Article Text

Abstract
The diagnosis of cancer during pregnancy imposes a medical-ethical dilemma in weighing the risks of both mother and child. Increasing awareness of the feasibility of chemotherapy during pregnancy results in more pregnant patients receiving treatment for cancer. Information on obstetric and pediatric outcome of these high-risk pregnancies is greatly needed to guide physicians in patient counseling. In this review we present reported evidence for the incidence, diagnostic options, therapeutic management, obstetric risks, and neonatal outcome when cancer treatment is initiated during pregnancy. Decision-making when a cancer is diagnosed in a pregnant patient should be multidisciplinary, always taking the patient’s perspective into account. Cancer treatment during pregnancy is associated with low birth weight and preterm delivery, therefore frequent obstetric follow-up during oncological treatment in a specialized center is mandatory. Short-term clinical, cardiac, and cognitive outcome of children pre-natally exposed to cancer treatment is overall reassuring. Long-term follow-up of children is warranted to define the possible effect of pre-natal cancer treatment on general health, fertility outcome, and the risk of secondary cancers.
- malignancy
- pregnancy
- cancer treatment
- neonatal outcome
- pediatric outcome
Statistics from Altmetric.com
Introduction
A diagnosis of cancer during pregnancy imposes a medical-ethical dilemma as immediate aggressive treatment is often indispensable for maternal survival, whereas cytotoxic medication threatens fetal well-being by crossing the placenta.1 2 Owing to their mechanisms of action, all chemotherapeutic agents are potentially toxic to the developing fetus and thus maternal advantage must be always weighed against the possible risks for the unborn child.
In clinical decision-making all possible treatments should be discussed by a multidisciplinary team. In the past, termination of pregnancy was often the preferred advice because of the fear for adverse effects of cytotoxic drugs on the fetus. Termination of pregnancy still remains the preferred option when cancer is diagnosed before fetal viability with a very poor maternal prognosis or when the maternal disease requires treatment that is not compatible with continuation of pregnancy. However, in most cases, termination of pregnancy does not improve maternal prognosis and for socioeconomic religious reasons may not be an option for a particular patient.3 Also, the pregnancy may be the last chance of childbearing, as oncological treatment may affect fertility.
Increasing awareness of the feasibility of cancer treatment during pregnancy, has resulted in a change in management, with more pregnant patients receiving cytotoxic drugs.4 Although administration of chemotherapy after the first trimester is considered to be relatively safe, it is of vital importance to ensure fetal well-being. Some of these agents potentially have neurotoxic and cardiotoxic effects on the fetus. Use of chemotherapy after the first trimester may be associated with intra-uterine growth restriction, stillbirth, (iatrogenic) premature delivery, low birth weight, and neonatal myelosuppression and sepsis.5 6 It is highly important to consider the feasibility and safety of oncological treatment during pregnancy in order to inform patients about the possible risks for both mother and child.
In this review we give an overview of the current knowledge on the oncologic management and the obstetric, neonatal, and pediatric risks of cancer treatment during pregnancy.
Methods
First, we give an update on current knowledge of the epidemiology, diagnosis, and management of cancer during pregnancy. In order to summarize the reported obstetric and neonatal risks associated with an oncological diagnosis and treatment during pregnancy, we searched PubMed on July 20, 2018, for articles on cohorts of patients with cancer during pregnancy that described obstetric, neonatal, and pediatric outcomes. We used the following keywords: 'pregnancy', 'cancer', 'tumor', 'neoplasm', 'obstetric outcome', 'neonatal outcome', and 'pediatric outcome'. The search was restricted to publications in English, cohorts of at least 50 cases, and articles published between January 1, 1992 and June 31, 2018. As available evidence is limited and the first important publication of fetal outcome after cancer during pregnancy was published by Zemlickis in 1992, we chose to use this broad time frame.7 References from the selected articles were scanned in order to identify other papers. In the search for the long-term outcome of children pre-natally exposed to cancer or cancer treatment there was no restriction of the year of publication or number of included cases. In total, 25 large cohort studies and 10 population-based studies that reported obstetric and/or neonatal outcome after a cancer diagnosis during pregnancy were selected. Pediatric outcome was reported in 10 cohort studies.
