Article Text

Abstract
Background The Laparoscopic Approach to Cervical Cancer (LACC) trial demonstrated a higher rate of disease recurrence and worse disease-free survival in patients who underwent minimally invasive radical hysterectomy.
Objectives To evaluate surgical and oncological outcome of laparoscopic radical hysterectomy performed at Hospital Italiano in Buenos Aires, Argentina.
Methods This retrospective study included all patients with cervical cancer, 2009 FIGO stage IA1, with lymphovascular invasion to IB1 (<4 cm) who underwent a laparoscopic radical hysterectomy between June 2010 and June 2015. Patients were eligible if they had squamous cell carcinoma, adenocarcinoma, or adenosquamous carcinoma, and no lymph node involvement by imaging. Patients must have undergone a type C1 radical hysterectomy. Only patients who were treated by a laparoscopic approach were included. Patients were excluded if histopathology showed a component of neuroendocrine carcinoma before or after surgery; if they had synchronous primary tumors, history of abdominal or pelvic radiotherapy, or were operated on at an outside institution; and if they had only surgery and no follow-up in our institution. Relapse rate and disease-free survival were evaluated using the Kaplan-Meier method.
Results A total of 108 patients were evaluated. The median age was 41 years (range 27–70). Distribution of histologic sub-types was squamous carcinoma in 77 patients (71%), adenocarcinoma in 27 patients (25%), and adenosquamous carcinoma in four patients (4%). Ninety-nine patients (92%) had stage IB1 tumors and 58 (54%) patients had tumors ≤2 cm. The median surgical time was 240 min (range 190–290), the median estimated blood loss was 140 mL (range 50–500) and the transfusion rate was 3.7%. The median length of hospital stay was 2 days (range 1–11). The median follow-up time was 39 months (range 11–83). The global recurrence rate after laparoscopic radical hysterectomy was 15% (16/108). According to tumor size, the recurrence rate was 12% in patients with tumors ≤2 cm (7/58) and 18% in patients with tumors >2 cm (9/50) (OR=0.76; 95% CI 0.26 to 2.22; p=0.62) The 3- and 5-year relapse rate was 17% (95% CI 11% to 27%). The 3- and 5-year disease-free survival was 81% (95% CI 71% to 88%) and 70% (95% CI 43% to 86%), respectively. Overall survival at 3 years was 87% (95% CI 76% to 93%).
Conclusion The recurrence rate after laparoscopic radical hysterectomy was 15%, and in tumors ≤2 cm it was 12%. The 3-year disease-free survival was 81%. Given these results our hospital has changed the approach to open radical hysterectomy.
- cervical cancer
- laparoscopy
- minimally invasive surgery
- radical hysterectomy
Statistics from Altmetric.com
Highlights
Recurrence rate after laparoscopic radical hysterectomy was 15%.
Recurrence rate in tumors ≤2 cm was 12%.
The 3-year disease-free survival rate after surgery was 81%.
Introduction
Radical hysterectomy with pelvic lymphadenectomy remains the standard recommendation for patients with cervical cancer, 2009 FIGO stage IA2 to IB1. The first case of a laparoscopic radical hysterectomy was reported by Nezhat et al in 1992.1 Since that time an increasing number of publications have documented the safety and feasibility of laparoscopic or robotic radical hysterectomy.2–4 Most publications have focused on the peri-operative outcomes of the minimally invasive approach with an emphasis on blood loss, transfusion rates, and post-operative return of bowel function and return to daily activities.
The retrospective data had shown that neither the laparoscopic nor the robotic approach were associated with lower 5-year rates of disease-free survival or overall survival in comparison with the open approach.5 6 A recent prospective randomized trial published by Ramirez et al in the New England Journal of Medicine compared open with minimally invasive radical hysterectomy in patients with early stage cervical cancer. The authors showed that the rate of disease-free survival at 4.5 years was 86% with minimally invasive radical hysterectomy and 96.5% with the open approach. Minimally invasive surgery was associated with lower rates of disease-free survival in comparison with the open approach (3-year rate, 91.2% vs 97.1%; HR for disease recurrence or death from cervical cancer, 3.74; 95% CI 1.63 to 8.58).7 In a cohort study involving women who underwent radical hysterectomy for stage IA2 or IB1 cervical cancer, published in the same edition of the New England Journal of Medicine, Melamed et al showed that minimally invasive radical hysterectomy was associated with a shorter overall survival than open surgery among women with 2009 FIGO stage IA2 or IB1 cervical carcinoma.8 In this same study, the authors showed hat the 4-year mortality was 9.1% among women who underwent minimally invasive surgery and 5.3% among those who underwent open surgery and that the adoption of minimally invasive surgery coincided with a decline in the 4-year relative survival rate of 0.8%. Given the results of these two studies, we aimed to evaluate the surgical and oncological outcomes at our own center pertaining to minimally invasive radical hysterectomy.
