Article Text

Abstract
Objective To determine the incidence of long term lymphadenectomy complications in primary surgery for endometrial cancer and to elucidate risk factors for these complications.
Methods A retrospective chart review was carried out for all patients with endometrial cancer managed at Parma University Hospital Unit of Gynecology and Obstetrics between 2010 and 2016. Inclusion criteria were surgical procedure including hysterectomy and lymphadenectomy (pelvic or pelvic and aortic). We identified patients with postoperative lymphocele and lower extremity lymphedema. Logistic regression analysis was used to identify predictive factors for postoperative complications.
Results Of the 249 patients tested, 198 underwent pelvic lymphadenectomy (79.5%), and 51 (20.5%) of those underwent both pelvic and para-aortic lymphadenectomy. Among the 249 patients, 92 (36.9 %) developed lymphedema while 43 (17.3%) developed lymphocele. Multivariate analysis showed that addition of para-artic lymphadenectomy was an independent predictor for both lymphedema (odds ratio (OR) 2.764, 95% confidence interval (CI) 1.023 to 7.470) and lymphocele (OR 5.066, 95% CI 1.605 to 15.989). Moreover, postoperative adjuvant radiotherapy (OR 2.733, 95% CI 1.149 to 6.505) and identification of any positive lymph node (OR 19.391, 95% CI 1.486 to 253.0) were significantly correlated with lymphedema, while removal of circumflex iliac nodes (OR 8.596, 95% CI 1.144 to 65.591) was associated with lymphoceles occurrence.
Conclusion Although sentinel lymph node navigation is a promising option, lymphadenectomy represents the primary treatment in many patients with endometrial cancer. However, comprehensive nodal dissection remains associated with a high rate of long term complications, such as lymphedema and lymphocele. Avoiding risk factors that are related to the development of these postoperative complications is often difficult and, therefore, the strategy to assess lymph nodal status in these women must be tailored to obtain the maximum results in terms of oncological and functional outcome.
- endometrial cancer
- lymphadenectomy
- lymphocele
- lymphedema
Statistics from Altmetric.com
Extent of lymphadenectomy and aortic nodes removal are associated to lymphedema and lymphocele
Adjuvant radiotherapy and identification of any positive lymph node are related to lymphedema
Removal of circumflex iliac nodes is associated to lymphoceles occurrence
Introduction
Endometrial cancer is the most common gynecological malignancy in developed countries. Even though two-thirds of cases are diagnosed at an early stage and potentially treated through surgery alone, a substantial improvement in patient survival has been achieved through the establishment of surgical staging criteria in endometrial cancer patients by the International Federation of Gynecology and Obstetrics in 1988.1 Comprehensive staging includes abdominal exploration, pelvic peritoneal cytology, hysterectomy with bilateral salpingo-oophorectomy, and pelvic lymphadenectomy with or without para-aortic lymphadenectomy.2 Surgical staging identifies patients who have uterine risk factors for on-site recurrence (large tumor size, deep myometrial invasion, lymph vascular space invasion, cervical extension, and positive peritoneal cytology), extra-uterine disease (lymph node metastasis) and who may benefit from an integrated approach that includes radiotherapy and/or chemotherapy.2 3
Although sentinel lymph node mapping has been used for surgical staging of women with low risk endometrial cancer, its role in high risk cases remains controversial.4 5 The extension of lymphadenectomy remains a topic of ongoing debate because a significant base of evidence suggests that it could increase the risk for intraoperative and postoperative complications, especially in patients who are elderly or affected by chronic diseases, such as obesity, diabetes mellitus, and coronary artery disease.6–8
An argument against pelvic and para-aortic lymphadenectomy is that the procedure can increase the risk for postoperative lymphocele and lower limb lymphedema.9
Lymphocele is a common postoperative affliction, which results from an obstruction of the lymphatic vessels that drain fluids from the removed lymph nodal stations. The incidence rate of lymphocele in patients with endometrial cancer ranges from 1% to 38%, and the clinical presentation is strikingly heterogeneous. While most cases are diagnosed within 3–8 weeks after lymphadenectomy, some may occur up to 1 year after surgery. In fact lymphoceles in most patients are clinically asymptomatic and diagnosed during routine postoperative examinations. An earlier diagnosis usually occurs for lymphoceles that compress adjacent structures, because they eventually elicit symptoms that can be divided into urological (dysuria, urinary frequency, urinary retention, and urine outflow obstruction), vascular, and visceral (bowel obstruction and organ displacement).10
Postoperative lower limb lymphedema is a chronic, progressive, incurable condition that is characterized by limb swelling and sensations of heaviness, tightness, and pain. Lower limb lymphedema typically occurs within the first 12 months after surgery and often becomes chronic with increasing degrees of severity and disability.9 11–15
The aim of this study was to retrospectively analyze the incidence of long term complications following lymphadenectomy in women who are surgically treated for endometrial cancer, specifically focusing on postoperative lower limb lymphedema and lymphocele, to assess their potential risk and protective factors and evaluate possible preventive strategies.
