Article Text

Abstract
Background The efficacy of adjuvant radiotherapy in patients with intermediate risk early cervical cancer after radical hysterectomy is still under debate. Most guidelines recommend adjuvant radiotherapy, whereas others consider observation a viable option.
Objective To investigate if patients with intermediate risk factors for cervical cancer who underwent radical hysterectomy may benefit from adjuvant radiotherapy.
Methods Consecutive patients with tumor confined to the cervix and intermediate risk factors (according to Sedlis), treated between January 1982 and December 2014 who were observed after a type C2 radical hysterectomy formed the basis for this study. The frequency of recurrences, specifically isolated loco-regional recurrences, and the risk of death from recurrences, were analyzed. Data were analyzed using SPSS, version 23.0 for Windows
Results A total of 161 patients were included in the analysis. Median age was 40 (range 20–76). Stages IB1 and IB2 were seen in 87 (54%) and 74 patients (46%), respectively. Squamous cell and non-squamous histology was seen in 114 (70.8%) and 47 patients (29.2%), respectively. Of the 161 patients, 25 (15.5%) had recurrent disease, of whom nine had an isolated loco-regional recurrence (5.6%). Median time to recurrence for isolated loco-regional recurrences was 28 months (range 9–151). Treatment for an isolated loco-regional recurrence was radiotherapy (n = 4) and chemoradiotherapy (n = 5). Four patients (2.5%) died from disease as a result of an isolated loco-regional recurrence. Actuarial disease- specific survival was 93.0% for the total group. No variables were found that predicted an isolated loco-regional recurrence.
Discussion The mortality from isolated loco-regional recurrence in patients with intermediate risk factors for cervical cancer who underwent only radical hysterectomy type C2 was 2.5%. Further studies should compare outcomes between patients who undergo a type C2 radical hysterectomy without adjuvant radiotherapy with those undergoing a less radical hysterectomy but with adjuvant radiotherapy.
- cervical cancer
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: http://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
HIGHLIGHTS
Radical hysterectomy without radiotherapy resulted in 15.5% recurrences in patients with intermediate risk cervical cancer.
Only 2.5% of intermediate risk patients in our study died from isolated loco-regional recurrence after observation only.
Adjuvant radiotherapy may not improve survival in intermediate risk patients after a type C2 radical hysterectomy.
Introduction
Cervical cancer is the most commonly diagnosed cancer in countries with low resources and the leading cause of death from cancer in 42 countries, the vast majority of which are in sub-Saharan Africa and South Eastern Asia.1 2 Whereas in the developing world most cancers are diagnosed at a late stage, in the developed world early-stage diagnosis is more common.3 The choice of treatment in early-stage cancer depends mainly on the diameter of the tumor, WHO performance status, and on the preference of the treating physician and/or patient. There is a debate as to which patient will benefit from adjuvant radiotherapy after radical hysterectomy with tumor confined to the cervix but who have intermediate risk factors (large tumor size, lymph vascular space invasion, and deep stromal invasion).
Recently, a study was published on the role of adjuvant chemoradiotherapy in patients with surgically treated early cervical cancer and intermediate risk factors.4 The authors showed that there was no improvement in loco-regional control, disease specific, or overall, survival for patients treated with adjuvant chemoradiotherapy compared with a group of patients without adjuvant treatment. This was in contrast with Gynecologic Oncology Group (GOG) 92, a randomized controlled trial published in 1999, showing improved disease-free interval after adjuvant radiotherapy.5 In that same year, our group published data for a small series of 56 patients with intermediate risk factors treated by a type C2 radical hysterectomy without adjuvant radiotherapy.6 In that group, only one out of 56 patients died as a result of an isolated pelvic recurrence. We concluded that it was very unlikely that adjuvant radiotherapy for this group of patients would have resulted in better survival. Consequently, there was no reason for our group to change our treatment strategy This approach was confirmed when Rotman et al published the long-term follow-up of GOG 92, in which no overall survival benefit was found when giving adjuvant radiotherapy.7
In the most recent FIGO Committee Report a change from clinical staging to clinical/imaging/pathological based staging for cervical cancer was announced.8 In a previously published,9 FIGO Cancer Report 2018, treatment recommendations were also given. For intermediate risk patients with any two of three factors (tumor size >4 cm, presence of lymph vascular space invasion, and deep depth of invasion), adjuvant radiotherapy without chemotherapy was recommended. The objective of this retrospective study was to determine whether intermediate risk patients (treated with radical hysterectomy in a uniform manner in one institute without adjuvant radiotherapy) had no oncologic adverse outcomes when not undergoing adjuvant radiotherapy.
