, disease free survival, and local recurrence free survival were 71.9% (95% CI 64.2 to 78.3), 59.4% (95% CI 51.6 to 66.4), and 81.3% (95% CI 74.3 to 86.5), respectively. Tumor size and tumor reduction rate at 45 Gy external beam radiotherapy MRI were significantly associated with local recurrence free survival (P<0.001), disease free survival, and overall survival (P<0.05, Table 2). Total radiotherapy treatment duration, including brachytherapy, was also significantly associated with overall survival (P=0.025, Table 2).
Univariate analysis for disease free survival and overall survival
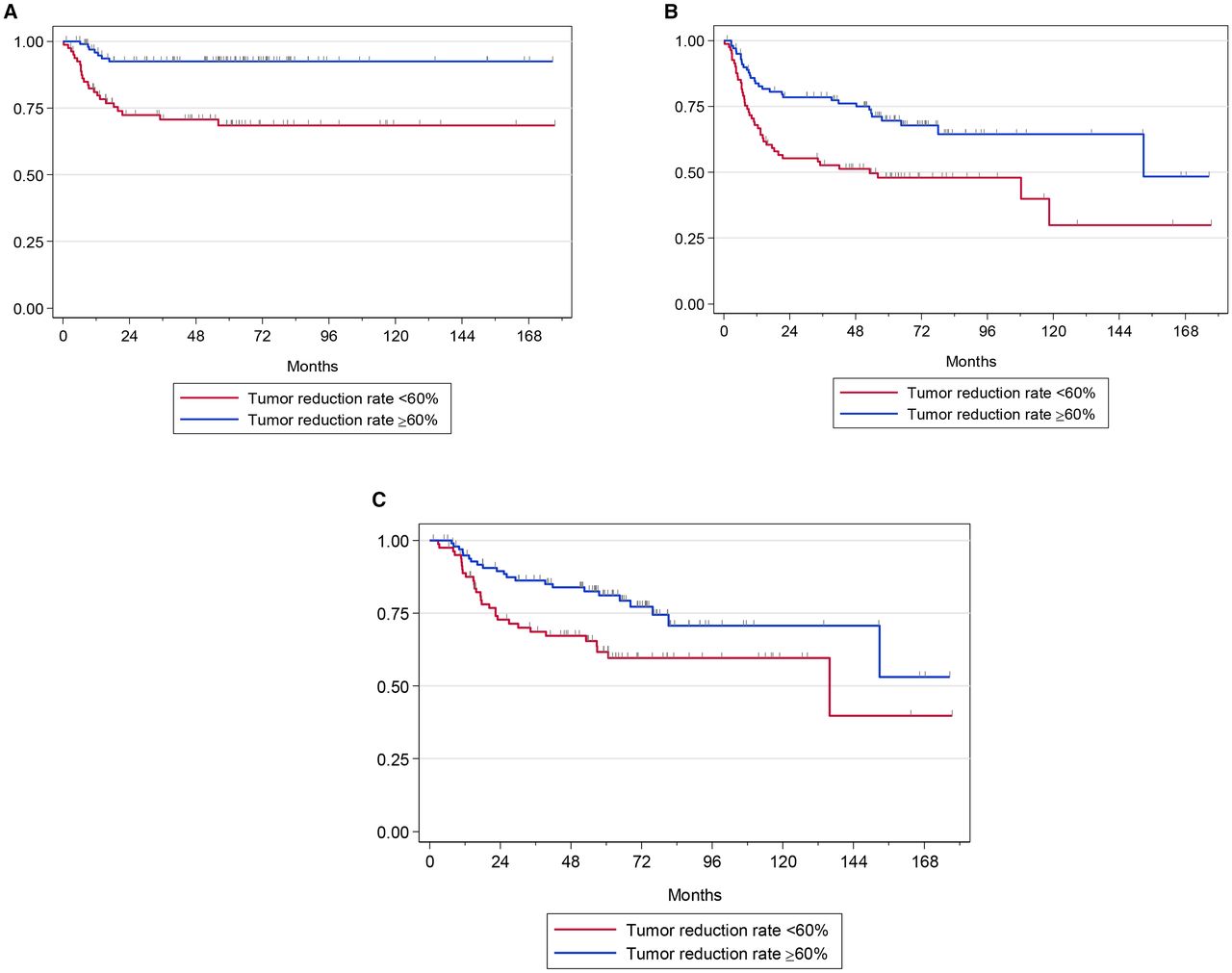
Tumor reduction rate with a cut-off of 50% was not significantly associated with disease free survival or overall survival. The effect of tumor reduction rate on survival was also evaluated using cut-off values of 60% and 80% (Table 2). Tumor reduction rate ≥60% was significantly associated with a decreased risk of relapse and death (HR (95% CI) 0.21 (0.09 to 0.50) P=0.001 for local recurrence free survival; 0.48 (0.30 to 0.77), P=0.002 for disease free survival; and 0.51 (0.29 to 0.88), P=0.014 for overall survival, Figure 2). After adjustment for other associated factors with a P value <0.1 in the univariate analysis, tumor size reduction rate of 60% remained significantly associated with disease free survival and overall survival in the multivariate analysis (HR (95% CI): 0.52 (0.27 to 0.98), P=0.044 for disease free survival and 0.54 (0.31 to 0.96), P=0.036 for overall survival).