Methods
We retrieved clinical data for all patients with a previous diagnosis of untreated and biopsy proven endometrial cancer who were admitted to the Gynecologic Oncologic Unit of the University Hospital of Parma (Italy) between March 2010 and December 2016.
Informed consent was obtained from all patients. The ethics committee at each institution approved the data collection. The study protocol followed the recommendations of the Strengthening the Reporting of Observational Studies in Epidemiology statement. Institutional review board approval was not required because the study analyzed existing data.
Inclusion criteria were: age >18 years, final histological diagnosis of endometrial cancer (all histologic subtypes and stages), and primary surgical treatment included pelvic and/or para-aortic lymphadenectomy (laparoscopic and open surgical procedures). Exclusion criteria included: age <18 years, performance status >2 according to the Eastern Cooperative Oncology Group, preoperative radiation or neoadjuvant chemotherapy, coexisting second primary cancer, visible metastatic disease, and leg edema related to medical comorbidities, such as heart failure, renal failure, diabetes, and vascular disease. All surgical procedures were performed by the same surgeon (RB).
The decision to perform a lymphadenectomy and the extent of the lymphadenectomy was typically made by consideration of grade, invasion depth, tumor size, primary tumor location at the time of hysterectomy, and each patient’s medical comorbidities.
According to institutional follow-up guidelines, the first postoperative examination was performed 1 month after surgery and then every 4 months until 36 months after the operation. All examinations were performed by one of four gynecological oncologists at our institution and included: an assessment of the vascular system (lymphatics, veins, and arteries), skin and soft tissues in swollen body parts, palpation of lymph nodes, and measures of limb volume and periodic ultrasonographic evaluation of the pelvis and abdomen to allow for an early detection of lymphocele (GE Voluson E8 instruments in B-mode and power Doppler mode).
Identification of patients with postoperative lower limb lymphedema and/or lymphocele was obtained through a physical examination, and the extent of lymphedema was assessed using the International Society of Lymphology's staging system.
Stage I (reversible edema): noticeable pitting and visible edema without dermal fibrosis, which both subside with limb elevation.
Stage II (spontaneously irreversible edema): as in stage I, but limb elevation alone rarely reduces tissue swelling and pitting, and dermal fibrosis may be noticeable.
Stage III (lymphostatic elephantiasis): skin examinations identify extensive acanthosis, fat deposits, and warty overgrowths, and pitting may be absent.
Stage 0 (latent or preclinical stage): no evidence of swelling despite impaired lymphatic transport and most patients are asymptomatic with a feeling of limb heaviness occasionally reported.
All patients with lymphedema were treated with a manual lymphatic drainage exercise, and external compression devices.
All detected lesions were classified according to the terms and definitions of the International Ovarian Tumor Analysis system.16 A lymph cyst was defined as a uni-locular or multi-locular, oval or round, or hourglass shaped cystic structure with a thick wall and fluid content of varying echogenicity, which might contain thin septae and debris. For each identified symptomatic or asymptomatic lymphocele, the location (external iliac, common iliac, obturator fossa, or para-aortic), size in three-dimensions (craniocaudal, transverse, and anteroposterior), and sonographic findings were retrieved. As defined by the Common Terminology Criteria for Adverse Events 4.03 grading system, symptomatic lymphoceles (sonographically verified pelvic lymphoceles that required medical intervention because of localized pelvic pain, pelvic abscess, fever, and/or leg edema) were considered as grade ≥2.
