Article Text

Abstract
Objective Endometrial cancer surgical staging includes lymph node assessment which can lead to lower extremity lymphedema. The aim of this study was to estimate prevalence after sentinel lymph node biopsy versus lymphadenectomy.
Methods Consecutive patients who underwent minimally invasive surgery at the Mayo Clinic, Rochester, Minnesota, USA, between January 2009 and June 2016 for newly diagnosed endometrial cancer were mailed our validated 13 item lower extremity lymphedema screening questionnaire. We also ascertained via questionnaire whether the patient was ever diagnosed with lower extremity lymphedema.
Results Among 378 patients included in the analysis, 127 (33.5%) had sentinel lymph node biopsy with or without side specific lymphadenectomy (sentinel lymph node cohort) and 251 (66.4%) underwent bilateral lymphadenectomy prior to sentinel lymph node biopsy implementation at our institution or as 'backup' after sentinel lymph node mapping (lymphadenectomy cohort). The prevalence of lower extremity lymphedema was 41.5% (157/378), with 69 patients (18.3%) self-reporting a lower extremity lymphedema diagnosis after their endometrial cancer surgery at a median of 54.3 months (interquartile range 31.2–70.1 months), and an additional 88 patients (23.3%) identified by the screening questionnaire. The prevalence of lower extremity lymphedema was significantly higher in the lymphadenectomy cohort compared with the sentinel lymph node group (49.4% (124/251) vs 26.0% (33/127); p<0.001). When the cohorts were restricted to patients surgically managed after the introduction of sentinel lymph node, the prevalence of lower extremity lymphedema was still significantly higher in the lymphadenectomy cohort compared with the sentinel lymph node cohort (39.0% (41/105) vs 26.0% (33/127); p=0.03). In a multivariable analysis adjusted for body mass index, receipt of adjuvant external beam radiation, diabetes, congestive heart failure, and International Federation of Gynecology and Obstetrics grade, the adjusted odds ratio for the association between type of nodal sampling (lymphadenectomy cohort vs sentinel lymph node cohort) and lower extremity lymphedema was 2.75 (95% confidence interval 1.69 to 4.47, p<0.001).
Conclusions Sentinel lymph node biopsy was associated with a decreased risk of post-treatment lymphedema compared with lymphadenectomy in patients who underwent surgical staging for endometrial carcinoma.
- SLN and lympadenectomy
- endometrial neoplasms
- lymphatic system
Data availability statement
Deidentified patient data are available upon reasonable request.
Statistics from Altmetric.com
HIGHLIGHTS
The prevalence of lower extremity lymphedema was higher with lymphadenectomy than sentinel lymph node biopsy.
Lower extremity lymphedema differences persisted despite risk factors in the sentinel lymph node cohort.
Sentinel lymph node biopsy may confer the same risk of lower extremity lymphedema as hysterectomy alone.
Introduction
Endometrial cancer is the most common gynecologic malignancy.1 The disease usually presents at an early stage, with an excellent prognosis.2 Although the rate of metastasis in patients with early stage endometrial cancer is low, standard treatment includes a pelvic and para-aortic lymphadenectomy for staging.3 Therefore, many patients undergo lymphadenectomy despite having disease confined to the uterus, resulting in undesired side effects, such as lower extremity lymphedema.4–6
Lymphedema is a debilitating condition that occurs when the lymphatic system cannot process its load, causing protein rich fluid accumulation in subcutaneous tissues.7 Symptoms often start after cancer therapy, especially surgery or radiation therapy. When untreated, lymphedema advances in stage, leading to cellulitis, reduced functional capacity, and chronic lower extremity wounds.8 Beyond early stages, lymphedema cannot be reversed and must be chronically managed.9
Patient reported symptoms of lymphedema, such as limb heaviness, often precede objective swelling. We previously developed and validated a 13 question lower extremity lymphedema screening questionnaire to identify prevalence based on subjective symptoms.10 When administered to a large cohort of surgically staged endometrial cancer survivors, the instrument demonstrated significant lower extremity lymphedema with a prevalence of 47% over 6 years of follow-up.4 Associations with prevalent lower extremity lymphedema were seen with complete lymphadenectomy, as well as radiation therapy, obesity, and congestive heart failure. The risk attributable to nodal assessment using lymphadenectomy (vs hysterectomy alone) was 23%.
