Article Text

Abstract
Objectives It is unclear if sentinel lymph node biopsy is associated with improved surgical outcomes compared with lymphadenectomy in patients with endometrial cancer. In this study we aimed to compare peri-operative surgical outcomes and treatment-related morbidity in patients who underwent robotic-assisted sentinel lymph node biopsy versus systematic pelvic lymphadenectomy or hysterectomy alone for apparent early-stage endometrial cancer.
Methods Records were reviewed of consecutive patients with International Federation of Gynecology and Obstetrics stages I–III endometrial cancer undergoing robotic-assisted staging from January 1, 2009, through June 30, 2016. For the purpose of this analysis we focused on the actual patients who had sentinel node biopsy only (ie, excluding those who had an associated lymphadenectomy either for failed mapping or during the learning curve). We also excluded patients who had para-aortic lymph node dissection from the lymphadenectomy group. Perioperative and 30-day surgical outcomes were compared between patients who underwent sentinel lymph node assessment and those who had pelvic lymphadenectomy or hysterectomy alone, respectively. Inverse probability of treatment weighting derived from propensity scores was used to minimize allocation bias in the comparison of outcomes between groups.
Results A total of 621 patients were analyzed: 188 (30.3%) with sentinel lymph node biopsy, 198 (31.9%) with pelvic lymphadenectomy, and 235 (37.8%) with hysterectomy alone. Inverse probability of treatment weights analysis balanced for baseline characteristics (age, body mass index, American Society of Anesthesiologists score, Charlson co-morbidity index, parity, prior cesarean section, and previous abdominal operation) showed no significant differences in intra-operative and post-operative complications, re-admissions, and re-operations between the groups. Compared with pelvic lymphadenectomy, the sentinel lymph node biopsy group had a shorter mean operative time (138.0 vs 222.8 min, p<0.001) and less median blood loss (50 vs 100 mL, p<0.001). Sentinel lymph node biopsy also was not associated with worse morbidity compared with hysterectomy alone.
Conclusions Introduction of sentinel lymph node biopsy reduces operative times and improves peri-operative surgical outcomes of robotic-assisted staging for apparent early-stage endometrial cancer without worsening the morbidity of hysterectomy alone.
- complications
- endometrial cancer
- morbidity
- robotic surgery
- sentinel lymph node
Statistics from Altmetric.com
HIGHLIGHTS
Sentinel lymph node biopsy reduces operative time of surgical staging for early endometrial cancer
Minimally invasive surgery and sentinel lymph node biopsy may improve quality of patient care in endometrial cancer
Sentinel lymph node biopsy does not worsen morbidity of robotic-assisted hysterectomy for endometrial cancer
Introduction
Surgical assessment of nodal involvement is a cornerstone in the staging process of endometrial cancer.1 In the past decade the surgical approach to endometrial cancer has evolved from a systematic pelvic and para-aortic node lymphadenectomy to a sampling of sentinel lymph nodes.2 3 This approach has been validated in a recent prospective study and can be considered the appropriate diagnostic technique for assessment of lymph node status in endometrial cancer.4 The 2017 National Comprehensive Cancer Network guidelines suggested sentinel lymph node biopsy for all patients undergoing surgical intervention for apparent early-stage endometrial cancer, regardless of the individual uterine risk factors for lymphatic dissemination.5
In the open operation, pelvic lymph node dissection has been shown to be an independent predictor of post-operative complications.6 A 23% attributable risk of lower extremity lymphedema has been shown among patients with endometrial cancer undergoing pelvic lymphadenectomy compared with hysterectomy alone.7 Furthermore, some investigators have reported pelvic lymphadenectomy to be associated with a wide range of non-lymphatic complications such as ureteral, vascular, bowel, and neurologic injuries.8 A suggested hypothesis is that reduction in the number of removed lymph nodes might correlate with a decrease in operation-related morbidity.9
On the basis of the limited data available in the current published literature,10 we hypothesized that sentinel lymph node biopsy is associated with improved surgical outcomes compared with pelvic lymphadenectomy, but estimation of the magnitude of its benefits is difficult. The present investigation aimed to compare peri-operative surgical outcomes (eg, operative time, blood loss, hospital stay) and treatment-related morbidity (ie, intra- and post-operative complications) of patients undergoing robotic-assisted management of endometrial cancer with sentinel lymph node biopsy versus pelvic lymphadenectomy or hysterectomy alone.