Statistical Analysis
Continuous variables were expressed as mean±standard deviation. Categorical variables were reported as per cent values. The association of lymphedema and lymphocele with individual data was assessed using the χ2 test (with continuity correction). Demographic and surgical data were dichotomized as follows: age <65 years versus ≥65 years, body mass index <30 kg/m2 versus ≥30 kg/m2, laparoscopy versus laparotomy,<15 resected lymph nodes versus >15, stage I versus stage >I, grading 1–2 versus grading 3, adenocarcinoma versus not adenocarcinoma, myometrial invasion <50% versus ≥50%, pelvic and para-aortic lymphadenectomy versus pelvic lymphadenectomy alone, any lymph node invasion versus no lymph node invasion, circumflex iliac nodes removed versus not removed, adjuvant chemotherapy versus no adjuvant chemotherapy, adjuvant radiotherapy versus no adjuvant radiotherapy, use of drainage versus no drainage, use of topical procoagulant versus no topical procoagulant, and disease related factors.
Multivariate odds ratios (OR) (and 95% confidence intervals (95% CI)) were calculated by linear regression analysis (SPSS 24, IBM Corp, Armonk, New York, USA) that was modeled to assess the relative influence of all factors associated with lymphocele by univariate analysis with a P value <0.200.
Results
A total of 249 patients met the inclusion criteria. The patients’ clinicopathologic characteristics are shown in Table 1. Mean age was 64.5±9.4 years. Mean patient’s body mass index was 28.3 kg/m2 and approximately 38.2% of patients were obese (body mass index ≥30 kg/m2). A total of 225 patients (90.4%) were in stage