Epidemiology of cancer during pregnancy
Pregnancies complicated by a cancer diagnosis are poorly studied epidemiologically as national registries usually do not combine information on both cancer diagnosis and obstetrics and most population-based studies focus on pregnancy-associated cancer, defined as a cancer diagnosis during pregnancy or within 12 months from delivery. Nationwide linkage studies estimated the incidence of pregnancy-associated cancer, to be approximately one in 1000 to 2000 pregnancies.8–10 As women in developed countries tend to delay childbearing, this rare combination is expected to become more common, as already demonstrated by population-based cohort studies. The incidence rate of pregnancy-associated cancer in Australia increased from 112.3 to 191.5 per 100 000 maternities between 1994 and 2007.9 In that continent, the incidence of pregnancy-associated melanoma rose from 37.1 per 100 000 maternities in 1994 to 51.84 per 100 000 maternities in 2008.11 A Canadian study found an increasing incidence of pregnancy-associated non-Hodgkin's lymphoma from 4.44 per 100 000 births to 7.17 per 100 000 births over the 9-year study period.12 Improved diagnostic procedures and more specialized interaction between health services during pregnancy might also have contributed to the higher incidence rates. Between 2003 and 2011 ovarian masses were increasingly detected in Canadian patients, probably owing to the recommendation of routine pre-natal ultrasound, whereas malignant masses remained relatively stable throughout the study period.13
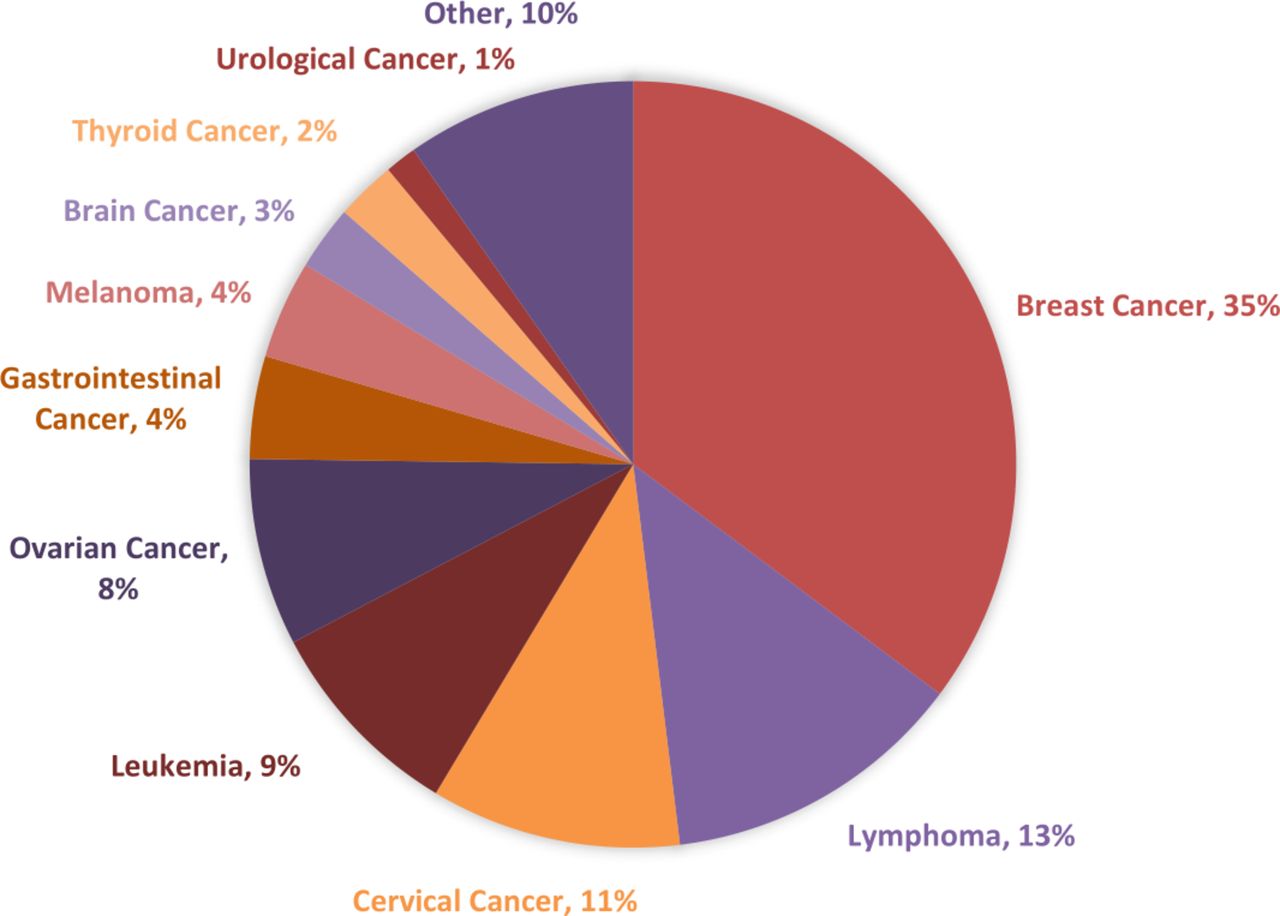
Large cohort studies that exclusively focus on patients with a cancer diagnosis during pregnancy are rare. In 2005 the International Network on Cancer, Infertility, and Pregnancy (INCIP) started a registry of cancer in pregnancy. The first update on the obstetric and neonatal outcome of 215 patients was published in 2010.14 An interim analysis on 1170 patients, the largest cohort study published to date, was performed in 2017.4 The research network continues to recruit patients with a cancer diagnosis in association with pregnancy, and a current update of the registry is shown in Figure 1. The most common cancers diagnosed during pregnancy were breast cancer (35%), lymphoma (13%), cervical cancer (11%), leukemia (9%), and ovarian cancer (8%). This distribution of diagnoses of various cancer types in association with pregnancy is similar to that seen in the non-pregnant population and is geographically defined.9 Melanoma is underreported in the registry as these patients are often not referred to tertiary centers for treatment in early stage. Older maternal age, high socioeconomic status, multiparity, multiple pregnancy, and prior diagnosis of cancer are retained as risks factors for an oncological diagnosis during pregnancy.9 10 15
{kind=link}
Distribution of cancer types diagnosed during pregnancy (N=1732, August 2018). Data retrieved from the cancer in pregnancy registry (August, 2018) by the International Network on Cancer, Infertility, and Pregnancy.