Methods
All consecutive patients who underwent a radical hysterectomy for early-stage cervical cancer between January 1982 and December 2014 in the Amsterdam University Medical Center (the Netherlands) were included in this study. Patients (n=31) referred from foreign countries were excluded, because an adequate follow-up was not feasible. Staging occurred according to the guidelines of the 1995 FIGO system. Patients with stage IB diagnosed before 1995 were retrospectively re-staged on the basis of the clinical tumor diameter of ≤4 cm (stage IB1) or >4 cm (stage IB2). Pathology specimens from 1982 to 1991, were previously reviewed by an expert gynecological pathologist,10 whereas specimens from 1991 to 2014 were analyzed prospectively by a gynecological pathologist and discussed by a multidisciplinary tumor board.
Only patients with squamous cell carcinoma, adenosquamous carcinoma, or adenocarcinoma were included. All patients were treated with an open radical hysterectomy and pelvic lymph node dissection according to Wertheim-Okabayashi.6 This type of surgery can be classified as a C2 radical hysterectomy according to the Querleu-Morrow Classification.11 This C2 resection aims at paracervix resection at the level of the internal iliac artery, uterosacral resection at the level of the rectum, sacrificing the autonomic plexus and removal of the vesico-uterine ligament at the level of the bladder. In the Okabayashi variant special attention is given also to a more radical removal of the posterior vesico-uterine ligament and removal of the pelvic nodal tissue dorsal from the obturator nerve.
During the study period the type of surgery and the radicality did not change. A subgroup of patients with negative lymph nodes, no parametrial invasion, and clear surgical margins (>1 mm), who did not receive adjuvant radiotherapy or chemotherapy were further analyzed. In this subgroup, patients with intermediate risk factors were selected based on criteria published by Sedlis et al5: a group with positive lymph vascular space invasion and deep one-third stromal invasion with tumor diameter of any size (Sedlis 1) or positive lymph vascular space invasion and middle one-third stromal invasion with tumor diameter of ≥2 cm (Sedlis 2) or positive lymph vascular space invasion and superficial one-third stromal invasion with a tumor diameter ≥5 cm (Sedlis 3), or negative lymph vascular space invasion and deep or middle one-third stromal invasion with a tumor diameter ≥4 cm (Sedlis 4). Depth of invasion was not always recorded in fractional one-thirds. Therefore, tumors with a depth of invasion ≥15 mm were classified as deep one-third stromal invasion, tumors with a depth of invasion between 10 mm and 15 mm as middle one-third stromal invasion, and all others as superficial one-third stromal invasion.
The following data were retrieved from the database, patient files, and pathology reports: age, FIGO stage, state of surgical margins, cell type, differentiation grade, clinical and pathological tumor size, presence of lymph vascular space invasion, depth of invasion, lymph node involvement, parametrial involvement, adjuvant treatment, and follow-up status. Survival status of patients was analyzed by matching our data with the National Cancer Registry. After treatment, patients were seen for follow-up every 3 months during the first year, every 6 months during the second/third year, and once yearly thereafter. Routine follow-up included history and physical examination. In cases of clinical suspicion of recurrent disease, diagnostic tests such as MRI or CT scan, serum tumor marker(s), and/or biopsies were performed. Recurrences were stratified as “local”, defined as a recurrence in the vagina or adjacent to the vagina in the central pelvis; “regional”, defined as a recurrence in the pelvis other than vaginal; and “distant”, defined as any recurrence outside the pelvis. Loco-regional recurrences were defined as either local or regional. Combined recurrences were defined as a combination of loco-regional recurrence and distant recurrence. Institutional review board approval was not obtained because according to Dutch law this is not necessary when anonymized patient data are used, keeping in mind the rules of good clinical practice.