I, 0 (0%) were in stage II, 22 (8.8%) were in stage III, and 2 (0.8%) were in stage IV. One hundred and twenty-five patients (50.2%) had grade 1 endometrioid adenocarcinoma, 67 (26.9%) had grade 2, 57 (22.9%) had grade 3, 21 had uterine serous carcinoma, 12 had uterine clear cell carcinoma, 7 had mixed serous–endometrioid carcinoma, and 1 had carcinosarcoma. A total of 130 patients (52.2%) had myometrial invasion >50%. The mean follow-up period was 53.2±12.3 months (range 11–60). Postoperative lower limb lymphedema was reported in 92 patients (36.9%) and lymphocele was identified in 43 patients (17.3%).
Clinical background of 249 patients who underwent surgical treatment, including lymphadenectomy
Post-operative Lower Extremity Lymphedema
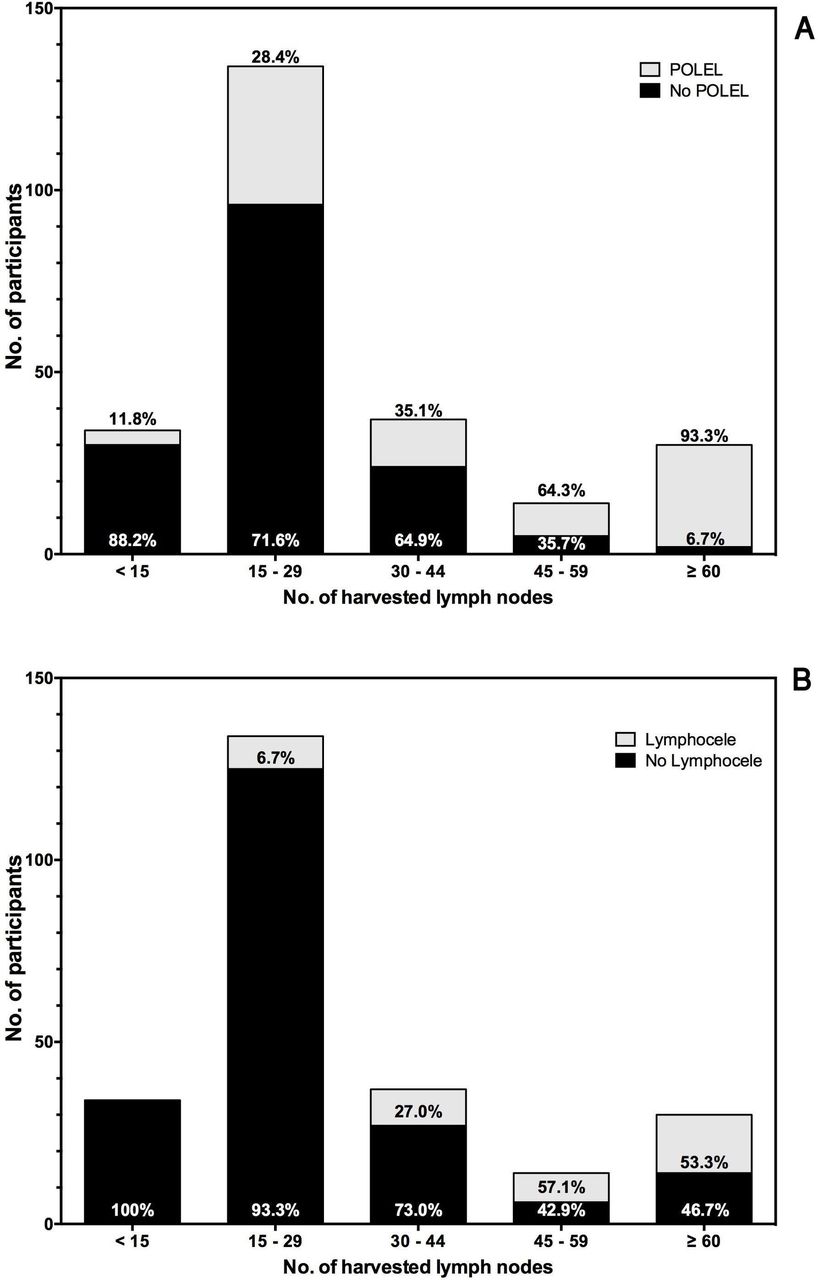
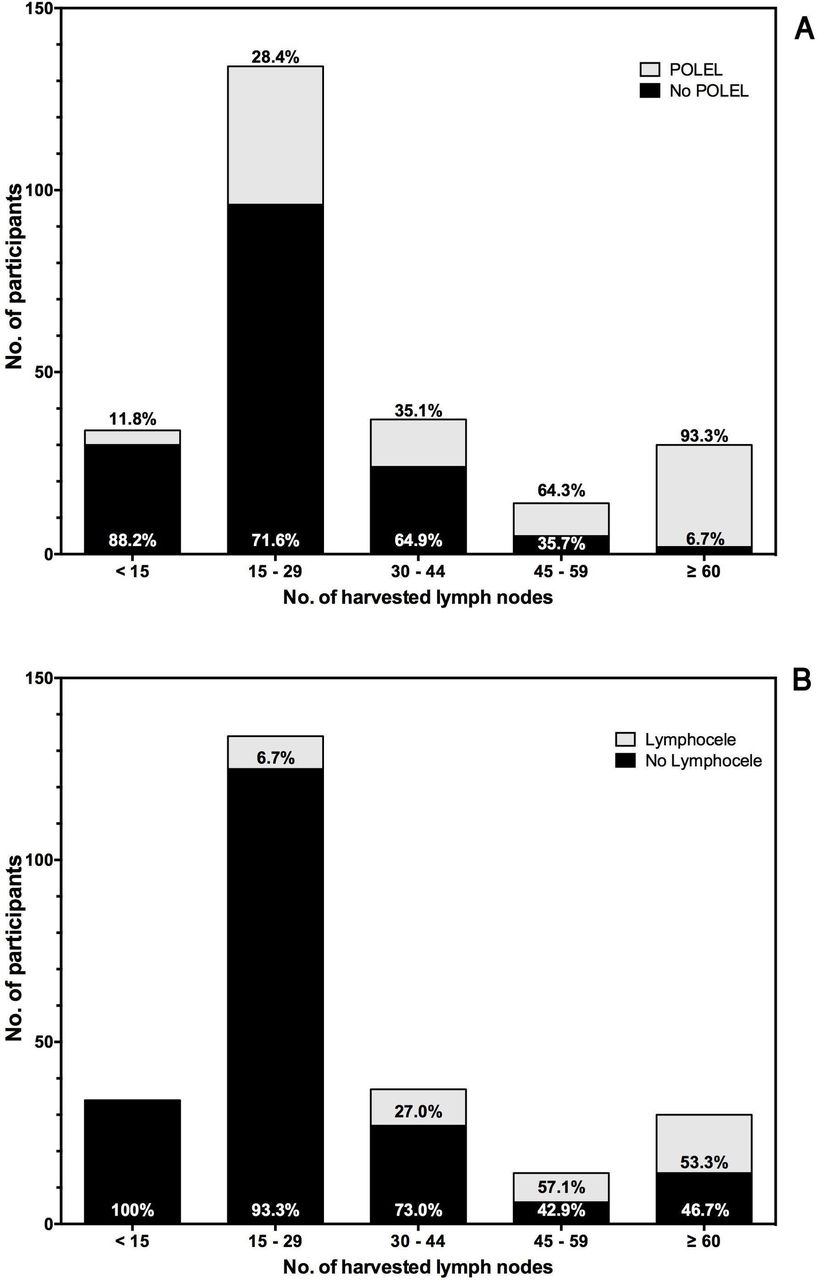
Univariate analysis showed that lower extremity lymphedema was significantly associated with a body mass index >30 kg/m2, presence of any comorbidity, stage ≥2, grading of G3, diagnosis of adenocarcinoma, myometrial invasion ≥50%, retrieval of pelvic and aortic lymph nodes ≥15, removal of circumflex iliac nodes, having received any topical procoagulant, and having been treated with adjuvant radiotherapy and chemotherapy, with all being included in a multivariate regression model (Table 2). The incidence of lymphedema significantly increased (χ2 test for trend P<0.001) as the number of harvested lymph nodes increased from 11.8% in patients with >15 harvested lymph nodes to 64.3% and 93.3% among patients who had received a larger lymphadenectomy (45–59 and ≥60 harvested lymph nodes, respectively) (Figure 1A).
