Article Text

Abstract
Objective To explore the factors influencing adoption of the sentinel lymph node (SLN) technique for endometrial cancer staging among gynecologic oncologists.
Methods A self-administered, web-based survey was sent via email (April 20 through May 21, 2017) to all members of European Society of Gynecologic Oncologists, International Gynecologic Cancer Society, and Society of Gynecologic Oncologists. Surgical and pathologic practices related to SLN and reasons for not adopting this technique were investigated.
Results Overall, 489 attending physicians or consultants in gynecologic oncology from 69 countries responded: 201 (41.1%), 118 (24.1%), and 117 (23.9%) from Europe, the USA, and other countries, respectively (10.8% did not report a country). SLN was adopted by 246 (50.3%) respondents, with 93.1% injecting the cervix and 62.6 % using indocyanine green dye. The National Comprehensive Cancer Network SLN algorithm was followed by 160 (65.0%) respondents (USA 74.4%, Europe 55.4%, other countries 71.4%). However, 66.7% completed a backup lymphadenectomy in high-risk patients. When SLN biopsy revealed isolated tumor cells, 13.8% of respondents recommended adjuvant therapy. This percentage increased to 52% if micrometastases were detected. Among the 243 not adopting SLN, 50.2% cited lack of evidence and 45.3% stated that inadequate instrumentation fueled their decisions.
Conclusions SLN with a cervical injection is gaining widespread acceptance for staging of endometrial cancer among gynecologic oncologists worldwide. Standardization of the surgical approach with the National Comprehensive Care Network algorithm is applied by most users. Management of isolated tumor cells and the role of backup lymphadenectomy for ‘high-risk’ cases remain areas of investigation.
- endometrial cancer
- lymphadenectomy
- minimally invasive surgery
- sentinel lymph node
- survey
Statistics from Altmetric.com
Highlights
SLN with cervical injection of indocyanine green is gaining acceptance for EC staging among gynecologic oncologists.
Adjuvant management of isolated tumor cells and micrometastasis still needs to be defined.
“Low level of evidence” is reported by gynecologic oncologists as primary reason for not adopting SLN technique.
Endometrial cancer is the most frequent gynecologic malignancy in developed countries. Approximately 63 000 women are diagnosed with early stage endometrial cancer in the USA annually.1 The cornerstone of surgical treatment is removal of the uterus, fallopian tubes, and ovaries.2 A minimally invasive approach (laparoscopic or robotic assisted) is preferred over open surgery for apparent early stage disease because it is associated with reduced post-operative pain scores, shorter hospitalizations, less surgical-related morbidity, and faster return to daily activities, with no difference in survival outcomes.3–6 One of the main independent predictors of survival is the presence of lymph node metastases; as such, its identification influences the administration of adjuvant therapies such as radiotherapy, chemotherapy, or both.7 8 A comprehensive dissection of the lymph nodes was traditionally suggested to assess for the presence of extra-uterine disease in patients with apparent early stage endometrial cancer, whereas the recent European guidelines2 recommend systematic removal of pelvic and para-aortic nodes in patients with high-risk endometrial cancer.9 However, when compared with simple hysterectomy, the performance of lymphadenectomy (pelvic alone or pelvic plus para-aortic) has been shown to prolong operative time, increase costs, and cause adverse effects such as lower-extremity lymphedema.10–12
With the intention of reducing surgical morbidity, sentinel lymph node (SLN) biopsy has been proposed in the past decade as a feasible option for endometrial cancer staging.13 Recently, the accuracy of this strategy has been tested in the FIRES (A comparison of sentinel lymph node biopsy to lymphadenectomy for endometrial cancer staging) trial, which showed 97.2% sensitivity and a negative predictive value of 99.6%.14 Although the reductions in adverse effects predicted to occur with this technique have not yet been fully investigated, it seems reasonable to hypothesize that the decreased radicality of SLN biopsy (compared with lymphadenectomy) may result in less morbidity and better quality of life.15 The National Comprehensive Care Network (NCCN) has included SLN biopsy as a valid method for endometrial cancer staging in its 2017 guidelines, but this method has not been universally adopted.16
The present survey aimed to investigate SLN technique adoption rates and identify factors that influence implementation of the SLN technique for endometrial cancer staging. In addition, we report surgical and adjuvant treatments commonly offered to patients with metastatic disease discovered during the SLN biopsy.