The prospective Gynecologic Oncology Group LymphEdema and Gynecologic Cancer Study also found striking rates of lower extremity lymphedema after lymphadenectomy. In this study, 34% of women who underwent endometrial cancer staging, including pelvic lymphadenectomy with or without para-aortic lymph node sampling, were subsequently diagnosed with lower extremity lymphedema defined as a limb volume change of ≥10%.11 In a secondary analysis, significantly more patients diagnosed with lower extremity lymphedema reported a measurable change in their quality of life (p<0.001).12
Sentinel lymph node biopsy offers an acceptable strategy between lymphadenectomy and no nodal evaluation in patients with endometrial cancer, and is included in the National Comprehensive Cancer Center Network guidelines.13–16 Feasibility of sentinel lymph node biopsy in endometrial cancer has been described in a large retrospective series,17 followed by accuracy reporting and confirmation from prospective trials.18–20 It has been hypothesized that this approach reduces side effects associated with lymphadenectomy, including lymphedema.21
Our objective was to examine the prevalence of lower extremity lymphedema in women who underwent sentinel lymph node biopsy as opposed to lymphadenectomy using the same instrument that was previously used in a similar population. For this study, we defined lower extremity lymphedema as any lymphedema below the navel; thus the legs, feet, lower abdomen, hips, buttocks, and genitals were included. We hypothesized that patients undergoing sentinel lymph node biopsy would have reduced lower extremity lymphedema compared with patients undergoing lymphadenectomy.
Methods
The study was approved by the Mayo Clinic institutional review board, and written informed consent was obtained from all subjects. Patients who underwent surgery for newly diagnosed endometrial cancer at the Mayo Clinic, Rochester, Minnesota, USA, between January 2009 and June 2016, provided research authorization, did not have synchronous cancer, and did not receive neoadjuvant chemotherapy, were included. In 2007, robotic assisted surgery was implemented for endometrial cancer, and this facilitated the widespread adoption of a minimally invasive approach by 2012.22 Sentinel lymph node biopsy was performed for endometrial cancer staging at our institution starting on October 18, 2013. Only patients with a planned vaginal, laparoscopic, or robotic surgery and with an acceptable lymph node asessment were included in this analysis; patients without nodes removed, or who underwent only para-aortic or unilateral pelvic lymphadenectomy were not included. Two cohorts were identified: (1) a lymphadenectomy cohort who underwent bilateral lymphadenectomy prior to sentinel lymph node implementation or as 'backup', after sentinel lymph node mapping during our period of transition to sentinel lymph node biopsy and (2) a sentinel lymph node cohort who underwent either sentinel lymph node removal and no pelvic lymphadenectomy or sentinel lymph node removal and side specific lymphadenectomy for no mapping per the sentinel lymph node algorithm.17 All patients underwent hysterectomy with or without bilateral salpingo-oophorectomy. Indocyanine green was used for the majority of sentinel lymph node identification, as previously described.23 Early in the transition to sentinel lymph node biopsy, we used blue dye injected in the same fashion. Retroperitoneal spaces were routinely and completely developed according to the National Comprehensive Cancer Center Network algorithm (inserted text about sentinel lymph node further below in this paragraph.ime of the ed patients had undergone a lymphadenectomy, however, aper on sentinel lymph node vs lymph node).