Factors related to 92 cases of postoperative lower extremity lymphedema in 249 patients who underwent surgical treatment including lymphadenectomy.
{kind=link}
Distribution of postoperative lower extremity lymphedema (POLEL) (A) and lymphocele (B), by number of harvested lymph nodes among 249 women treated for endometrial cancer.
Multivariate analysis showed that only the addition of para-aortic lymphadenectomy (OR 2.764, 95% CI 1.023 to 7.470), identification of any positive lymph node (OR 19.391, 95% CI 1.486 to 253.0), and postoperative adjuvant radiotherapy (OR 2.733, 95% CI 1.149 to 6.505) were identified as significant predictors for postoperative lower limb lymphedema.
Lymphoceles
Thirty-three (76.7%) of 43 patients identified as having lymphoceles were asymptomatic; the remaining 10 patients (23.2%) were symptomatic (abdominal pain, hydroureteronephrosis, venous thrombosis, and sepsis). Most of the lymphoceles were localized in the pelvic region along the external iliac vessels (30/43 patients (71.4%)). Only one patient had a single lymphocele found in the para-aortic region (2.32%). The lymphoceles in four patients (9.3%) were diagnosed 3 months after surgery due to the occurrence of bacterial infections, and all of these patients required surgical treatment combined with antimicrobial therapies. All other patients (90.6%) were diagnosed 6 months after surgery.
Univariate analysis showed age ≥65 years, body mass index ≥30 kg/m2, stage ≥II, grading of G3, histological diagnosis of adenocarcinoma, myometrial invasion ≥50%, total number of harvested pelvic and aortic lymph nodes ≥15, having received para-aortic lymphadenectomy, identification of any positive lymph node among those harvested at surgery, removal of circumflex iliac nodes, application of any topical procoagulant, and having performed postoperative radiotherapy and chemotherapy were associated with lymphocele status (P<0.200), and all were included in the multivariate model (Table 3). A significant association between lymphocele and the number of harvested lymph nodes was identified (χ2 test for trend, P<0.001) (ie, a more extensive lymphadenectomy resulted in a higher incidence of lymphocele) (Figure 1B), peaking at 53.3% in patients with ≥60 harvested lymph nodes.
Factors related to lymphoceles in 43 patients among 249 women who underwent surgical treatment for endometrial cancer
Multivariate analysis showed previous comorbidity (OR 4.809, 95% CI 1.433 to 16.146), stage ≥II (OR 15.050, 95% CI 1.282 to 176.6), addition of para-aortic lymphadenectomy (OR 5.066, 95% CI 1.605 to 15.989), and removal of circumflex iliac nodes (OR 8.596, 95% CI 1.144 to 65.591) were identified as significant predictors of lymphocele.
Discussion
Lower extremity lymphedema and lymphocele are serious long term lymphadenectomy complications that negatively impact a patient’s quality of life,9–15 and the incidence rate in gynecological malignancies varies from 7.8% to 37.8%.10–13 This variance is due to the extent of lymphadenectomy, eventual application of the drain, techniques of coagulation in the lymphadenectomy area, and postoperative external beam radiation therapy.