Methods
The study protocol was approved by the Mayo Clinic Institutional Review Board (Rochester, Minnesota, USA) and by the Society of Gynecologic Oncologists (SGO), International Gynecologic Cancer Society (IGCS), and European Society of Gynecologic Oncologists (ESGO).
A self-administered, anonymous survey (online supplementary table 1) was sent via email to all the members of the SGO, IGCS, and ESGO from April 20 through May 21, 2017. The Mayo Clinic Survey Research Center (Rochester, Minnesota) received membership lists from SGO (n=1014) and IGCS (n=854). When duplicate members were identified in both societies, the member was randomly assigned to only one group, yielding a final sample of 942 for SGO and 731 for IGCS. The Survey Research Center sent individualized emails to SGO and IGCS members such that each member was assigned a unique survey link that permitted the person to complete the survey only once. The use of the unique links for SGO and IGCS members also allowed the Survey Research Center to send two reminder emails to non-respondents.
Supplemental material
ESGO was unable to release their member list to the Survey Research Center, and thus an email with a generic survey link (ie, all respondents received the same link) was sent to ESGO members by that society. The number of ESGO members contacted to complete the survey and the number of ESGO members who were possible duplicates in the other two societies was not known. Because we could not identify non-respondents with the generic survey link, two subsequent emails were sent to all ESGO members, thanking them if they had already responded and encouraging them to respond if they had not.
The intended survey population was gynecologic oncologists affiliated with the above-mentioned societies who were fluent in reading English (the survey was not translated into other languages). Respondents who identified themselves as either medical or radiation oncologists, affiliated physicians in training (eg, residents and fellows), or retired physicians were excluded from the analysis. They also were not considered when calculating the response rates for IGCS and SGO. We calculated the response rates for these societies in two ways. The first used the American Association for Public Opinion Research response rate formula 1 (RR1), which assumes all non-respondents were eligible to complete the survey. The second formula (RR3) assumes the same proportion of eligible members among the non-respondents as the respondents.17 The denominator for ESGO was unknown; thus, a response rate could not be calculated for that society.
The survey was designed to assess surgical and pathologic practice details related to SLN biopsy among respondents, specifically to determine the use of the SLN technique as a common practice of surgical staging. Demographic characteristics of the respondents and their institutions included country of institution, type of institution (academic center, non-academic center), availability of laparoscopic and robotic surgery, yearly number of endometrial cancer cases surgically treated at each institution, and the availability of a frozen section pathology laboratory in each center. The questionnaire also assessed the awareness and application of the NCCN SLN algorithm developed at Memorial Sloan Kettering Cancer Center.16 18 Respondents were asked whether they performed frozen section or ultrastaging on the removed SLNs, and they were also asked about the use and type of adjuvant management in cases with isolated tumor cells (≤0.2 mm), micrometastases (>0.2 mm and ≤2 mm), or macrometastases (>2 mm). Reason(s) for not adopting SLN technique and alternative practices for staging were ascertained.
Statistical Analysis
Results are reported as frequency and percentages. For analytic purposes, respondents were classified into three geographic categories based on the location of their institutions (Europe, USA, and other). Comparisons of respondents from Europe and the USA were evaluated with the Fisher exact test or χ2 test. Factors were evaluated by univariate analysis for an association with SLN adoption for endometrialcancer staging, using the χ2 test for categorical variables and the Cochran-Armitage test for trend for ordinal variables. A multivariable logistic regression model was fit to evaluate combinations of factors for an association with SLN adoption. All calculated P values were two-sided and values of P<0.05 were considered statistically significant. Statistical analysis was performed with the SAS software package (v 9.4; SAS Institute Inc).
Results
Survey responses were obtained from 610 respondents, of whom 494 (81.0%) were an attending physician or consultant in gynecologic oncology, 70 (11.5%) were a resident, fellow, or retired physician or consultant in gynecologic oncology, 15 (2.5%) were a radiation or medical oncologist, and 31 (5.1%) were self-declared as ‘other’. After excluding the ineligible respondents, we calculated response rates for SGO (RR1=14.8%, RR3=14.9%) and IGCS (RR1=17.8%, RR3=21.1%). Among the 494 attending physicians or consultants in gynecologic oncology respondents who were considered for this analysis, 5 (1.1%) answered only the initial items regarding their position and years of experience; their responses were therefore excluded. The reported analyses are based on the remaining 489 respondents: 226 (46.2%), 124 (25.4%), and 139 (28.4%) from ESGO, IGCS, and SGO, respectively.