Methods
A review was performed for records of consecutive patients with apparent early-stage endometrial cancer who underwent a robotic-assisted operation at Mayo Clinic in Rochester, Minnesota, from January 1, 2009, through June 30, 2016, and gave research authorization. The Mayo Clinic Institutional Review Board approved this study.
For the purpose of this study, patients were excluded if they had an advanced stage of disease (International Federation of Gynecology and Obstetrics stage IV), carcinosarcoma histotype, synchronous malignancy, neoadjuvant treatments, or para-aortic staging. Patients were classified into three groups on the basis of their treatment: hysterectomy with or without bilateral salpingo-oophorectomy without lymph node status assessment; lymph node status evaluation through selective pelvic lymphadenectomy; and lymph node status assessment with sentinel lymph node biopsy.
The surgical procedures were performed with a robotic-assisted technique during the study period. All patients enrolled in the analysis had hysterectomy with or without bilateral salpingo-oophorectomy. The surgical techniques performed and the details of peri-operative management in hysterectomy alone and pelvic lymphadenectomy at Mayo Clinic are reported elsewhere.11 12 In accordance with the National Comprehensive Cancer Network guidelines,13 sentinel lymph node biopsy was performed with cervical injection of indocyanine green for most patients. On June 20, 2011, the Enhanced Recovery After Surgery protocol14–16 was introduced at Mayo Clinic to achieve faster recovery after surgery. A representation of the change in endometrial cancer management for patients treated for early-stage endometrial cancer at our institution is reported in the online supplementary figure.
Supplemental material
Data collection
Data were manually abstracted from the electronic health records, which included general demographic characteristics and obstetric, past medical, and surgical histories. The Charlson co-morbidity index5 was used for grading the co-morbidities of each patient. Peri-operative outcomes (ie, operative time, estimated blood loss, need for blood transfusion, and intra-operative and post-operative complications) and length of stay were recorded. Operative time was calculated and included robot docking time. Data on blood loss were extracted from surgical records as estimated by the surgeon during the surgical procedure. Length of stay was calculated from the day of admission to the day of discharge. Any unintentional damage (or opening) to an organ or structure was considered an intra-operative complication. Conversion from robotic to open approach was not considered a complication per se but was counted as a separate outcome. Post-operative complications within 30 days from the operation were graded with the Accordion Severity Classification.17 We report only complications of Accordion Severity Classification grade 2 or higher.
Statistical analysis
Given that the treatment approach was not randomly assigned, propensity score methodology was used to reduce the imbalance of measured baseline characteristics among the treatment groups, to thereby obtain less biased comparisons of outcomes between groups.18 Two parallel analyses were conducted for sentinel lymph node versus pelvic lymphadenectomy (as described below) and for sentinel lymph node versus hysterectomy alone. First, a multivariable logistic regression model was fit to estimate a propensity score value for each patient, defined as the probability that a patient would undergo a sentinel lymph node biopsy (versus pelvic lymphadenectomy) conditional of the measured baseline covariates included in the model. Then, with use of each patient’s specific propensity score value, inverse probability of treatment weights were derived as 1/propensity score for patients in the sentinel lymph node group and 1/(1 − propensity score) for patients in the pelvic lymphadenectomy group. Large weights were trimmed at the 95th percentile, and weights were then normalized according to the proportion of patients in the two treatment groups. Covariate imbalance between the two groups was assessed through evaluation of the standardized difference for each baseline covariate, separately in the unadjusted cohorts and the inverse probability of treatment weights-adjusted cohorts. Outcomes were compared between the sentinel lymph node and pelvic lymphadenectomy groups on the basis of fitting an inverse probability of treatment weights–adjusted logistic regression model for each binary outcome and an inverse probability of treatment weights–adjusted linear regression model for each continuous outcome, with the treatment group as a covariate in each model.
All calculated p values were two-sided and p values less than 0.05 were considered statistically significant. Statistical analyses were performed with the use of statistical software (SAS Version 9.3; SAS Institute).