All data were analyzed using SPSS, version 23.0 for Windows (SPSS Inc, Chicago, Illinois, USA). Patients were censored on August 2018, at the date of the last visit, or at the time of death not related to the cervical cancer. Outcomes were recurrence, localization of recurrence, time to recurrence defined as the interval between date of radical hysterectomy and date of recurrence, disease-free survival defined as the interval between date of radical hysterectomy and date of recurrence or last follow-up visit, disease-specific survival defined as the interval between the date of radical hysterectomy and date of death as a result of recurrent disease, and overall survival defined as the interval between the date of radical hysterectomy and death (irrespective of the cause of death) or last follow-up visit. Patients’ and disease characteristics were described using standard descriptive statistics—that is, medians/range for continuous data and frequencies/percentages for categorical data. Differences between groups were analyzed using Χ2 testing for categorical variables. Univariable survival curves were created using the Kaplan-Meier method. Comparison between groups was done using the log rank test. For all statistical tests, a two-tailed p value of <0.05 was considered significant.
Results
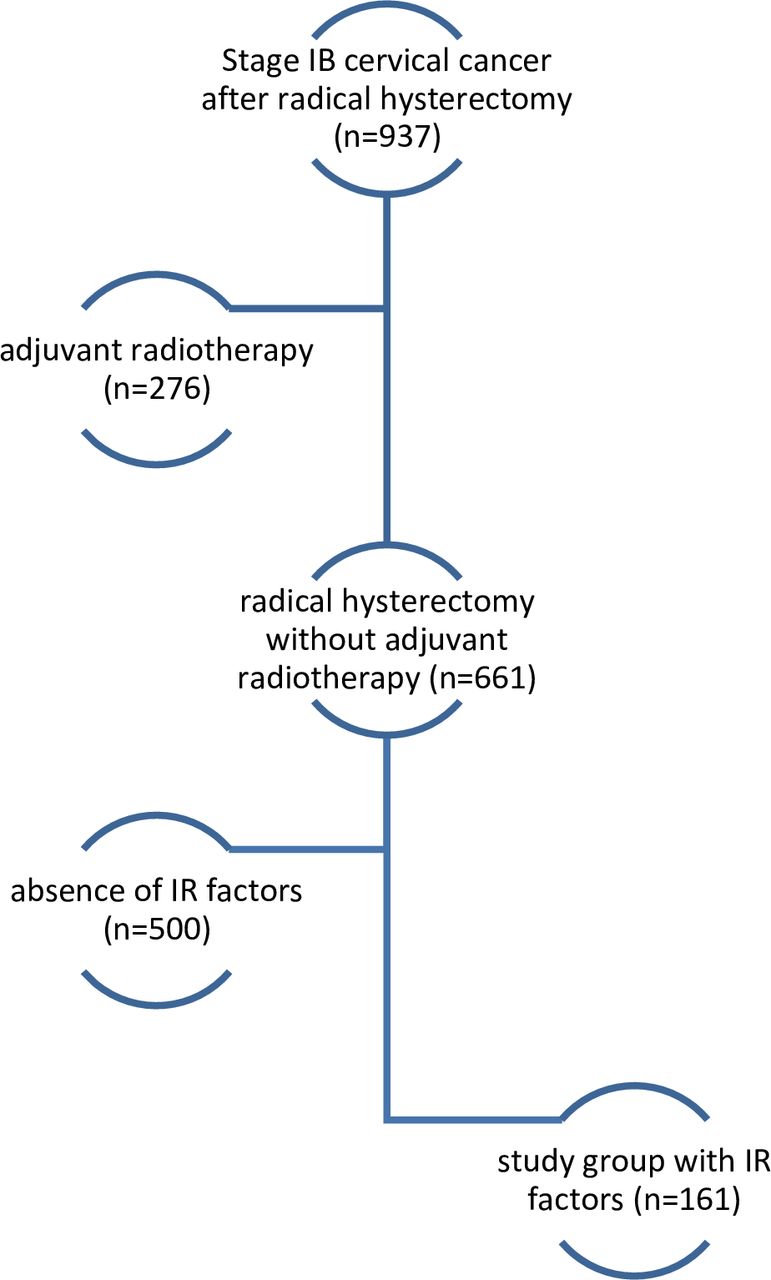
A total of 937 patients with stage IB1 and IB2 cervical cancer were treated with a radical hysterectomy. Patients who underwent adjuvant chemoradiotherapy (n=276) were excluded from further analysis. The reasons for adjuvant radiotherapy were a combination of positive lymph nodes and infiltration in the parametrium (n=75), positive lymph nodes (n=108), infiltration in the parametrium (n=64), non-radical or close (<1 mm) involvement of resection margins (n=24), extensive lymph vascular space invasion at a distance from the tumor front (n=1), and unknown reasons (n=4). Of the remaining 661 patients, 161 (24%) had intermediate risk factors (Figure 1). Results for 56 of the 161 patients with intermediate risk criteria have been published previously.6 The median follow-up of patients not dying from disease was 83 months (range 7–401). Clinical and pathological characteristics in relation to recurrence-free survival and disease-specific survival are shown in Table 1.
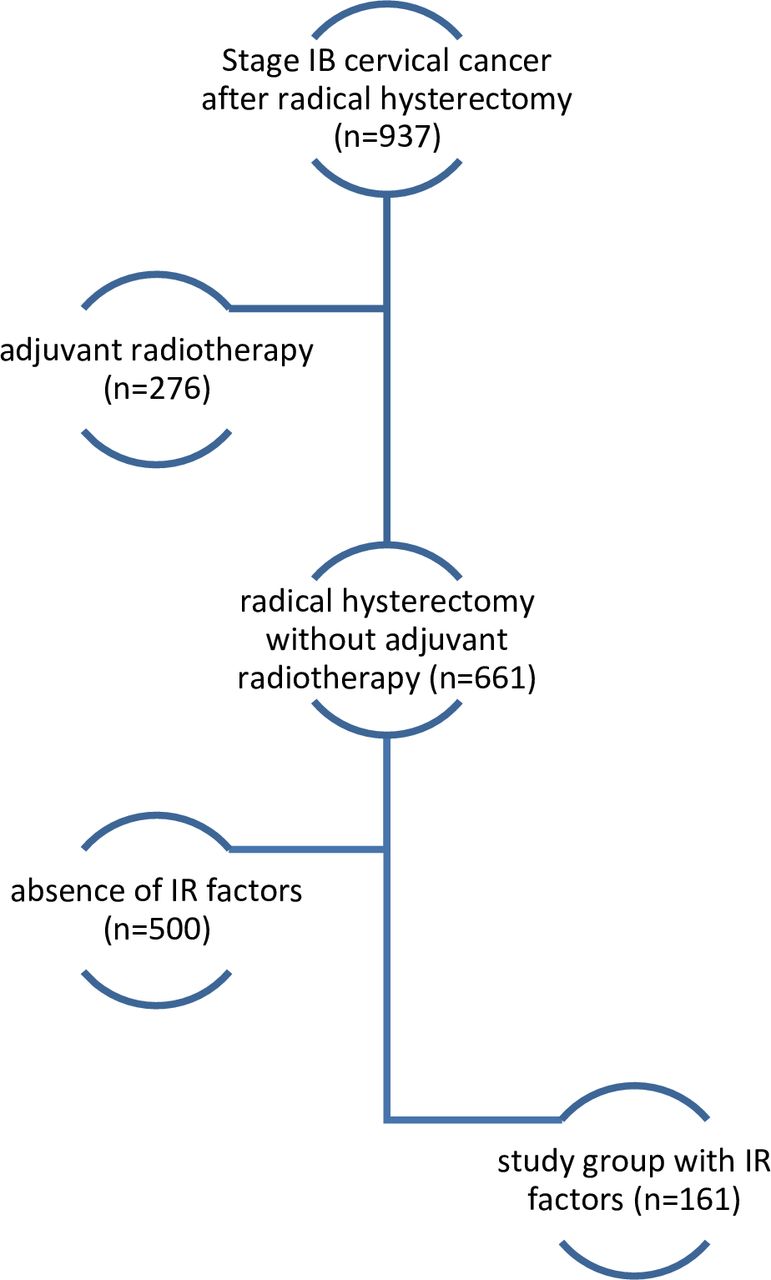
Flow diagram representing the selection of the study group with intermediate risk (IR) factors from the total group of patients with cervical cancer treated by a radical hysterectomy.