Methods
We conducted a retrospective cohort study to assess the surgical outcomes, recurrence rate, and disease-free survival at 3 years and 5 years in patients with early stage cervical cancer who underwent a laparoscopic radical hysterectomy at Hospital Italiano in Buenos Aires, Argentina.
This study was approved by the ethical investigation protocol committee of our hospital. The records of patients diagnosed with cervical cancer, between June 2010 to June 2015 in the gynecologic oncology department were reviewed.
Patients were eligible if they had a squamous cell carcinoma, adenocarcinoma, or adenosquamous carcinoma of the uterine cervix; had a disease 2009 FIGO stage IA1 (lymphovascular invasion), IA2, or IB1, and no lymph node involvement by imaging studies. Patients must have undergone a type C1 radical hysterectomy (Querleu-Morrow classification).9 Only patients who were treated by a laparoscopic approach were included. Patients were excluded if histopathology showed a component of neuroendocrine carcinoma before or after surgery; if they had synchronous primary tumors, a history of abdominal or pelvic radiotherapy, or were operated on at an outside institution; and if they had only surgery and had no follow-up in our institution.
All patients underwent a pre-treatment evaluation, including a physical examination, and CT or MRI scan. Primary surgery included a laparoscopic total radical hysterectomy with pelvic lymphadenectomy, with or without bilateral salpingo-oophorectomy. The procedure was performed using a four-port technique (a 10 mm optical port was placed in the umbilicus or 2 cm above, depending on uterine size, and three 5 mm ancillary trocars were placed in the lower abdominal quadrants). A VCare ConMed uterine manipulator was used in all cases.
The variables evaluated included the following: age, body mass index, imaging, follow-up period, histological type, depth of stromal invasion, number of lymph nodes resected, presence of lymphovascular invasion, tumor size (measured in millimeters by MRI), adjuvant treatment, time to relapse, site of recurrence, and disease status at last follow-up. The follow-up after treatment included visits every 4 months during the first 2 years, and then every 6 months from years 3 to 5. Once a year, a MRI scan was performed to evaluate pelvic or distant disease.
Statistical analyses were conducted using STATA version 13 software. Continuous variables with normal or skewed distribution were shown as mean (SD) or median (IQR), and compared by Student’s t-test or Mann-Whitney U test, respectively. Categorical variables were shown as number (percent), and compared by Χ2 test. Overall mortality and overall survival was evaluated using the Kaplan-Meier method. Two-tailed p values <0.05 were regarded as statistically significant.
Results
Of the 130 patients with 2009 FIGO stage IA–IB1 cervical cancer treated at our institution within the study period, only 108 met the inclusion criteria. Two patients were excluded because of neuroendocrine histology, four received neoadjuvant chemotherapy, and the remaining 16 patients only had surgery at our institution without follow-up.
The median age was 41 years (range 27–70), and the median body mass index at the time of the surgery was 28 kg/m2 (range 21–37) (table 1). A total of 102 patients (94%) underwent an abdominal and pelvic MRI scan before surgery, the remaining six patients had a pre-operative CT scan. A laparoscopic approach was completed in all patients, and no conversion to open abdominal approach was required. The median surgical time was 240 min (range 190–290) and the median estimated blood loss was 140 mL (range 50–500). The overall (intra-operative and post-operative) transfusion rate was 3.7%. The median number of lymph nodes resected was 20 (range 15–30). The median length of hospital stay was 2 days (range 1–11). Intra-operative complications included three patients (3%) who experienced a bladder injury that was managed laparoscopically. Five patients (4.6%) experienced post-operative grade 3A (Clavien-Dindo classification)10 or worse post-operative complications. The events included hemoperitoneum requiring laparoscopic surgery on the first post-operative day; a diagnosis of uretero-vaginal fistula requiring a laparoscopic ureteral re-implantation on day 13 after surgery; uroperitonitis due to an unidentified bladder injury; and two symptomatic lymphoceles requiring percutaneous drainage in one patient and a laparoscopic drainage after failed percutaneous drainage in the other. The median follow-up time was 39 months (range 11–83) (table 1). After surgery, 45 patients (42%) with adverse prognostic factors, such as positive nodes, microscopic parametrial involvement, or positive margin, and patients with two of three Sedlis criteria,11 received adjuvant concurrent chemoradiation therapy. Seventeen of the 108 patients (15.7%) had positive lymph nodes, the median tumor size of patients with positive nodes was 27 mm, whereas in patients with negative nodes the median tumor size was 18 mm (p=0.009).