Starting in December 2016, patients in the two predefined cohorts who were known to be alive were mailed a survey that included queries for a self-reported history of clinically diagnosed lower extremity lymphedema, comorbidities known to be associated with lymphedema, and a 13 item screening questionnaire assessing symptoms such as swelling, skin tightness, and discomfort in different parts of the lower body in the past 4 weeks. Each question was scored on a 0 (not at all) to 4 (very much) scale, and a total score was derived as a sum of the 13 questions, which ranged from 0 to 52. A score of 5 or higher was previously determined to be an optimal cut-off score for identifying women with lower extremity lymphedema.10 If no response was received, a second survey was mailed after 1 month and patients were contacted by phone after 2 months. Two data specialists from the Mayo Clinic Survey Research Center independently entered the survey responses. The two versions of the entered data were compared and discrepancies were reconciled against the survey. Lower extremity lymphedema was defined using the same criteria as reported previously4 by either a self-reported diagnosis by a doctor, nurse, or other health professional after surgery (with a request for the date first told) and/or ‘screen positive,’ defined as a score of 5 or higher (appendix). The original validation set for our screening questionnaire was stratified by body mass index to ensure its performance in both obese (body mass index ≥30 kg/m2) and non-obese women. Sensitivity and specificity were 95.5% and 86.5% among all women (94.8% and 76.5% among obese women).10
Statistical analysis was performed using the SAS V.9.4 software package. Comparisons between groups (in study vs not in study; lymphadenectomy cohort vs sentinel lymph node cohort) were evaluated using the two sample t test for age, the Wilcoxon rank sum test for all other continuous variables, and the χ2 or Fisher’s exact test for categorical variables. Univariate logistic regression models were fit to evaluate the association of patient characteristics and surgical details with prevalent lower extremity lymphedema. Multivariable logistic regression models were fit to evaluate the association between type of nodal sampling (lymphadenectomy vs sentinel lymph node) and prevalent lower extremity lymphedema after adjusting for previously established covariates. Odds ratios (OR) and corresponding 95% confidence intervals (CI) were calculated from the parameters estimated by the models. All calculated p values were two sided, and p<0.05 was considered statistically significant.
Results
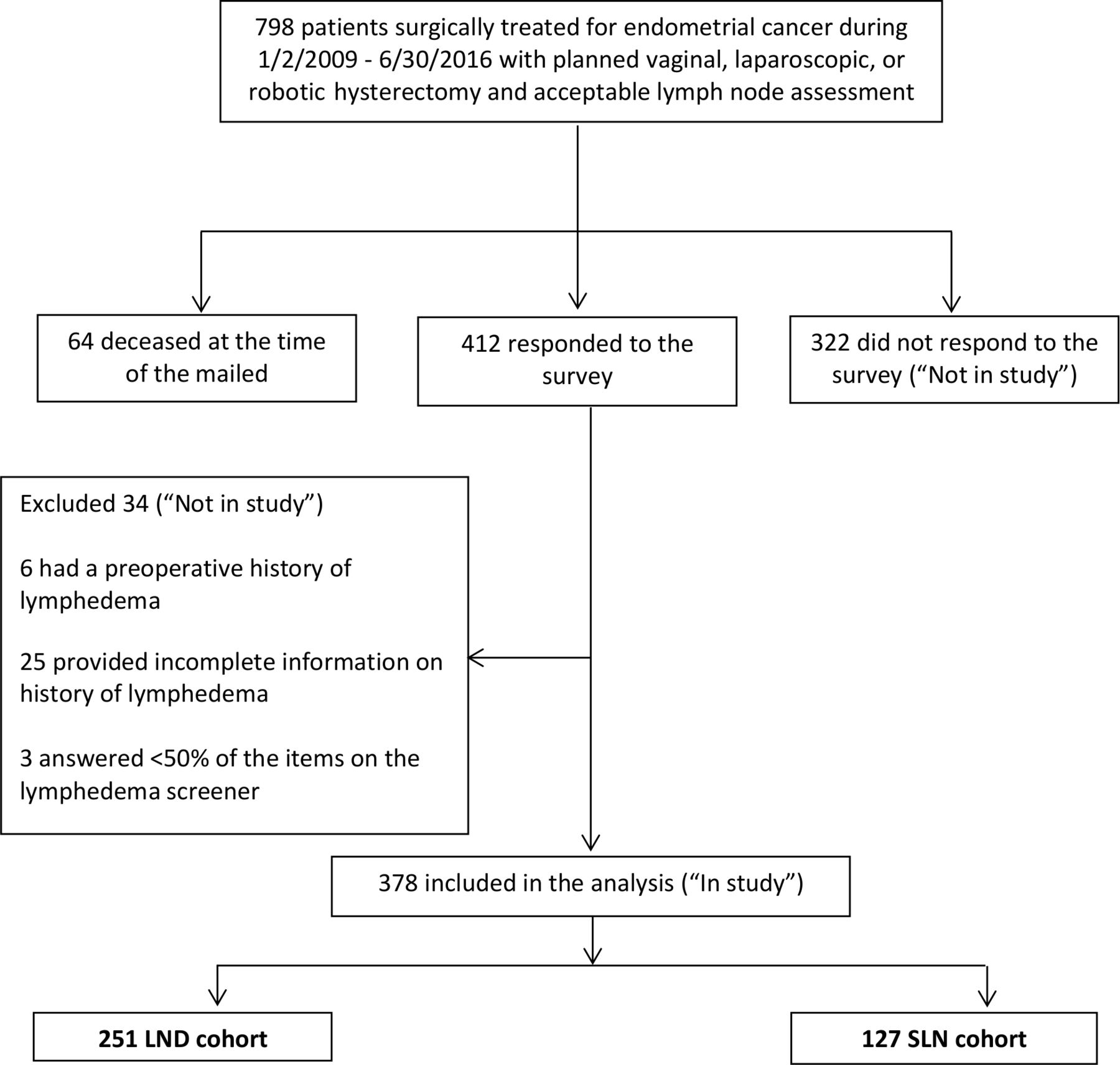