Overall, 436 of the 489 respondents (89.2%) reported the country where they practiced: Europe, n=201 (41.1%); USA, n=118 (24.1%); other, n=117 (23.9%); not reported, n=53 (10.8%). Sixty-nine countries (28 in Europe) were represented among these 436 respondents: 340 (78.0%) were from a high-income country, 51 (11.7%) were from an upper-middle-income country, 44 (10.1%) were from a lower-middle-income country, and 1 (0.2%) was from a low-income country. (Country income level was based on the World Bank list of economies as of March 2017.19) A map reporting the institutional countries of the respondents is shown in Figure 1.
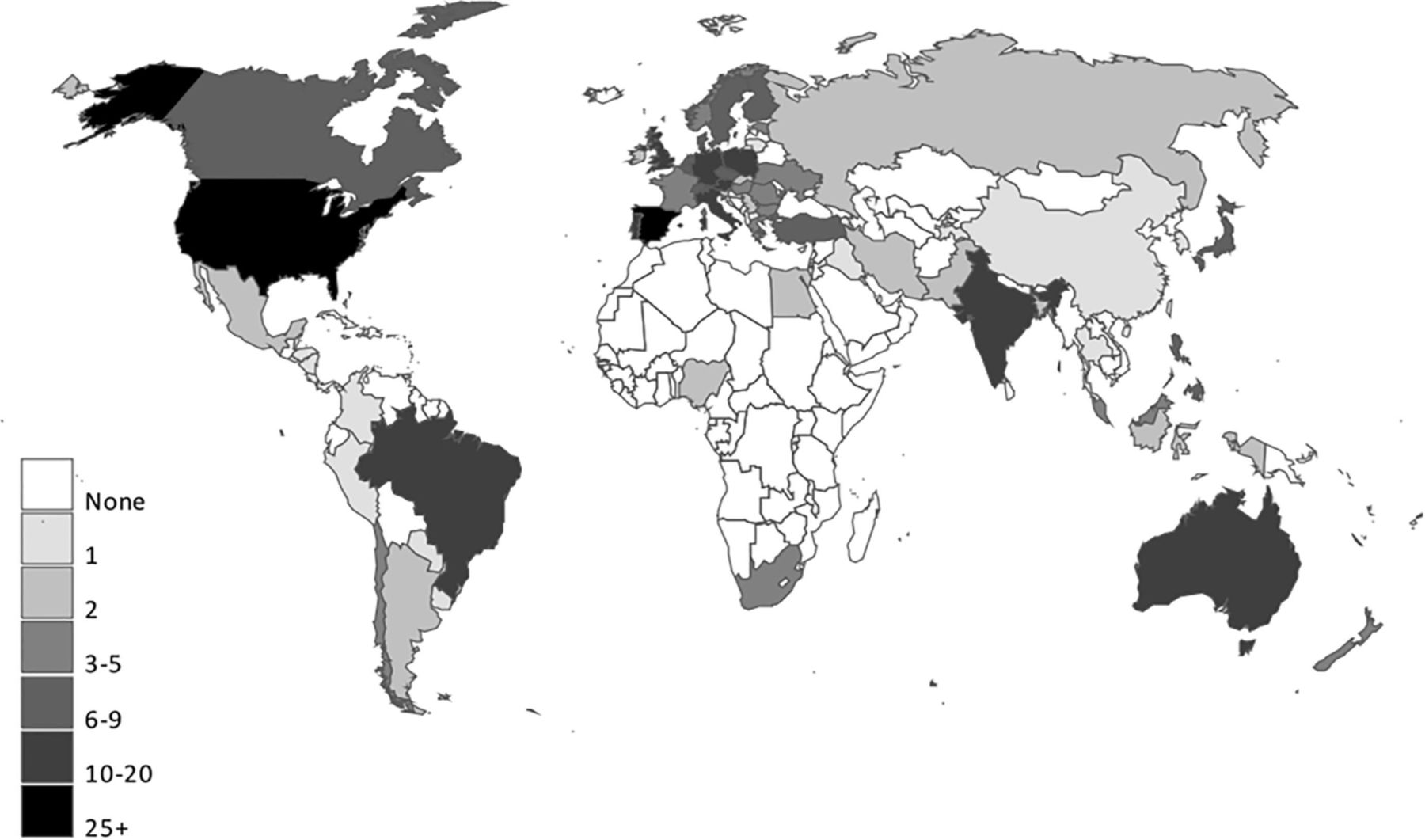
Map of respondents’ institutions. Countries were determined from answers to the question “What country are you from?” (489 respondents).19
The SLN technique was used by 246 (50.3%) respondents: 101 (50.2%) in Europe, 82 (69.5%) in the USA, 42 (35.9%) in other countries, and 21 (39.6%) who did not report their institutional country. When the SLN technique was used, indocyanine green was the most common dye (overall 62.6%; USA 87.8%; Europe 56.4%), and the uterine cervix was the site most commonly injected (overall 93.1%; USA 97.6%; Europe 90.1%). Despite the majority of the respondents reporting that they were applying the NCCN SLN algorithm (overall 65.0%; USA 74.4%; Europe 55.4%; other countries 71.4%), a backup lymphadenectomy in high-risk patients was still performed by 66.7% of respondents (USA 63.4%; Europe 68.3%), whereas only 16.3% (USA 25.6%; Europe 11.9%) stopped the dissection after SLN removal. For those who used SLN techniques, frozen section was part of the pathologic evaluation for 30.5% of the respondents (USA 28.0%; Europe 34.7%), and ultrastaging was performed by 78.9% (USA 84.1%; Europe 79.2%).
Among the 243 not adopting SLN techniques, the majority (n=126, 51.9%) pursued surgical staging, performing a selective pelvic lymphadenectomy, with or without para-aortic lymphadenectomy, on the basis of tumor risk factors (USA 69.4%; Europe 55.0%). Overall, 50.2% of respondents (USA 61.1%; Europe 61.0%) cited lack of evidence and 45.3% (USA 30.6%; Europe 37.0%) cited inadequate instrumentation as fueling their decisions not to use SLN biopsy. Detailed results are shown in Table 1.