Baseline characteristics of the patients
The global recurrence rate was 15% (16/108), with no significant difference in age (p=0.14), histologic sub-type (p=0.84), stage (p=0.62), node involvement (p=0.71), parametrial involvement (p=0.81), or presence of lymphovascular invasion (p=0.54), when comparing patients in whom the disease did and did not occur (table 2). According to tumor size, recurrence rate was 12% in patients with tumor size ≤2 cm (7/58) and 18% in patients with tumor size >2 cm (9/50) (OR=0.76; 95% CI 0.26 to 2.22; p=0.62).
Comparison of the main variables between patients who did and did not relapse.
Seven recurrences were located in the vagina and all had a tumor size <2 cm. Five patients had a recurrence in the pelvis, three of them were central, and two were pelvic side wall recurrences. Three patients had peritoneal carcinomatosis, and one a metastasis to the liver (table 3). The median time to recurrence was 12.6 months (range 7.1–19.5).
Patients who had recurrent carcinomatosis
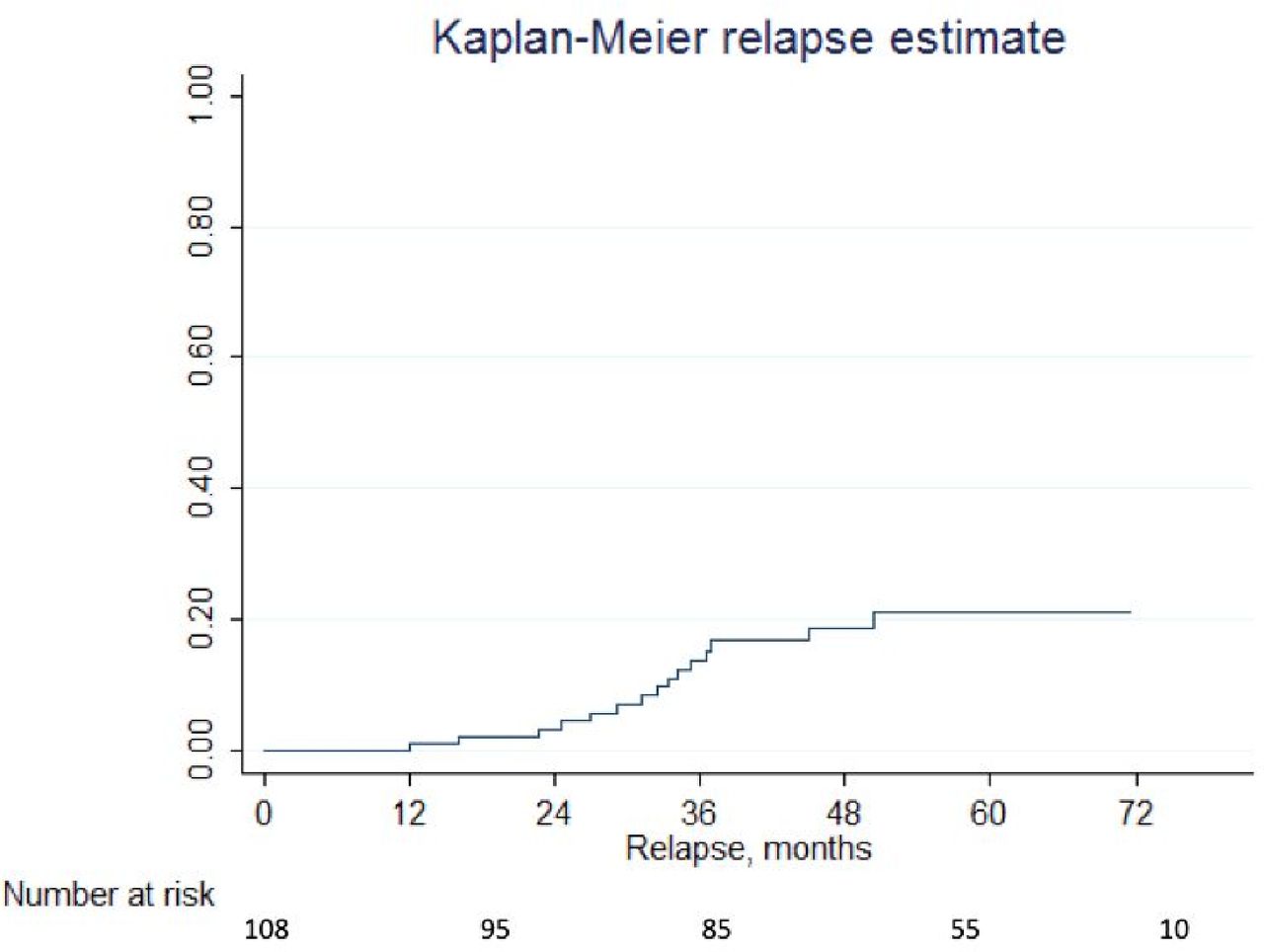
A total of 10 patients died during follow-up, eight patients died owing to disease progression, one patient had a myocardial infarction 13 months after surgery, and the other patient died of anaphylactic shock after a urological procedure not associated with her oncological disease. The Kaplan-Meier method estimated that the 3- and 5-year relapse rates were 17% (95% CI 8% to 24%) (figure 1). The 3- and 5-year disease-free survival was 81% (95% CI 71% to 88%) and 70% (95% CI 43% to 86%), respectively (figure 2).

Kaplan- Meier estimated 3-year relapse rate.

{kind=link}
{kind=link}
Kaplan- Meier estimated 5-year disease-free survival.
Discussion
This study evaluated the oncological results of 108 patients who received laparoscopic radical hysterectomy for early invasive cervical cancer. The recurrence rate was 15%, and the 3-year disease-free survival was 81% (95% CI 71% to 88%).
The use of a minimally invasive approach in the management of gynecological cancers has increased in recent decades, with the aim of improving the peri-operative results and the quality of life of patients undergoing radical hysterectomy. Many reports of comparative studies have shown better surgical results and equal oncological outcomes with both approaches.2–6