{kind=link}
{kind=link}
Local recurrence free, disease free, and overall survival according to 60% tumor size reduction rate at post-external beam radiotherapy magnetic resonance imaging
Discussion
In France and other European countries, the initial workup after diagnosis of locally advanced cervical cancer systematically includes an MRI.6 MRI may also be performed at the end of external beam radiotherapy and concurrent chemotherapy to assess treatment response. Different MRI tumor measurements and different time points to perform this evaluation have been reported previously.4 7–9 There is a large amount of published data evaluating the role of MRI evaluation prior to initiation of therapy. Previous data suggest that cervical local extension can be more effectively assessed by MRI rather than by clinical examination.10–13 MRI has also been shown to be superior to CT and physical examination for evaluating uterine body involvement and measuring tumor size.10 11 However, tumor size can be overestimated when comparing MRI with histological results after surgery.11 One study reported that MRI found a more locally advanced disease in approximately one-third of patients, which is consistent with our results.9 In our study, compared with physical examination, initial MRI found a more locally advanced disease in 29.7% of patients and a less locally advanced disease in 13.5%. We also found that the primary discordance in clinical and MRI findings was in parametrial evaluation, which is concordant with data in the literature.12 14 In this series, 29 patients (15.6%) would have been upstaged to FIGO IIB based on MRI results. Other series concluded that clinical assessment of parametrial invasion was improved when performing additional MRI.13 MRI was also superior to CT for parametrial evaluation, with sensitivities to determine parametrial invasion of 74% (95% CI 68 to 79) for MRI and 55% (95% CI 44 to 66) for CT.12 A meta-analysis of 15 relevant studies comparing PET/CT with MRI concluded that PET/CT did not increase the accuracy of local cervix evaluation compared with MRI,15 and that there were no significant differences in tumor size on PET/CT versus MRI images.15–18 Other studies have evaluated the benefit of associating PET/CT and MRI in the pre-therapeutic evaluation. Fused PET/MRI has better diagnostic performance than PET/CT in local evaluation due to improved detailed information regarding local tumor extension and parametrial invasion. PET/MRI also has higher diagnostic performance in detecting lymph node metastases.19 The predictive value of pre-therapeutic MRI tumor measurements has been investigated in several series. Tumor diameter and volume in pre-therapeutic MRI were associated with a higher risk of recurrence and death.7–9 However, in our series, initial tumor size was not associated with patient outcome.
Wang et al studied serial MRI during and after chemoradiotherapy to compare the sensitivity and specificity of the tumor regression metrics and to identify the optimal time to perform MRI in order to identify patients at high risk of recurrence.4 In our study, the largest tumor diameter measured in pre and post-external beam radiotherapy MRI was used, as it is less time consuming and more easily reproducible than volume parameters. Indeed, the different cut-offs employed to compare volumetric parameters are variable between studies.20 Outcome prediction of combined pre-therapeutic and 4 week chemoradiotherapy MRI volume regression ratios were demonstrated to be highly accurate in predicting local recurrence and death.4 In our series, a 60% reduction rate in tumor size after 45 Gy external beam radiotherapy MRI was the best predictor of long term survival. In contrast, Mayr et al found that residual tumor volume ≥20% on MRI evaluation after 45 Gy radiotherapy was associated with decreased disease free survival.5 In our study, no significant survival difference was observed in patients with tumor size reduction rates ≥80%, probably because of the lack of statistical power due to the low number of events.
Differentiating residual tumor from post-radiotherapy fibrosis and inflammation might be challenging. Post-radiotherapy evaluation can be improved by functional MRI, including diffusion weighted imaging, dynamic enhanced MRI, and PET/MRI. Dynamic MRI permits evaluation of tumor response to chemoradiotherapy by analysis of tumor hypoxia and tumor interstitial pressure.21 Apparent diffusion coefficient has been identified as a good biomarker and modifications of its value during chemoradiotherapy have been associated with treatment response and survival.22 A prospective cohort study in which 92 women underwent PET examination 3 months after the end of the treatment found that residual tumor was significantly associated with decreased progression free survival.23 Metabolic responses on serial PET performed during chemoradiation, and at 4 and 8 weeks after the end of treatment, have been associated with complete response and survival in patients with cervical cancer.24
Tumor reduction rates <60% after external beam radiotherapy with chemotherapy on MRI can help to identify patients at higher risk of local and distant recurrence, suggesting a potential interest of optimized local treatment, such as completion surgery.25 26 Another strategy would be to offer such patients adjuvant chemotherapy, as is often done in high risk patients, such as those with para-aortic lymph node involvement.27 Moreover, closer follow-up might also be offered in order to detect early recurrences. However, current clinical practice cannot be modified based on retrospective studies and further prospective trials are needed to evaluate these strategies. Until then, our results will only permit us to give prognosis outcome counseling to our patients.
The main strength of our study was the long follow-up time. However, we do recognize a number of limitations, including its retrospective design and the heterogeneity of the treatment after external beam radiotherapy, particularly with some patients undergoing a surgical procedure. In addition, the size of the poor responder group was too small to evaluate if different treatment modalities had an influence on prognostic outcome.
In summary, we found that tumor size and its reduction rate after 45 Gy external beam radiotherapy and chemotherapy were associated with better survival. A tumor size reduction rate >60% after 45 Gy external beam radiotherapy MRI was significantly associated with improved disease free and overall survival. Therefore, identifying a subgroup of poor responders with a higher risk of local and distant recurrence may help to modify treatment recommendations after initial combination of chemotherapy and radiation.
References
Footnotes
Contributors Conceptualization: MAA, PB, EL, GF, AD, CM-G, DQ, and AM. Methodology: MAA, PB, EL, AL, GF, AD, CM-G, DQ, and AM. Software, validation, and formal analysis: AL. Investigation: MAA, PB, EL, AL, GF, AD, CM-G, DQ, and AM. Resources: AL, DQ, and AM. Data curation: MAA, PB, and AL. Writing - original draft: MAA and PB. Writing - review and editing: EL, GF, AD, CM-G, DQ, and AM.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Ethics approval Institutional review board approval was obtained from both participating centers.
Provenance and peer review Not commissioned; externally peer reviewed.