Diagnosis of cancer during pregnancy
Pregnancy-induced physiological changes may challenge the diagnosis of several cancers. It is estimated that a pregnant patient has a 2.5-fold higher risk of being diagnosed with locally advanced breast cancer than a non-pregnant patient, as physiological changes of the breast during pregnancy may delay diagnosis.16 A systematic physical examination and a low threshold for further investigations is crucial for an early diagnosis. The most optimal imaging is required to decide on further treatment and follow-up of the patient. When deciding on radiographic imaging in pregnancy, one should consider that only those examinations that will influence the management should be performed and caution is warranted since the (accumulated) fetal radiation exposure must not exceed 100 mGy and ideally, should be <50 mGy.17 Therefore, MRI and ultrasound are the preferred staging examinations during pregnancy. Diffusion-weighted MRI of the whole body is validated for the staging of cancer during all trimesters of pregnancy.18 Ultrasound can be performed safely during pregnancy. In breast cancer a mammography (restricted to one medio-lateral oblique record of both breasts and with abdominal protection in the second half of pregnancy) is advised. The sentinel-node procedure is considered to be sufficiently safe during pregnancy as the estimated average fetal radiation dose is 0.45 mGy. The injected dose of technetium-99m labeled colloid should be as low as possible and a 1-day protocol is preferred. Blue dye, which is sometimes injected before surgery to facilitate the detection of the sentinel node, is not advised as this may cause an anaphylactic reaction. Contrast products have to be used with caution in imaging. MRI of the breasts during pregnancy is not the preferred method, as gadolinium is contraindicated. Fetal gadolinium exposure is associated with rheumatologic, inflammatory, or infiltrative skin conditions, stillbirth, and neonatal death.19 Iodinated contrast may cause neonatal thyroid dysfunction. If it is used during pregnancy, the thyroid function of the neonate has to be controlled within 1 week after birth.
Treatment options during pregnancy
In the management of cancer during pregnancy the key principle is that the treatment stays as close as possible to standard treatment of non-pregnant patients. However, from the fetal perspective some treatments are not recommended or even contraindicated during pregnancy. If a pregnant patient presents with a very aggressive or metastatic disease in early pregnancy, it should be questioned whether the pregnancy can be continued safely. If a low-grade malignancy is detected, treatment postponement until after delivery may be considered. Preferably, decision-making should be performed in a specialized center by a multidisciplinary team, always taking the patient’s perspective into account.