Descriptive analysis of staging procedures for endometrial cancer among gynecologic oncologists, stratified by geographic region
Although most of the analyzed variables (univariate analysis) were significantly associated with adoption of the SLN technique (Table 2), after adjusting for the use of minimally invasive surgery (ie, laparoscopy, robotic surgery) in a multivariable model, none of the other variables attained statistical significance. Regarding the approach of choice for endometrialcancer, minimally invasive surgery was reported by 83.2% of respondents (USA 97.5%; Europe 83.6%) (Figure 2).

{kind=link}
{kind=link}
Suggested surgical approach for apparent early stage endometrial cancer and adoption of sentinel lymph node (SLN) technique. Results were based on the answers to the questions “Is minimally invasive surgery (laparoscopy and/or robotic surgery) the approach of choice for the treatment of apparent early stage endometrial cancer at your institution?” and “Do you use SLN technique for endometrial cancer staging?”; answers were stratified by geographic area. Highlights: SLN with cervical injection of indocyanine green is gaining acceptance for endometrial cancer staging among gynecologic oncologists; adjuvant management of isolated tumor cells and micrometastasis still needs to be defined; “low level of evidence” is reported by gynecologic oncologists as the primary reason for not adopting the SLN technique.
Factors associated with SLN adoption
Of the physicians who reported performing SLN biopsy as their common practice, 13.8% (USA 22.0%; Europe 10.9%) stated that they would always suggest adjuvant treatment when removed SLNs revealed isolatedtumor cells, whereas 58.9% reported that they would recommend adjuvant therapy on the basis of tumor risk factors. In cases of micrometastasis in the SLNs, the majority of respondents suggested adjuvant treatment should always be given, regardless of the presence of risk factors (overall 52.0%; USA 59.8%; Europe 49.5%). A majority (89.4%) supported the use of adjuvant therapy when macrometastasis was detected, regardless of the presence or absence of other risk factors (USA 98.8%; Europe 85.1%). The combination of chemotherapy and radiotherapy was reported to be the primary option when adjuvant treatment was prescribed (Table 3).