Univariate analysis of clinical and pathological factors of intermediate risk patients with cervical carcinoma associated with recurrence and disease-specific survival.
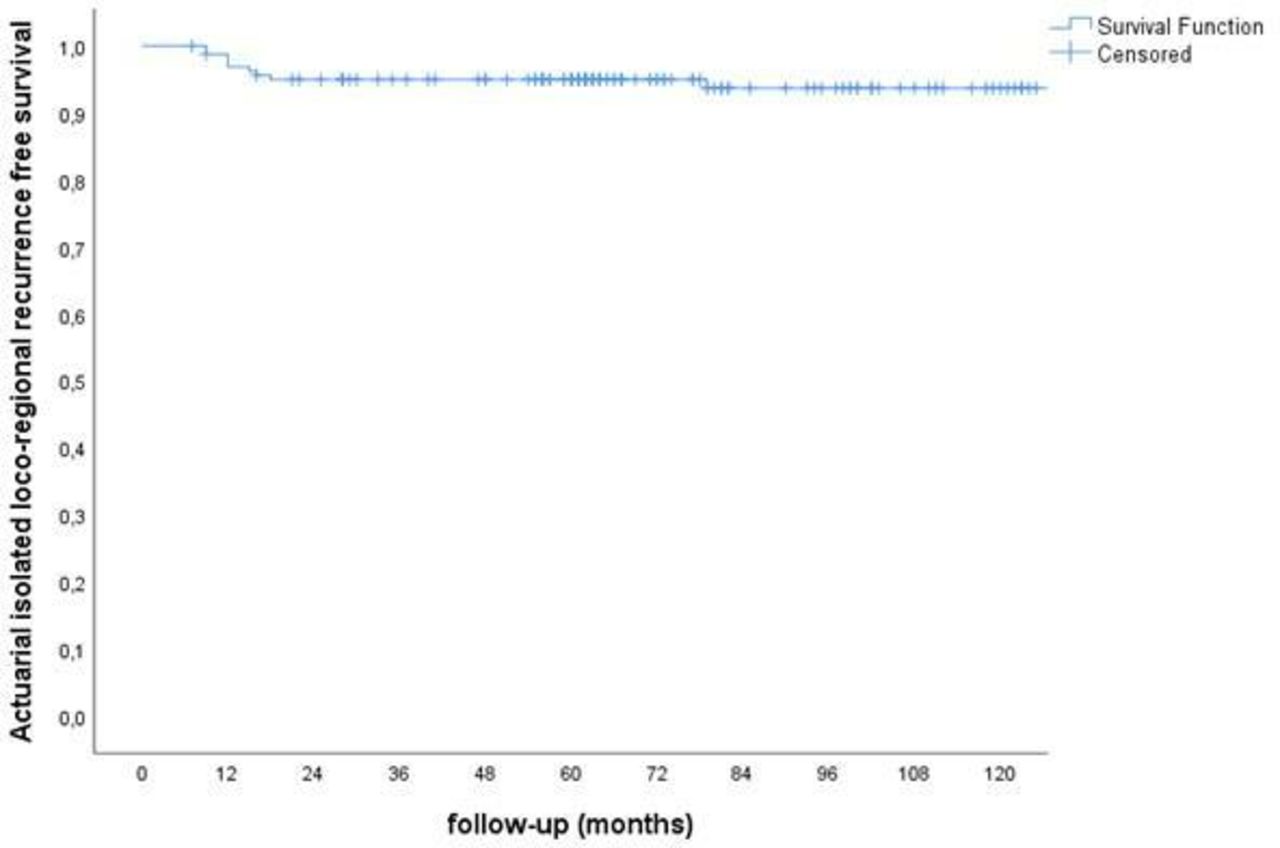
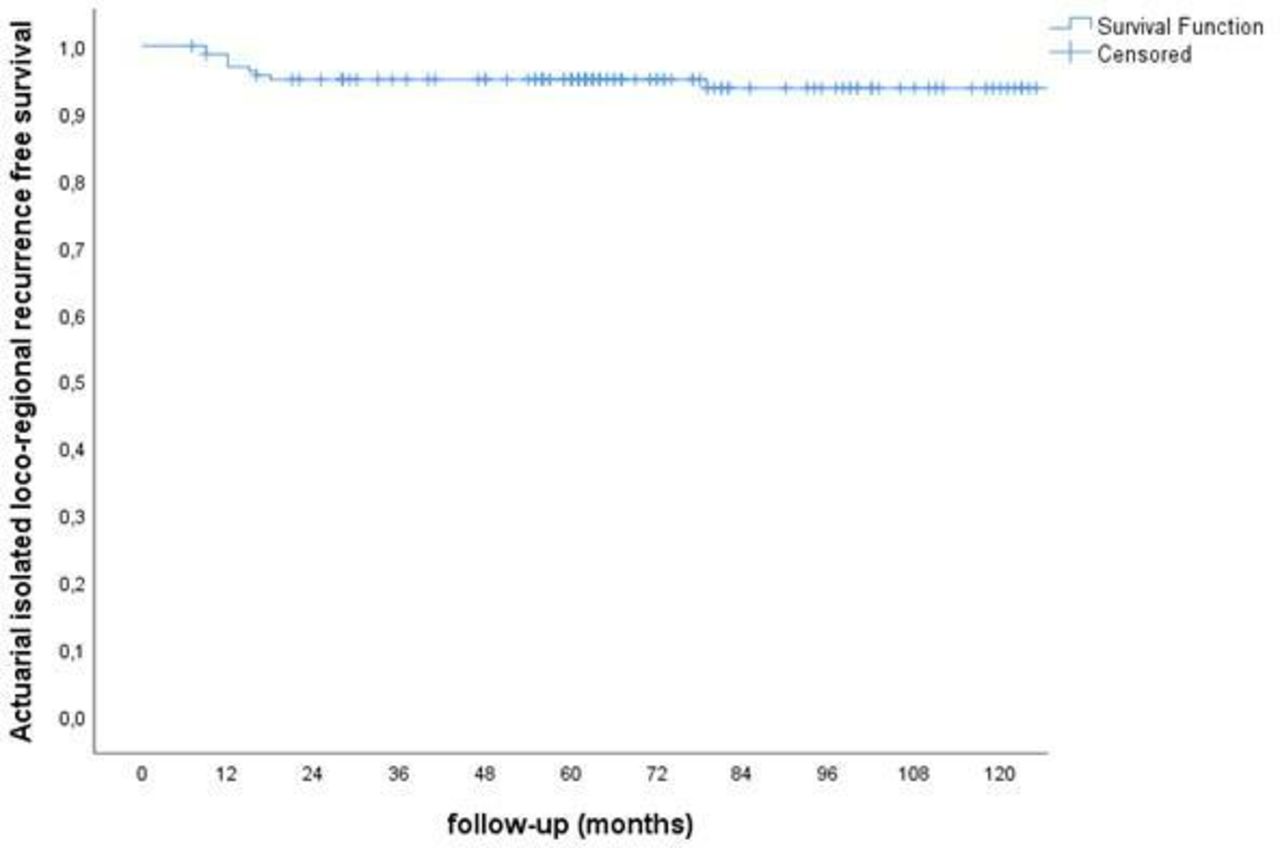
None of the analyzed variables were shown to be a significant predictor for recurrence or disease-specific survival. Recurrences were found in 25 (15.5%) of 161 patients. Recurrence frequency and pattern in relation to intermediate risk group according to Sedlis 1–4 is depicted in online supplementary Table 2). Actuarial recurrence-free survival at 2 and 5 years was 93.9% and 86.6%; respectively (online supplementary Figure 2). Seventeen patients died as a result of recurrent disease resulting in 2 and 5 years of actuarial disease-specific survival of 99.4% and 93.0%, respectively (online supplementary Figure 3). Actuarial overall survival at 2 and 5 years was 98.8% and 90.0%, respectively. Isolated loco-regional recurrences were found in 9 (5.6%) of 161 patients. Median time to recurrence for isolated loco-regional recurrences was 28 months (range 9–151). Isolated loco-regional recurrence-free survival at 2 and 5 years was 95% and 95%, respectively (Figure 2). From the total group, four patients (2.5%) with an isolated loco-regional recurrence died from disease (Table 2). Treatment for the patients with an isolated loco-regional recurrence was radiotherapy (n=4) and chemoradiotherapy (n=5). Five patients with an isolated loco-regional recurrence were initially salvaged by chemoradiotherapy. One of these latter patients had a second distant recurrence in the lung and is currently disease free 5 years after completing combination chemotherapy. The recurrence pattern for patients with squamous cell cancer and non-squamous cell cancer is shown in Table 3. The recurrence pattern was not significantly different for patients with non-squamous cell cancer vs squamous cell cancer (p=0.42). Of the patients with an isolated loco-regional recurrence 3 (2.6%) of 114 patients with squamous cell cancer and 1 (2.1%) of 47 patients with non-squamous cell cancer died as a result of the recurrent disease. The recurrence pattern was not different for patients with stage IB1 and IB2 (p=0.67) (online supplementary Table 5)
Supplemental material
{kind=link}