Results
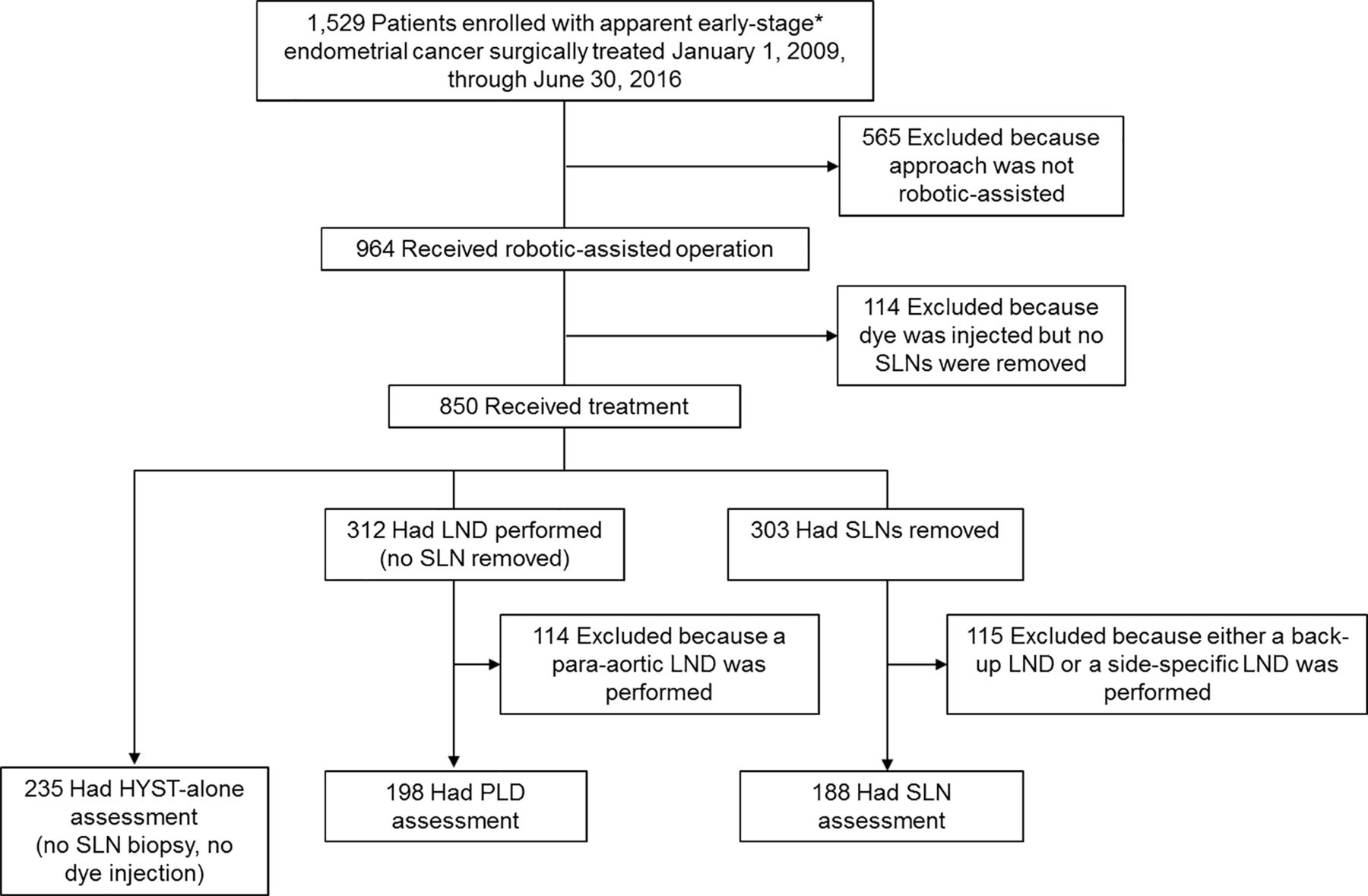
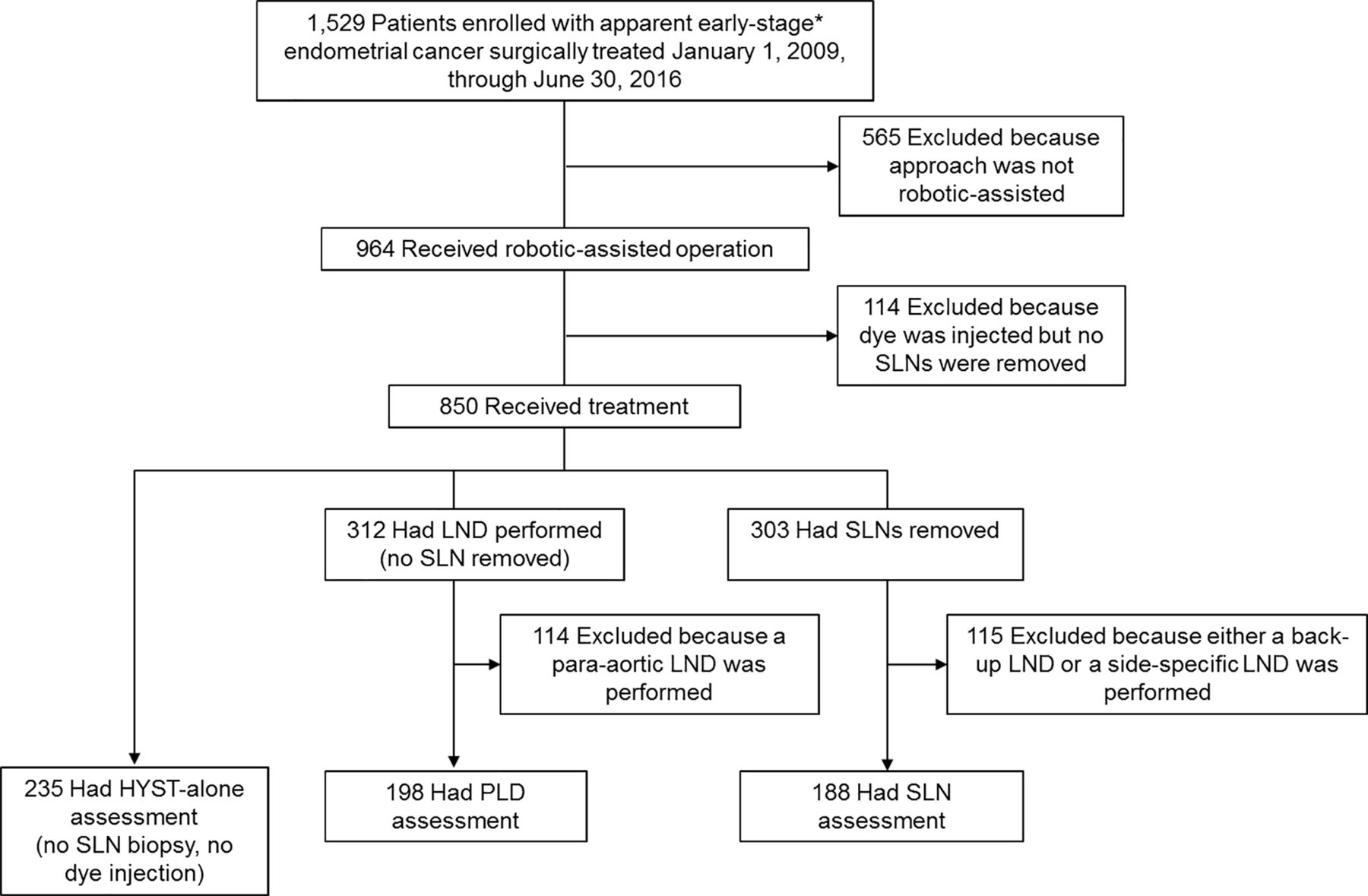
A total of 621 patients met the inclusion criteria and were analyzed: 188 (30.3%) with sentinel lymph node biopsy, 198 (31.9%) with pelvic lymphadenectomy, and 235 (37.8%) with hysterectomy alone. Among the sentinel lymph node biopsy group, cervical injection of methylene blue was performed in seven patients (3.7%). The flow diagram of the study population is reported in Figure 1. As is evident from the flow diagram, the main analysis was focused on the 'actual treatment'. In fact, we analyzed patients who had sentinel node biopsy only (ie, excluding those who had an associated lymphadenectomy either for failed mapping or during the learning curve). Also, we excluded those patients who had para-aortic lymph node dissection from the lymphadenectomy group.