Clinical management of positive SLN, stratified by geographic region*
Discussion
The present investigation revealed that gynecologic oncologists consider SLN biopsy to be a feasible and valid option for the surgical staging of patients with apparent early stage endometrialcancer. Consistent with a review of published studies,15 our respondents indicated that the cervix was the preferred site of dye inoculation. Among respondents in the USA, indocyaninegreen was the dye most commonly used. As expected from prior analyses,20–22 we found that cervical injection of indocyaninegreen was the preferred technique for SLN biopsy. This method is associated with a higher SLN detection rate than hysteroscopic endometrial injection, without influencing the anatomic nodal distribution in patients with endometrialcancer.23 Although the decision to use this dye is supported by current evidence,15 only half of the European respondents adopting the SLN technique reported indocyaninegreen as their first option.
The use of the SLN technique is gaining widespread acceptance worldwide; however, the results of the present survey confirmed strong differences regarding endometrialcancer staging among gynecologic oncologists. For example, 15% of our survey respondents still indicated that they preferred the abdominal (open) surgical approach, despite clear evidence that minimally invasive techniques should be standard in this population.16
Although conclusions from the FIRES trial14 and a recent meta-analysis20 support the use of SLN biopsy for identifying lymphatic metastases in endometrialcancer staging, respondents from Europe and the USA cited a low level of evidence as the primary reason for not adopting the SLN technique. The lack of confidence in the SLN technique is also confirmed by the fact that for high-risk patients, complete lymphadenectomy is performed by almost 70% of respondents. This practice contradicts NCCN guidelines for SLN mapping in endometrialcancer staging, which suggest side-specific lymphadenectomy only for cases of unsuccessful mapping, but it is in accordance with the ESGO recommendations regarding lymphadenectomy in apparent early stage endometrialcancer.2 16 Results of ongoing prospective randomized controlled trials comparing SLN with lymphadenectomy will help define the role of systematically removing regional lymph nodes for endometrialcancer staging.24 25
As we predicted, the survey showed extensive discrepancies in the indications for adjuvant treatment, especially for patients with isolatedtumor cells and micrometastases, thus emphasizing the need for a consensus on post-operative management of these patients. The recommendation for adjuvant chemotherapy plus radiotherapy was much more uniform for patients with macrometastases, consistent with guidelines from Europe and the USA.2 16
Some limitations of the present survey need to be addressed. First, despite the high number of gynecologic oncologists who participated in this survey, our results may be affected by non-response bias. We were unable to determine overlap between ESGO versus SGO or IGCS member respondents. It is possible that some responses were received from the ESGO direct mailing; if these responses were submitted from oncologists with multiple society memberships, it could lead us to underestimate the response rate for the other two societies. Second, the survey was created with closed-ended questions that may not capture the full range of practice behaviors and attitudes. However, this method was necessary to avoid the plausible heterogeneity of the answers from open-text questions that may yield richer data but complicate analysis and interpretation of the results. Third, response rates ranged from about 15% to 21%, depending on the society and formula used. Thus, a bias due to survey non-responses is possible; that is, individuals who chose to respond may differ with respect to the study variables from those who did not respond. Fourth, grouping different geographic areas into the category of ‘other countries’ and receiving information only from the members of the ESGO, SGO, and IGCS might not reflect the actual practice of individual regions.
Although a subset of patients might not benefit from lymph node removal, it is extremely difficult to identify these patients pre-operatively because of the uncontrollable variable of change in grade and depth of invasion on final histopathology.26 27 We believe that the application of the SLN technique following the Memorial Sloan Kettering Cancer Center algorithm16 18 is a valid alternative to lymphadenectomy in patients with early stage disease.
SLN mapping with cervical injection is gaining widespread acceptance for staging of endometrialcancer among gynecologic oncologists worldwide. However, the standardization of this surgical approach (including the role of backup lymphadenectomy for ‘high-risk’ cases) and a general consensus on post-operative management in patients with micrometastases and isolatedtumor cells are still controversial. The present survey highlights a marked heterogeneity in the management of patients with early stage endometrialcancer among gynecologic oncologists worldwide. We hope our data will stimulate further prospective studies of adjuvant therapy in the case of micrometastases and isolatedtumor cells and a move toward standardization of the management of uterine cancer.
References
Footnotes
Presented at Presented at the 20th International Meeting of the European Society of Gynaecological Oncology, Vienna, Austria, 4–7 Nov 2017
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.