{kind=link}
Actuarial isolated loco-regional recurrence-free survival of 161 patients with early cervical cancer and intermediate risk factors treated by a radical hysterectomy without adjuvant radiotherapy.
Localization and frequency of recurrences and frequency of patients death from disease for the various recurrence localizations.
Recurrence pattern for patients with squamous cell carcinoma (SCC) and non-SCC histology (p=0.076).
Discussion
In this study 25 of 161 patients with stage IB cervical cancer and intermediate risk factors (15.5%) had a recurrence and nine of 161 (5.6%) had an isolated loco-regional recurrence after a type C2 radical hysterectomy without adjuvant radiotherapy. Four (2.5%) of 161 patients died from disease after developing a loco-regional recurrence. These results are in contrast with the randomized controlled trial (GOG 92) mentioned before, showing that patients with intermediate risk factors had a lower recurrence rate (15.3% vs 27.9%) and longer disease-free survival after adjuvant radiotherapy.5 A later publication in 2006, evaluating the follow-up results of this particular study did not show a significant difference in overall survival.7 However, on the basis of a longer disease-free survival, many national and international guidelines and9 FIGO Cancer Report 2018 recommend adjuvant radiotherapy for these patients.12–14 In the European Society of Gynecological Oncology (ESGO) guideline, the recommendation to give adjuvant radiotherapy is dependent on the type of hysterectomy. When, according to the ESGO guideline, an “adequate” radical hysterectomy is performed, observation is recommended as an option.13 Our results in this study confirm the low rate of intermediate risk patients dying from an isolated loco-regional recurrence after a type C2 radical hysterectomy without adjuvant radiotherapy as shown before in a subset of the current study population.6 Recently, other authors reached the same conclusion on the basis of a case–control study, showing isolated loco-regional recurrences in 1.6% vs 0% in the surgery only and adjuvant radiotherapy groups, respectively.4 Our results with 5.6% isolated loco-regional recurrences, compare unfavorably with the data published by Cibula and co-workers, showing 1.6% isolated loco-regional recurrences. This lower loco-regional