Surgery
An intervention can be performed safely during the pregnancy, as long as some anesthetic and surgical adjustments are made. A stable oxygenation and blood pressure are mandatory to maintain an optimal fetal condition. In pregnancy the use of oxygen is raised and the functional residual capacity of oxygen reduced, resulting in a fast desaturation when apnea occurs. Maternal hypotension as a result of deep anesthesia, hypovolemia, and vena cava compression, may cause uterine hypoperfusion. Therefore, left lateral tilt position from 20 weeks gestational age onwards is advised. From a viable duration of pregnancy (usually 24 weeks of gestation, depending on local hospital policies and patient perspective) intraoperative fetal monitoring is advised whenever possible. Although data are limited, tocolytic medication may be considered if uterine manipulation during surgery is inevitable.20 A laparoscopic intervention during pregnancy can be performed until 26–28 weeks of gestation, depending on the surgeon’s expertise. An open introduction by Hasson is the preferred method. The umbilical port should be located 3–4 cm above the uterine fundus, even if this location is supra-umbilical. CO2 insufflation of 10–15 mm Hg can be safely used and maximal duration of the intervention is ideally 90 min. Postoperative analgesia is important as pain may provoke preterm uterine contractions. Non-steroidal anti-inflammatory drugs are contraindicated in pregnancy because of the risk of preterm closure of the ductus arteriosus. In the post-operative setting, prevention of thromboembolism with low molecular weight heparin is indicated because of the hypercoagulable state of pregnancy and cancer.20
Chemotherapy
The ability of a drug to cross the placenta is defined by its physicochemical properties, such as lipid solubility, ionization constant, molecular weight and protein binding. Owing to their relatively low molecular weight, most cytotoxic drugs can cross the placenta. Studies on the transplacental passage of cytotoxic agents, including paclitaxel, carboplatin, doxorubicin, and epirubicin, showed that the placenta acts as a barrier and the exposed fetal concentration is substantially lower than the maternal concentration.1 2 21 Since cytotoxic drugs are usually administered in a multi-drug regimen, it is difficult to estimate the effect of each drug. The reported neonatal outcomes after pre-natal exposure to various chemotherapeutic agents were recently reviewed by Ngu et al.22 Based on published reviews and case series, the authors concluded that adverse neonatal outcome is related to the dosage, timing, and extent of exposure to cytotoxic drugs. The use of chemotherapy during the first trimester of pregnancy potentially disturbs organogenesis and might cause spontaneous miscarriage, fetal death, and congenital malformations.7 22 Starting from the second trimester of pregnancy, the administration of cytotoxic drugs is associated with intra-uterine growth restriction, low birth weight, stillbirth, prematurity and admission to a neonatal intensive care unit.4 22 The evidence on placental passage and neonatal risks for several types of chemotherapy most commonly used during pregnancy is summarized in Table 1. Physiological changes in pregnancy, such as the increased blood volume and increased renal clearance, lead to a decrease in peak plasma concentrations and area under the curve, as well as a raised distribution volume and elimination.23 Theoretically this finding may suggest that a standard treatment dose of cytotoxic agents, which is based on the actual body weight may be suboptimal. To date no studies justify a change in dosage and the prognosis of patients treated for cancer during pregnancy seems similar to that of non-pregnant patients.24 However, more studies including larger numbers of patients with follow-up data and pharmacokinetic data are needed.
Evidence on possible neonatal risks after pre-natal exposure to the most frequently used cytotoxic drugs starting from the second trimester of pregnancy
Targeted anti-cancer therapies and tamoxifen
Over the years, targeted therapy has developed and is now used in the treatment of several types of cancers. Mostly the effect of these drugs during pregnancy is not known and use of targeted therapy in pregnant patients is discouraged because of the limited experience. Use of these drugs may be associated with fetal anomalies as specific molecular changes in cancer development are targeted, which may also be mechanisms in fetal development. Large IgG molecules are actively transported in the placenta by receptor-mediated endocytosis, from the second trimester onwards. In 2015 a comprehensive review with advice on the possible use of various targeted agents during pregnancy was published.25 Most targeted agents are contraindicated during pregnancy as pre-clinical data suggest high neonatal risks. The use of interferon-α can be administered during pregnancy on strict indications. Table 2 gives a brief overview of evidence on neonatal risks when targeted therapy or tamoxifen is used during pregnancy.26–28
Evidence on possible neonatal risks after pre-natal exposure to targeted therapy and tamoxifen
Radiation therapy
Whether or not radiation therapy should be started in pregnancy is a dilemma and the potential risks and benefits should be extensively discussed with the pregnant patient and her partner. Fetal radiation exposure during radiation therapy is much higher than the exposure during diagnostic procedures. Pelvic irradiation, with direct effect on the fetus, should never intentionally be performed during pregnancy. For the upper body (ie, breast, brain) the total fetal exposure should always be calculated by a physicist using a phantom model. Radiation exposure during the early first trimester can cause congenital malformations with a threshold dose of 100-200 mGy.17 The central nervous system is sensitive to radiation during 8–25 weeks after conception and a dose of 100 mGy may result in a decreased IQ. Radiation doses of 1 Gy are associated with up to 40% risk of several mental retardation. In utero irradiation at all gestational ages may increase the risk of cancer during childhood (ie, leukemia and solid tumors). In clinical practice, radiation after breast-conserving therapy will usually be postponed until after delivery, to avoid the potential effects on the fetus.