A total of 1664 patients met the inclusion criteria. Among these, eligibility was restricted to 798 patients for whom the intended route of surgery was vaginal, laparoscopic, or robotic and who had an acceptable lymph node assessment (Figure 1). Sixty-four patients were deceased at the time of the study. Surveys were mailed to the remaining 734 patients, of whom 412 (56.1%) responded. We excluded 34 respondents for the following reasons: preoperative history of lymphedema (n=6); answering an insufficient number of the 13 lower extremity lymphedema screening questions, defined as six or fewer questions (ie, <50%) (n=3); and did not indicate if or when a doctor, nurse, or other health professional had diagnosed lymphedema (n=25). There were 378 patients in the final sample ('in study'). Online supplemental Table 1 compares the characteristics of women included in this study and the remaining 356 women ('not in study') who either did not respond to the survey (n=322) or were excluded as described above (n=34). Compared with respondents, non-respondents or those who were deceased had a significantly higher median body mass index and had differing distributions of International Federation of Gynecology and Obstetrics (FIGO) grade and type of lymphadenectomy.
Supplemental material

{kind=link}
Flow diagram. LND, lymphadenectomy; SLN, sentinel lymph node.
Among 378 'in study' patients, 251 met the criteria for the lymphadenectomy cohort and 127 for the sentinel lymph node cohort. Table 1 contrasts patient characteristics at the time of surgery between these two cohorts. Patients in the sentinel lymph node cohort were significantly more likely to have congestive heart failure and lower grade disease compared with patients in the lymphadenectomy cohort. In addition, the sentinel lymph node cohort had significantly more patients with a body mass index of 40 kg/m2 or higher (25.2% vs 16.5%; p=0.04).
Characteristics of in study patients stratified by method of nodal sampling
Median time from surgery to survey response was 51.9 months (interquartile range (IQR) 32.3–72.3 months) for patients in the lymphadenectomy cohort and 25.6 months (IQR 21.8–29.9 months) for patients in the sentinel lymph node cohort. Sixty-nine patients (18.3%) self-reported that they were first told by a doctor, nurse, or other health professional that they had lymphedema in their lower body at a median of 54.3 months (IQR 31.2–70.1 months) following surgery. An additional 88 patients (23.3%) were identified by the survey with undiagnosed lower extremity lymphedema. The overall prevalence of lower extremity lymphedema was 41.5%, and it was significantly higher in the lymphadenectomy cohort compared with the sentinel lymph node cohort (49.4% (124/251) vs 26.0% (33/127); p<0.001).