{kind=link}
Flow chart of study population. Asterisk indicates patients with International Federation of Gynecology and Obstetrics stage IV disease, neoadjuvant treatment, invasive synchronous cancer, and carcinosarcoma who were excluded from the present investigation. HYST, hysterectomy; LND, lymphadenectomy; PLD, pelvic lymphadenectomy; SLN, sentinel lymph node.
Table 1 shows that each baseline characteristic included in the derivation of the propensity scores was well balanced between groups in the inverse probability of the treatment weights–adjusted cohort, with standardized differences below the recommended threshold of 0.100.
Comparison of baseline characteristics between systemic PLD and SLN biopsy groups
The comparative analysis of surgical outcomes between pelvic lymphadenectomy and sentinel lymph node biopsy in the inverse probability of treatment weights analysis did not show a statistical difference in intra-operative complications (p=0.19), conversion to open surgery (p=0.83), post-operative complications within 30 days from surgery (Accordion Severity Classification grade ≥2, p=0.50), re-admission within 30 days from surgery (p=0.61), and re-operation within 30 days from surgery (p=0.39) (Table 2). Patients who underwent pelvic lymphadenectomy were more likely to have longer hospitalization than those with sentinel lymph node biopsy (length of stay ≥2 days, 21.6% vs 7.8%; p<0.001), although the median (IQR) length of stay was 1 (1–1) day in both groups. Sentinel lymph node biopsy was associated with significantly lower mean (SD) operative time (pelvic lymphadenectomy, 222.8 [70.1] min vs sentinel lymph node, 138.0 [44.0] min; p<0.001), and less median (IQR) estimated blood loss (pelvic lymphadenectomy, 100 [50–200] mL vs sentinel lymph node, 50 [50–100] mL; p<0.001).
Comparison of peri-operative and 30-day surgical outcomes between systematic PLD and SLN biopsy groups
Comparisons of baseline characteristics between hysterectomy alone and sentinel lymph node biopsy are reported in Table 3. Each baseline characteristic included in the derivation of the propensity scores was well balanced between groups in the inverse probability of the treatment weights–adjusted cohort. When the sentinel lymph node group was compared with hysterectomy alone with use of inverse probability of treatment weights analysis (Table 4), no statistical differences were observed for intra-operative complications: hysterectomy alone versus sentinel lymph node biopsy (p=0.24), conversion to open operation (hysterectomy alone versus sentinel lymph node, p=0.34), post-operative complications within 30 days from operation (Accordion Severity Classification grade ≥2, p>0.99), re-admissions within 30 days from operation (p=0.56), or re-operation within 30 days from operation (p=0.19). Patients with hysterectomy alone had a mean operative time 15.6 min longer (p=0.002) and had no statistical differences in median (IQR) estimated blood loss (50 [50–100] mL for both hysterectomy alone and sentinel lymph node, p=0.26). Hospital length of stay of 2 days or more was statistically more frequent in the hysterectomy alone group (17.1% vs 7.9%; p=0.006), whereas no significant difference was observed for length of stay greater than 3 days (p=0.81). Over the study period, the introduction of the Enhanced Recovery After Surgery protocol did not influence the median length of stay of any treatment group. Tumor characteristics and histologic details of the three treatment groups are reported in the online supplementary table.
Comparison of baseline characteristics between hysterectomy alone (hysterectomy without lymph node status evaluation) and sentinel lymph node biopsy groups
Comparison of peri-operative and 30-day surgical outcomes between hysterectomy alone (hysterectomy without lymph node status evaluation) and sentinel lymph node biopsy groups
In order to evaluate if our results are consistent with a real-life, intention-to-treat situation, we repeated all the above comparisons by (1) adding to the sentinel lymph node group also those patients who had pelvic/para-aortic lymphadenectomy due to failure to map; and (2) adding to the lymphadenectomy group also patients who received para-aortic lymphadenectomy. The results (not shown) were similar, with a significantly shorter operative time, hospital stay, and less blood loss in the sentinel node group (compared with the lymphadenectomy group). Also, there were still no significant differences in the main peri-operative outcomes between the sentinel lymph node and the hysterectomy groups.