Supportive therapy
Supportive medication in pregnant women should be given only if clinically indicated. During pregnancy anti-emetic agents like metoclopramide, cyclizine, and meclozine can be safely used.20 If the effect is insufficient, ondansetron (5-hydroxytriptamine antagonist), aprepitant (NK1 antagonist), and alizapride (dopamine antagonist) may be considered with care. Also, the safety of corticosteroids, growth factors (granulocyte colony-stimulating factor) and erythropoietins during pregnancy has not been adequately studied, requiring surveillance of the fetus. These drugs are, however, mandatory for high-dose schemes as used in some patients with breast cancer. The use of hydrocortisone and prednisolone is preferred over dexamethasone or betamethasone as they are extensively metabolized in the placenta and relatively little will be detected in the fetal compartment. Repeated administrations of betamethasone are associated with attention problems and cerebral palsy.20
Obstetric management and delivery
Decisions about the best management in pregnancy, including timing of delivery, should balance maternal and fetal risks. In obstetric management, continuous evaluation of maternal and fetal well-being is essential. Before chemotherapy exposure, fetal growth as well as fetal doppler assessment and cervical length should be measured. In this population, iatrogenic preterm delivery is not uncommon, as delivery will be mostly planned to optimize the timing of oncological treatment. However, prematurity is associated with neonatal mortality and morbidity in the short and long term.29 Therefore the tendency to avoid iatrogenic preterm delivery and start of treatment needs to be balanced against the neonatal risks. Ideally, delivery after 37 weeks of gestation should be intended. Delivery within 2–3 weeks after the last administration of cytotoxic drugs (depending on the regimen used) should be avoided to reduce the risk of myelosuppression and systemic infection. Therefore, a neonatal blood sample is recommended. A vaginal delivery should be aimed for, unless there is an obstetric or oncological contraindication. Cervical cancer is an absolute indication for cesarean section in order to avoid recurrences on the episiotomy scar or major bleeding.20 During cesarean section, corporeal uterine incision or a wall wound protective system may prevent tumor spilling and abdominal wound recurrences. In gynecological cancers a cesarean section can be performed simultaneously with surgical treatment. Although rare, the placenta should be sent for histological examination to detect possible placental metastasis, mostly seen in malignant melanoma, followed by leukemia and lymphoma.6
Obstetric, neonatal, and pediatric outcome of cancer treatment during pregnancy based on published cohort and population-based studies
Obstetric outcome
The rarity of cancer during pregnancy and the variety of different cancer types have limited assessment of obstetric outcome and maternal events. Most information on obstetric risks for patients with cancer comes from large population-based cohort studies, summarized in Table 3. However, several limitations of studies based on a linkage between cancer and birth registries should be acknowledged. These studies often focus on obstetric outcome of pregnancy-associated cancers, which also includes post-natal cancer diagnoses. Early pregnancy loss (miscarriage or termination of pregnancy) is often not registered in birth data, potentially leading to a slight underestimation of the incidence of pregnancy-associated cancer as well as an overestimation of the average gestational age at cancer diagnosis in population-based linkage studies. Often these studies lack information on treatment modalities during pregnancy, preventing adjustment for cancer treatment in analyses of adverse pregnancy outcomes. Obstetric outcome after breast cancer and hematologic malignancies during pregnancy have been better studied than less common cancer types diagnosed during pregnancy.