In a retrospective study Roh et al,4 compared the outcomes of patients treated by laparoscopic radical hysterectomy and patients treated by abdominal radical hysterectomy. The 5-year recurrence-free survival rate was 94.8% in the laparoscopic group and 96.8% in the abdominal group respectively (p=0.39).
Lee et al2 described a retrospective, matched case–control study of patients with stage I–II cervical cancer who underwent laparoscopic radical hysterectomy; the patients were matched with controls (ratio 1:2) who underwent radical abdominal hysterectomy. The median follow-up was 78 and 75 months, respectively, and there was no significant difference in the 5-year disease-free survival rate between the groups (90.5% and 93.3% for laparoscopic radical hysterectomy and radical abdominal hysterectomy, respectively; p=0.92).
These results were confirmed in two subsequent meta-analyses. Wang et al5 compared laparoscopic with laparotomy radical hysterectomy in 754 and 785 patients, respectively. They found no differences in overall survival (HR=0.91, 95% CI 0.48 to 1.71, p=0.76) or in disease-free survival (HR=0.97, 95% CI 0.56 to 1.68, p=0.91) between the two approaches. Similarly, in the meta-analysis by Cao et al,6 which included 2922 patients, there were no significant differences in the disease-free survival rate, overall survival rate, and recurrence rate between the two groups. Both meta-analyses have a short follow-up time in the minimally invasive surgery group.
Previously, we presented at the 2015 Society of Gynecologic Oncology annual meeting, a descriptive observational comparative study of 50 patients treated by laparoscopic radical hysterectomy and 31 patients treated by open radical hysterectomy. The groups were comparable in age, body mass index, tumor size, FIGO stage, and histological type. Our data showed a recurrence rate of 13.4% for laparoscopy versus 8.5% for laparotomy (p=0.77).12 The study design had limitations, including its retrospective nature, the use of a historical series of laparotomy surgeries, and differences in follow-up times where the median follow-up in the laparotomy group was 44 months (range 29–57) vs 14.5 months (range 7–25) for the minimally invasive group.