Discussion
Our study shows that sentinel lymph node biopsy is associated with improved surgical outcomes of traditional robotic-assisted staging for endometrial cancer without worsening the morbidity associated with total hysterectomy alone. The favorable peri-operative outcomes and acceptable rate of surgical complications observed in all three groups underline how minimally invasive surgical procedures provide improved outcomes for patients with endometrial cancer. We found, as expected, that sentinel lymph node staging was associated with a significant reduction in mean operative time (approximately 85 min), length of hospital stay, and a 50 mL reduction in median estimated blood loss compared with pelvic lymphadenectomy. The shorter hospitalization associated with sentinel lymph node biopsy reflects benefits for the patients19 20 and also for the entire healthcare system because it potentially can reduce surgical costs21 and improve patient satisfaction.
We observed also that the proportion of patients with a length of stay of two or more days was greater in the hysterectomy alone group than in the sentinel lymph node biopsy group. However, the reason for this finding is unclear. We observed that the shorter recovery time in the sentinel lymph node biopsy group, compared with hysterectomy alone, was not associated with the introduction of Enhanced Recovery After Surgery at our institution, because it remained significant over the different time periods and after adjustment for potential confounders.
In our series we did not observe an increase in morbidity for sentinel lymph node biopsy compared with hysterectomy alone. This is another important aspect in favor of implementation of sentinel lymph node biopsy in endometrial cancer. This finding may advocate for sentinel lymph node use in patients with low-risk endometrial cancer,22 especially when the pre-operative biopsy cannot rule out the presence of cancer and in institutions with inaccurate intra-operative frozen sections.23 Our findings suggest that implementation of the sentinel lymph node procedure in endometrial cancer may improve peri-operative outcomes and thereby provide reduction in surgery-related morbidity. As Geppert et al24 recently reported, the use of sentinel lymph node biopsy seems to be associated with a lower rate of specific lymphatic complications such as lower extremity lymphedema.
We note that, in this study, we focused our main analysis on the actual treatment that was given to patients and not on the intention-to-treat. In fact, we excluded from the sentinel node group all those patients who had an associated lymphadenectomy because of failure to map. However, even when we considered a 'real-life' situation by adding the above patients to the analysis, the main results did not change. The strengths of our study include the large number of patients treated in a single institution with a standardized surgical technique (cervical injection of dye and robotic-assisted surgery). Moreover, the measured baseline demographic and clinical characteristics of patients were balanced between the groups through the inverse probability of treatment weights analysis to minimize the potential confounders. In our analysis, we did not include patients who underwent para-aortic lymphadenectomy, and this presumably led to an underestimation of the reduction in morbidity associated with sentinel lymph node biopsy. Weaknesses of our study include its retrospective design, which might lead to implicit selection biases in the analyzed population. Furthermore, given that the prevalence was low (<10%) for many of the outcomes, there was limited statistical power to detect statistically significant differences between the treatment groups for some outcomes. However, none of the differences in outcome rates with a p value >0.05 were clinically meaningful. We acknowledge that our data came from a single teaching health care referral institution in the USA where robotic-assisted operation is the approach of choice for endometrial cancer treatment. This reduces the generalizability of our results at an international level. Moreover, the present investigation focused on short-term outcomes (30 days) without consideration of long-term lymphatic complications associated with endometrial cancer treatment, especially the rate of lower extremity lymphedema when sentinel lymph node biopsy is performed.
Conclusion
We confirm that robotic-assisted treatment of endometrial cancer is associated with favorable surgical outcomes and low morbidity rates. The implementation of the sentinel lymph node technique may improve the already excellent outcomes of minimally invasive full surgical staging through a reduction in operative time, blood loss, and length of stay. The performance of sentinel lymph node biopsy does not worsen the peri-operative morbidity of robotic-assisted hysterectomy alone for endometrial cancer treatment.
References
Footnotes
Twitter @Fmultinu
Correction notice Author name 'William A Cilby' has been corrected to 'William A Cliby'.
Contributors All authors contributed to the manuscript. JC, FM, LT, GG, and AM conceived and designed the study. JC, FM, LT, SC, ALW, GG, and AM contributed to the acquisition, statistical analysis, and interpretation of the data. FG, WC, AK, CL, GG, and AM provided insightful guidance and feedback for the study. All authors read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.