Reported obstetrical outcome and complications of cancer during pregnancy in the largest multicenter cohort study and population based cohort studies on ‘pregnancy-associated cancer’
The largest cohort study to date revealed a pregnancy result, based on 1089 singleton pregnancies with known obstetric outcome, as follows: 1% stillbirth, 2% miscarriage, 9% termination of pregnancy, and 88% live birth.4 The main reasons for termination were start of oncological treatment or poor maternal prognosis (77%), unwanted pregnancy (11%), and fetal anomalies (4%). Patients were mostly diagnosed during the second trimester of pregnancy (48%). In total, 429/1170 (37%) patients were treated with chemotherapy during pregnancy. Of the 969 ongoing singleton pregnancies, seven (1%) intrauterine fetal deaths and seven (1%) perinatal deaths were reported. Preterm premature rupture of membranes (PPROM) or preterm contractions (10%) were the most commonly reported obstetric complications among ongoing singleton pregnancies. Half of the deliveries were preterm (48%), of which 88% were iatrogenic for oncological or obstetric reasons and 12% were spontaneous (for those with available data).
A change in management over time, with more patients treated during pregnancy, resulting in more live births was observed. Every 5 years there was, on average, an increased likelihood of a live birth among singleton pregnancies (RR=1.04, 95% CI 1.01 to 1.06), a reduction in the risk of preterm live birth (0.93, 0.86 to 0.99), and a reduction in the risk of iatrogenic preterm live birth (0.91, 0.84 to 0.98). In line with the decrease in preterm deliveries, neonatal intensive care unit admissions decreased (RR 0.91, 95% CI 0.83 to 0.99) and PPROM or preterm contractions decreased (0.97, 0.80 to 1.18) every 5 years, whereas the risk of a birth small for gestational age increased (1.16,0.99 to 1.35).
The high incidence of iatrogenic preterm delivery in pregnancies complicated by cancer was reported in a previous series.8 9 14 Maternal deterioration, optimal timing of cancer treatment, or the need to start therapy that is not compatible with pregnancy may force early delivery. Also, the administration of chemotherapy is associated with PPROM or spontaneous preterm contractions and labor. This is attributed to chemotherapy-induced weakening of the amnion-chorion membrane or activation by maternal hypothalamic-pituitary-adrenal axis, provoking labor by the release of oxytocin.12 14 30 The cesarean section rate in patients with a cancer diagnosis during pregnancy appears to be higher than in the normal population.9 This is likely to reflect the standard management of certain types of cancer (eg, cervical cancer), but may also be attributed to the comfort of a planned, controlled delivery.
Neonatal outcome
Clear evidence exists for the risk of birth defects when chemotherapy is administered during the first trimester, the crucial timing of organogenesis, which occurs roughly 2–8 weeks after conception. In cohort studies where mothers started treatment in the second trimester of pregnancy, the incidence of congenital malformations was not increased.5 31 The first large observational study that reported on fetal safety when cancer was diagnosed during pregnancy evaluated the neonatal outcome of 116 children, of whom 106 were pre-natally exposed to chemotherapy.32 There was no difference in the congenital malformation rate (3.8%) of the children exposed to chemotherapy compared with the general population. Larger and more recent studies confirmed this, with no higher incidence of congenital malformations and equivalent rates compared with the general population after second and third trimester chemotherapy exposure.4 33 34 However, caution remains warranted as after organogenesis, the eyes, genitalia, the hematopoietic system, and central nervous system are still vulnerable to exposure.5
Results of cohort studies appear to be inconsistent with regard to the effect on birth weight, with some studies showing an increased risk of fetuses small for gestational age (SGA)14 35 and others finding no different results6 11 36 37 or even a higher incidence of large for gestational age fetuses.9 11 Variations in management during pregnancy, treatment modalities, and the type of cancer diagnosed in the studied populations probably explain this inconsistency. Based on the largest cohorts, antenatal cancer treatment is associated with low birth weight. In a study of Cardonick et al, eight children (6.9%) were SGA.32 No significant differences were found for gestational age at delivery or birth weight according to the treatment given during pregnancy. Another cohort study in 2017 assessed the neonatal outcome of 61 infants pre-natally exposed to chemotherapy.38 The overall rate of SGA was 32%, independent of whether or not chemotherapy was administered during pregnancy. The largest cohort study to date evaluated the outcome of 955 neonates born after a cancer diagnosis during pregnancy: 21% of the fetuses were born small for gestational age.4 Maternal age, cytotoxic agents, and type of malignant disease were defined as risk factors. Fetuses that were exposed to platinum-based chemotherapy during pregnancy were at highest risk of being SGA.