In order to address the influence of imbalanced follow-up on lower extremity lymphedema rates in the two cohorts, a sensitivity analysis was performed focusing on the patients surgically managed after the introduction of sentinel lymph node at our institution. Among the subset of 232 patients, median time from surgery to survey response was 30.7 months (IQR 27.4–38.3 months) for the 105 patients in the lymphadenectomy cohort and 25.6 months (IQR 21.8–29.9 months) for the 127 patients in the sentinel lymph node cohort. The prevalence of lower extremity lymphedema was still significantly higher in the lymphadenectomy cohort compared with the sentinel lymph node cohort (39.0% (41/105) vs 26.0% (33/127); p=0.03). A total of 21% (22/105) and 3.1% (4/127) in the lymphadenectomy and sentinel lymph node cohorts self-reported that they were first told by a health professional that they had lower extremity lymphedema (p<0.001). An additional 18.1% (19/105) and 22.8% (29/127) in the lymphadenectomy and sentinel lymph node cohorts were identified by the survey with undiagnosed lower extremity lymphedema (p=0.38).
Table 2 summarizes the characteristics that were evaluated univariately for an association with prevalent lower extremity lymphedema based on all 378 patients. Only type of nodal sampling (ie, lymphadenectomy vs sentinel lymph node) was significantly associated with prevalent lower extremity edema. Although the prevalence of lower extremity lymphedema was higher in patients with diabetes (52.5% vs 39.5%) and in those who received adjuvant external beam radiation therapy (55.6% vs 40.3%), these differences did not meet the conventional level of statistical significance. In a multivariable analysis adjusted for body mass index (modeled using a cubic spline) and receipt of adjuvant external beam radiation therapy (which were identified in our prior study), the adjusted OR for the association between type of nodal sampling (lymphadenectomy vs sentinel lymph node) and lower extremity lymphedema was 2.87 (95% CI 1.78 to 4.62; p<0.001). The adjusted OR for lower extremity lymphedema was 2.75 (95% CI 1.69 to 4.47; p<0.001) after further adjusting for diabetes, congestive heart failure, and FIGO grade in addition to body mass index and adjuvant external beam radiation therapy.
Summary of variables evaluated univariately for an association with lower extremity lymphedema
During this study period, 428 patients were surgically treated for endometrial cancer with a planned vaginal, laparoscopic, or robotic hysterectomy but without nodal assessment. At the time of the survey mailing, 36 patients were deceased, and 177 of the remaining 392 patients returned a survey. Twelve of the 177 were excluded for the following reasons: preoperative history of lymphedema (n=5); answering an insufficient number of the survey questions (n=2); and did not indicate if or when a doctor, nurse, or other health professional had diagnosed lymphedema (n=5). The 165 remaining patients were eligible for analysis. Online supplemental Table 2 contrasts the patient characteristics at the time of surgery between the hysterectomy only cohort and the lymphadenectomy and sentinel lymph node cohorts. Patients in the hysterectomy only cohort were more likely than both sentinel lymph node and lymphadenectomy groups to have low stage, low grade, and endometrioid disease. The overall prevalence of lower extremity lymphedema was 27.3% (45/165) in this subset and median time from surgery to survey response was 55.1 months (IQR 39.9–74.9 months). The prevalence of lower extremity lymphedema was 32.8% (20/61) when restricted to patients surgically managed with hysterectomy only after the introduction of sentinel lymph node at our institution.
Discussion
In this study, we found that sentinel lymph node biopsy was significantly associated with less lower extremity lymphedema than lymphadenectomy using a validated patient reporting instrument.10 The difference in prevalence of lower extremity lymphedema between women who underwent lymphadenectomy versus sentinel lymph node was striking: 49.4% in the lymphadenectomy group and 26.0% in the sentinel lymph node cohort. This was despite the fact that our sentinel lymph node cohort had a higher median body mass index and a higher proportion of patients with congestive heart failure, and that 13.4% had a side specific lymphadenectomy for failed mapping. There was no difference in the rate of adjuvant external beam radiation therapy between the two cohorts. We observed differences in body mass index, FIGO grade, and type of lymph node assessment between patients who were 'in study' versus 'not in study'. This is possibly because patients with comorbidity associated with obesity, grade 3 endometrial cancer, and lymphadenectomy were more likely to be deceased from their disease. In our previous study, the prevalence of lower extremity lymphedema in women with endometrial cancer who underwent hysterectomy only, was 36.1%.4 Aging and associated comorbidities, such as obesity, chronic venous insufficiency, infection, and many other factors can contribute to this condition. In this current cohort, patients who underwent hysterectomy only had a lower extremity lymphedema rate of 27.3%. This was significantly less than those who had lymphadenectomy (p<0.001) but not statistically different from those who had sentinel lymph node (p=0.81), indicating that lower extremity lymphedema in women who undergo sentinel lymph node may not differ from those who have hysterectomy alone. Two recent studies reported similar findings. In one study, there was a 14-fold decrease in the risk of lower extremity lymphedema with sentinel lymph node as opposed to lymphadenectomy.24 In the other study, 27.2% (sentinel lymph node) and 40.9% (lymphadenectomy) reported lower extremity lymphedema.21 Similar to our investigation, this study showed that sentinel lymph node biopsy may not contribute to the development of lower extremity lymphedema beyond hysterectomy alone.