recurrence rate might be due to the exclusion of patients with micrometastases identified after a sentinel lymph node procedure and by using imaging more frequently, resulting in exclusion of patients with extra-uterine disease. Also, only 12% of patients in the Cibula study had a tumor diameter ≥4 cm compared with a clinical tumor diameter ≥4 cm in 65% (105/161) of patients in our population, which might have contributed to their more favorable findings.4 In the follow-up of the original Sedlis study, published in 2006, it was concluded that adjuvant radiotherapy for an intermediate risk group could be particularly beneficial for patients with tumors with non-squamous histology, because in the radiotherapy arm they found that 3 (8.8%) of 34 patients had recurrences vs 11 (44%) of 25 patients in the surgery-only arm.7 In our population, a non-significant difference in recurrence rate (23.4% vs 12.3%, p=0.076) was found for patients with non-squamous vs squamous tumors. Isolated loco-regional recurrences for the squamous and non-squamous groups were observed in 6.4% and 5.3%, respectively, while 2.6% and 2.1%, respectively, died as a result of isolated loco-regional recurrences. Therefore, it is very unlikely that the subgroup of patients with non-squamous histology would have had a better survival if adjuvant radiotherapy had been given.
Other retrospective case series and case–control studies have been published advocating adjuvant radiotherapy for patients with intermediate risk factors.15–17 Unfortunately these studies were either small with only 17 patients in the surgery-only arm15 or showed a better recurrence-free survival without a difference in overall survival.16 17 One of the subjects that is not often considered in the studies discussed so far is the type or quality of surgery that was used. In the randomized GOG 92 study, quality control of the surgery consisted of review of the operation reports only.5 Therefore, inadequate surgery might have been the cause of the very high isolated loco-regional recurrence rate of 19.3% found in the surgery-only arm. This is in contrast with the data of the study of Cibula et al, where a type C2 radical hysterectomy was performed in tumors that were >4 cm in diameter, resulting in an isolated local recurrence rate of 1.6%.4 In a