The exact etiology of SGA and stillbirth in pregnancies complicated with a cancer diagnosis needs further research. As some cytotoxic drugs have several toxic properties and cross the placenta, fetal growth may be directly affected. Similarly, it appears that stillbirth and preterm SGA are more strongly associated with maternal cancer diagnosed during the second trimester of pregnancy, which is more likely to be treated than cancers diagnosed in the other trimesters.14 Also chemotherapy may alter placental growth factors. Whole transcriptome sequencing and immunohistochemical analysis show an increase in oxidative DNA damage in chemotherapy-exposed placentas.39 However, cancer treatment might not be the only explanation for increased neonatal risks. Other factors related to cancer diagnosis, such as maternal nutrition, anemia, thrombosis, maternal age, and maternal (psychological) stress, might affect fetal growth. That cancer itself may adversely affect fetal growth is proved by the association between preterm SGA and cancer diagnosis within 3 months after delivery, as a likely incipient yet untreated cancer during pregnancy.40 41 Fortunately, it seems that these SGA children show compensatory growth in the first months after birth.29 33
Published reports are inconsistent for the association between cancer during pregnancy and neonatal death. Most population-based linkage studies found no increased risk.9 12 15 37 42 In contrast, a recent large Swedish nationwide cohort study concluded that a diagnosis of maternal cancer was associated with an increased risk of adverse neonatal outcomes, including preterm SGA birth, stillbirth, and neonatal mortality.40 Also, post-natal cancer diagnosis was found to be associated with preterm SGA and neonatal mortality, but not with stillbirth. Information on treatment modalities during or after pregnancy was lacking. The authors stated that the association between SGA and stillbirth is not surprising as they share etiological factors, including intrauterine malnourishment, and SGA itself is a major determinant of stillbirth, especially preterm stillbirth. To optimize the timing of oncological treatment or due to maternal deterioration, iatrogenic preterm delivery is common in pregnancies complicated by cancer. It is suggested that the increased risk of neonatal mortality among these pregnancies might be explained by the high incidence of pre-term birth, a leading cause of neonatal death.40
Furthermore, cancer during pregnancy seems to be associated with neonatal intensive care unit admission. In the most recent cohort study, 41% of neonates were admitted to an intensive care unit, and in 84% of cases this was related to prematurity.34 Admission was associated with exposure to taxanes and was more likely after a diagnosis of gastrointestinal or cervical cancer during pregnancy.
In a case series of 50 neonates pre-natally exposed to chemotherapy for acute leukemia in the last month of pregnancy, 33% were cytopenic at birth.43 Delivery should be avoided during the maternal nadir period to prevent myelosuppression and the additional risk of sepsis.5 Especially in preterm babies the results of the administration of chemotherapy shortly before delivery might not have been eliminated because of the limited ability of immature liver and kidney function to metabolize cytotoxic drugs. Delaying delivery for 2–3 weeks after chemotherapy allows for placental drug excretion.