In an analysis of the surgical complications associated with surgical staging in 128 patients, Orr et al determined the long term risk of lymphocele to be 1.3% and of lymphedema to be 0.7%, which are acceptable risks for a surgical procedure that can assist a physician with the quantification of a patient’s risk for recurrence.17 Todo et al performed a retrospective chart review that evaluated the risk factors associated with postoperative lower extremity lymphedema and found that 38% of patients undergoing exploratory laparotomy, total abdominal hysterectomy, bilateral adnexectomy, and pelvic and para-aortic lymphadenectomy experienced postoperative lymphedema, which was a higher percentage than that cited in other studies. Moreover, adjuvant pelvic radiotherapy, number of harvested lymph nodes, and removal of circumflex iliac nodes were identified as risk factors for the development of lower extremity lymphedema.12 18 Many studies have reported a great variety in the incidence rate of lymphocele, ranging from 9.4% to 48.5%.10 19–22
In the present study, we focused only on women with endometrial cancer. Although several previous studies reported a lower incidence of lower limb lymphedema and lymphocele, we found the occurrence to be 36.9% and 17.3%, respectively. A possible explanation for this discrepancy is the different radicality of the lymphadenectomy according to tumor type. We performed a systematic lymphadenectomy that removed a mean number of 24.0±8.5 nodes during pelvic and 6.2±13.1 nodes during para-aortic lymphadenectomies. Our results confirm that the extent of lymphadenectomy is significantly correlated with the risk of developing long term lymphatic complications.
Moreover, our data showed that the addition of para-aortic lymphadenectomy is an independent predictor of both lymphedema and lymphocele. Furthermore, identification of any positive lymph node and adjuvant pelvic radiotherapy are related to lymphedema while circumflex iliac node removal is associated with lymphoceles.
Lymphadenectomy in women with endometrial cancer should be considered only after evaluating the potential risks and benefits of the procedure. Potential risks include intraoperative and postoperative complications, such as lymphedema and lymphoceles, prolonged hospitalization, readmission, and increased cost. Several authors have underlined the potential benefits of lymphadenectomy.6 23–25 A study of the survival effect of para-aortic lymphadenectomy recently reported that a systematic lymphadenectomy, including para-aortic lymphadenectomy, has therapeutic significance for patients with an intermediate to high risk of endometrial cancer.7 That study showed that high risk patients who had a pelvic and para-aortic lymphadenectomy experienced longer overall survival than patients who had only pelvic lymphadenectomy (HR 0.53; 95% CI 0.38 to 0.76; P<0.001). The authors found that survival was not influenced by the performance of a para-aortic lymphadenectomy in the low risk group, but it was an independent prognostic factor in intermediate and high risk endometrial cancer patients (P<0.001).
The American College of Obstetrician and Gynecologists recommend that “retroperitoneal lymph node assessment is a critical component of surgical staging, because it is prognostic and facilitates targeted therapy to maximize survival and to minimize the effect of undertreatment and potential morbidity associated with overtreatment”. Nevertheless, a high variation in procedures in clinical practice reflect the lack of standardization of lymphadenectomy; the techniques vary from elective omission, to simple lymph node sampling, to systematic pelvic lymphadenectomy, with or without para-aortic lymphadenectomy.26 Despite the many decades of debates, there are still no convincing data that demonstrate a therapeutic role of lymphadenectomy in endometrial cancer.
Sentinel lymph node navigation is an accepted way to assess lymphatic spread in several solid tumors, including breast cancer, vulvar cancer, and melanoma, and is gaining ground in cervical cancer and endometrial cancer as a promising treatment for lowering the incidence rate of postoperative long term complications. This procedure has already been validated in low risk patients, but its role in women with high risk endometrial cancer is still under evaluation.27–33 Therefore, lymphadenectomy remains a primary treatment for patients with endometrial cancer.
The principal weaknesses of the present analysis are the retrospective and monocentric nature of the study, which cannot exclude reporting bias. However, the high rate of lymph nodes removed and the homogeneity of the surgical technique, which was performed by the same surgeon, are the principal strengths of our study.
Despite these limitations, we conclude that although sentinel lymph node navigation is a promising option, lymphadenectomy represents the primary treatment in many patients with endometrial cancer. However, comprehensive nodal dissection is associated with a high rate of long term complications, such as lymphedema and lymphocele. Avoiding risk factors that are related to the development of these postoperative complications is often difficult, and therefore the strategy to assess lymph nodal status in these women must be tailored to obtain the maximum results in terms of oncological and functional outcome. Future larger perspective studies are needed to confirm our promising findings.
References
Footnotes
LV and GS contributed equally.
Correction notice This article has been corrected since it was published Online First. An author name was corrected and an erroneous word was removed from the title.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Competing interests None declared.
Ethics approval The ethics committee at each institution approved the data collection for scientific purposes and institutional review board approval was not required because the study analyzed existing data.
Provenance and peer review Not commissioned, externally peer reviewed.