Lower extremity lymphedema adversely affects patients’ quality of life in most measured domains,4 25 and contributes to increased unemployment and healthcare utilization.26 27 Sentinel lymph node provides crucial staging information while solving the problem of over treatment, especially in low risk patients.2 28 Regardless of method, nodal assessment continues to be crucial for staging, prognosis, and adjuvant therapy decisions.29 While the best approach is still debated,30 sentinel lymph node has emerged as a safe and accurate method of assessment (sensitivity to detect node positive disease 97.2%, negative predictive value 99.6%), and has been shown in a prospective trial to be able to safely replace lymphadenectomy.20 As many physicians and institutions transition to sentinel lymph node instead of lymphadenectomy for endometrial cancer, a critical aspect of counseling patients will be the risk of adverse outcomes after surgery, including lower extremity lymphedema.
Strengths of our study include use of a validated instrument to detect lower extremity lymphedema; one which was confirmed to perform well in obese patients.10 Although some may consider leg circumference measurements to be the gold standard for lower extremity lymphedema assessment, patient symptoms are known to precede measurable lymphedema and may allow earlier intervention.31 In addition, the recent Gynecologic Oncology Group LymphEdema and Gynecologic Cancer Study noted significant challenges of pursuing these measurements, with difficulty possibly outweighing utility.12 Our cohort was large and limited to patients with endometrial cancer. In addition, predetermined criteria for use of sentinel lymph node and lymphadenectomy limited potential bias.2 Limitations include that patients who were deceased at the time of our survey mailing were more likely to have advanced disease and received external beam radiation therapy. Survey non-respondents differed significantly from respondents with respect to body mass index, FIGO grade, and type of lymphadenectomy, which may have introduced non-response bias. Finally, the median questionnaire follow-up time was shorter in the sentinel lymph node cohort because these patients were more contemporary. This may have introduced recall bias or resulted in reported lymphedema for multifactorial reasons, possibly unrelated to surgery. However, even when we restricted both groups to patients surgically managed after the introduction of sentinel lymph node, for which the median follow-up was similar, the prevalence of lower extremity lymphedema remained significantly higher in the lymphadenectomy cohort. The median follow-up time for patients in the sentinel lymph node cohort was 25.6 months, and prior studies have shown that most patients who experience clinically meaningful lower extremity lymphedema are diagnosed within 12 months.25 32 Recent prospective studies have performed follow-up for 24 months because of this, a time frame also covered by our sentinel lymph node cohort.12
Lower extremity lymphedema occurs in women undergoing surgery for endometrial cancer, with approximately 23% attributable to nodal assessment using lymphadenectomy (compared with hysterectomy alone).4 The advent of sentinel lymph node has the potential to significantly reduce this risk of lower extremity lymphedema and may provide an ideal opportunity for accurate nodal assessment with less short term and long term morbidity.
Supplemental material
Data availability statement
Deidentified patient data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by the Mayo Clinic institutional review board.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @Fmultinu
Correction notice This article has been corrected since it was first published. The third affiliation has been updated to include 'IRCCS'.
Contributors GG and AM conceived the project idea and obtained institutional review board approval. GG, GD, KY, ALW, and MM completed the chart review and survey information compilation, as well as conducted the data analysis. GG wrote the manuscript. FM, MA, AL, AK, AC, SD, and AM participated with edits of the manuscript and offered mentorship for completion of the project.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.