Pediatric outcome
The long-term outcome of children exposed to maternal malignancy and its treatment for general health, cardiologic, cognitive, behavioral, and neurological development is still a concern since data on these long-term effects are scarce. Table 4 gives an overview of the published series on prenatal cancer exposed children.29 33 34 43–48
Published literature on outcome of children pre-natally exposed to cancer or cancer treatment
In adults and children, treatment with anthracyclines, is associated with short- and long-term cardiotoxic effects. Cardiologic assessment in 10 pregnant patients exposed to anthracycline showed no significant short-term effect on both maternal and fetal cardiac function.49 Cardiac function in 50 children pre-natally exposed to anthracyclines was not affected at the age of 1–18 years, compared with 50 age- and sex-matched controls.29 Electrocardiographic results disclosed no arrhythmia or conduction abnormalities, although a higher heart rate (median 109, range 61–152) was observed in the study group. During echocardiographic examination, no cardiac defects were identified and all cardiac dimensions were within the normal range. The ejection fraction, fractional shortening, and interventricular septum thickness were slightly decreased in the study children compared with the control children. Some of the heart-rate dependent diastolic variables were significantly different between the patient and control group. Mitral valve E velocity was lower, mitral valve A velocity was shorter, and isovolumetric relaxation time was shorter in the study group. However, all measurements were still within the normal range. A normal cardiac function was confirmed among 47 pre-natally exposed children at 36 months of age.33 Furthermore, the use of chemotherapy during pregnancy in 81 children with mean age of 17 years (range 9.3–29.5) show no clinical or echocardiogram evidence of late cardiac toxicity.47
As the central nervous system continues to develop after the first trimester and throughout pregnancy, chemotherapy administered in the second or third trimester of pregnancy may affect neurocognitive development. Cognitive problems may become more apparent with increasing age as tasks become more complex and challenging for a child’s cognitive abilities. In a study that followed up 84 children until an age of 18.7 years, a normal physical, neurological, and neurocognitive development was found.44 Another study on the long-term outcome of 70 children exposed to chemotherapy in utero with a median age of 22.3 months (range 16.8 months – 17.6 years) reported normal neurodevelopment.29 Remarkably, 29% of exposed children had an increased score for internalizing, externalizing, or total problems behaviors compared with the general population. In addition, 50 pregnant patients with breast cancer treated with 5-fluorouracil, doxorubicin, and cyclophosphamide completed a post-neonatal health questionnaire. Fetal exposure to 5-fluorouracil, doxorubicin, and cyclophosphamide was not associated with serious adverse events or short-term health concerns and cognitive abnormalities for offspring.34 The largest cohort study to date comprises 96 children exposed to chemotherapy after the first trimester with a median follow-up of 22 months.33 These children were compared with healthy controls, matched for gestational age at delivery and test age. The cognitive, cardiac, and general development of children who were exposed to chemotherapy did not differ significantly from the control group. These results suggest that chemotherapy had no clear adverse short-term effect on post-natal growth or on cognitive or cardiac function. In addition, this study found that preterm birth was an independent predictor of poorer cognitive outcome in both the study and control group.
Ototoxicity is a known complication of platinum-based chemotherapy, and cisplatin carries the greatest risk. Cisplatin has a low molecular weight and the potential to easily cross the placenta. Few cases of hearing loss after pre-natally exposure to cisplatin have been reported.50 Amant et al assessed auditory functioning in 21 children between 6 and 18 years who were exposed to platinum-based treatment during pregnancy. While 18 children showed no abnormalities, three children reported hearing loss. In reported cases, infection, the use of aminoglycosides, and neurodevelopmental problems in these children were possible confounding factors.29 This risk should be carefully weighed and follow-up examination of hearing after birth is recommended. Where possible, cisplatin should be replaced by carboplatin with a more favorable toxicity profile.
Other potential adverse effects of pre-natal exposure to chemotherapy and/or radiotherapy are malignant disease and subfertility or infertility in the children. In a group of 84 children exposed to chemotherapy, with a median follow-up of 18.7 years, no secondary malignancies were observed and 12 second-generation children were born.44 However, more studies, larger samples, and longer-term follow-up of children pre-natally exposed to cancer treatment are needed to delineate the safety on secondary cancers and fertility.
Conclusion
Increased awareness of the feasibility of cancer treatment during pregnancy results in more pregnant women receiving oncological treatment and more children pre-natally exposed to cytotoxic drugs. Acknowledgement of possible obstetric and neonatal risks in this population is of extreme importance, as cancer in pregnancy is related to maternal and fetal morbidity. A multidisciplinary approach and follow-up in an experienced center with a high-risk obstetric unit is therefore recommended. Overall, pre-natal exposure to maternal cancer and cytotoxic treatment does not appear to impair physical, cardiologic, cognitive, and neurological development. However iatrogenic pre-term delivery should be prevented when possible. Moreover, more thorough and longer follow-up is needed to delineate the safety of both the children and their mothers. In order to provide more long-term evidence, INCIP set up a multidisciplinary network to follow the development of children pre-natally exposed to cancer or cancer treatment until the age of 18 years and beyond. Specialists with a special interest in cancer and pregnancy are invited to participate in the worldwide registry of INCIP.
Acknowledgments
We are grateful to the Koningin Wilhelmina Fonds (K.W.F.), European Research Counsil (ERC), Stichting Tegen Kanker and Research Foundation-Flanders (F.W.O.). FA is senior clinical investigator of the F.W.O.
References
Footnotes
CM and MvG are joint first authors.
Competing interests None declared.
Provenance and peer review Not commissioned, externally peer reviewed.