Ramirez et al7 recently published the results of the LACC trial and found that minimally invasive surgery was associated with a lower rate of disease-free survival and a lower rate of overall survival (3-year rate 93.8% vs 99.0%) than open surgery. In addition, the epidemiologic study conducted by Melamed et al8 reported that over a median follow-up of 45 months, the 4-year mortality was 9.1% among women who underwent minimally invasive surgery and 5.3% among those who underwent open surgery, and a decline in survival coinciding with the incorporation of the minimally invasive approach. The results of these studies challenged the previously published retrospective literature as it pertained to oncologic outcomes.
In our study, we also evaluated whether recurrence rates differed based on tumor size, recognizing that the number of patients in each group (≤2 cm vs >2 cm) was not adequately powered to provide a definitive answer. We found that seven recurrences (12%) occurred in patients with tumors ≤2 cms, and 9 (18%) in tumor sizes >2 cm. The recurrence rate is higher than that reported in the study by Ramirez and colleagues, which was 8.4%.
In addition, in our study we observed an unusual pattern of recurrence, since 19% of the patients presented a recurrence with carcinomatosis. This supports the possible role of peritoneal diffusion of neoplastic cells from the embolization of the tumor and the pneumoperitoneum in minimally invasive surgery. This topic was evaluated by Kong et al13 in a retrospective analysis of 128 patients with FIGO stage IB and IIA cervical cancer, who underwent laparoscopic or robotic radical hysterectomy. Multivariate analysis demonstrated that laparoscopic intra-corporeal colpotomy represented a strong prognostic factor related to disease recurrence (OR=7.04, 95% CI 1.06 to 15.18; p<0.041), with five patients who presented peritoneal recurrence in this group. The authors conclude that CO2 pneumoperitoneum may carry a risk of positive vaginal cuff margin, as well, as intra-peritoneal tumor spread in these patients.
In our study, we also noted a high rate of adjuvant therapy, with 45 patients (42%) receiving adjuvant chemoradiation after surgery. In 29 (64.4%) of these patients, adjuvant treatment was indicated because of positive lymph nodes or parametrial involvement. In the other 16 patients (35.6%) the treatment was performed owing to Sedlis criteria, where the indication for adjuvant treatment is currently debated and not indicated in other oncological centers.14
This was a retrospective study and the events were few. However, of the 16 patients with recurrences, six had undergone adjuvant treatment owing to unfavorable prognostic factors, and 10 recurrences occurred in low-risk patients, who did not undergo any adjuvant treatment. When we analyzed the prognostic factors in patients with recurrences, no statistically significant differences were found with respect to age, histological type, nodal and parametrial involvement, lymphovascular invasion, or tumor size. There were no significant differences between the low-risk group and the group of patients with unfavorable prognostic factors who received adjuvant treatment (p=0.61) (table 2).
This study has several limitations, including its retrospective nature; the low number of recurrences, thus making it difficult to find associated factors; and finally, although the follow-up was adequate during the first 3 years, the rate of lost to follow-up at 5 years was high 22% (N=21). However, assuming the median time to relapse in this study as well as in other publications7 8 14 occurs before 2 years of follow-up, we consider that it does not modify the interpretation of the results presented.
In summary, we noted a recurrence rate of 15% in patients with early cervical cancer undergoing laparoscopic radical hysterectomy. We showed a 3-year overall survival rate after surgery of 81%. These outcomes support the inferiority of minimally invasive surgery as proposed by the results of the recently published LACC trial. Such findings have led our group to reconsider our approach, returning to the laparotomy approach in radical hysterectomy for patients with early invasive cervical cancer.
New investigations in progress will clarify some doubts about the tumor size,15 as well as, technical issues such as isolation of the vagina during colpotomy, or the combination of two surgical techniques, laparoscopic and vaginal, as potential strategies in the minimally invasive approach.
Footnotes
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available in a public, open access repository. Data are available upon reasonable request. Data may be obtained from a third party and are not publicly available. All data relevant to the study are included in the article or uploaded as supplementary information.