recent, large retrospective study, we have shown that radicality of surgery is an independent prognostic factor for recurrence and survival, especially in the group of patients with large tumors (>4 cm).18 Therefore, we hypothesize that also the relatively low isolated loco-regional recurrence rate of 5.6% in our study population is the result of more radical surgery. We admit that this type of radical surgery results in higher morbidity.19
Limitations of our study are the analyses of retrospective data over a period of 32 years. Modern imaging techniques such as MRI and PET/CT scanning have been introduced, resulting in a potentially different selection of patients for primary surgery compared with the first years of the study period. A strength of this study is the large homogeneous dataset of consecutive patients with long follow-up (median 83 months), where the status (alive or dead) of all patients was checked in the population registry. Furthermore, all patients had the same radicality of surgery. In the end the discussion will focus on the comparison of the morbidity of more radical surgery without adjuvant radiotherapy with less radical surgery followed by more adjuvant radiotherapy for patients in the intermediate risk group. This should preferably be tested in a prospective randomized study. It is our opinion that, as long as this debate has not been settled, the ESGO guideline13 should be followed for the indication for adjuvant radiotherapy after radical surgery for patients with a stage IB cervical cancer and intermediate risk factors.
Acknowledgments
The authors thank the registration team of the Netherlands Comprehensive Cancer Organization(IKNL) for the collection of data for the Netherlands Cancer Registry (NKR).
References
Footnotes
Correction notice This article has been corrected since it first published online. The open access licence type has been amended.
Contributors All authors contributed to the acquisition of the data, critically revised the manuscript, gave final approval for publication, and agree to be accountable for all aspects of the study. JvdV, CHM, and GF also analyzed and interpreted the data. JvdV was responsible for the conception and the design of the study.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data are available upon reasonable request.