


Abstract
Aim: Adjuvant concurrent chemoradiation (CCRT) should be considered in surgically-treated patients with early-stage cervical cancer (ECC) who exhibit pelvic lymph node (LN) metastasis. Platinum-based chemotherapy is usually recommended during adjuvant CCRT, however, it is unclear which regimen has better prognostic outcomes. Patients and Methods: We reviewed the electronic medical records to find patients with primary ECC (FIGO stages IB-IIA) who underwent type III radical hysterectomy and adjuvant CCRT due to pelvic LN metastasis at the Samsung Medical Center, Sungkyunkwan University School of Medicine in Seoul, Korea, from November 1997 to September 2007. Results: Among 75 patients, 34 received weekly cisplatin. Combination chemotherapy was performed without consolidation in 21 patients and with consolidation in 20 patients. The mean follow-up period was 59.0 months and the five-year survival rate was 84.4%. In multivariate analysis, combination chemotherapy with and without consolidation was associated with improved disease-free survival [hazard ratio (HR)=0.23, 95% confidence interval (CI)=0.06-0.88, p=0.032, and HR=0.29, 95% CI=0.09-0.91, p=0.034, respectively]; combination chemotherapy with consolidation significantly improved overall survival (HR=0.11, 95% CI=0.02-0.87, p=0.037) when compared to weekly cisplatin. Conclusion: We found that platinum-based combination chemotherapy during adjuvant CCRT after surgery promoted better survival than a weekly cisplatin regimen in ECC patients with pelvic LN metastasis.
Cervical cancer is the seventh most common cancer in the world, the second most common cancer among women (1), and the leading cause of cancer-related death in women in developing countries (2, 3). About 71% of patients are diagnosed with early-stage cervical cancer (ECC), which includes (FIGO) stage I–IIA tumors (4).
With the limited value of the clinical staging system for predicting recurrence in ECC, several pathological findings after surgery have been used to predict recurrence and plan adjuvant therapy (5). Among these findings, the status of lymph node (LN) involvement is known to be the best independent predictor of disease-free survival (5, 6) and adjuvant concurrent chemoradiation (CCRT) should be considered in patients surgically-treated for ECC who exhibit pelvic LN metastasis (7); platinum-based chemotherapy is usually recommended during adjuvant CCRT (8). However, it is still unknown which regimen, single-platinum vs. platinum-based combination with consolidation vs. platinum-based combination without consolidation, results in better prognostic outcomes in ECC with pelvic LN metastasis.
This study was designed to investigate the survival difference between weekly cisplatin and combination chemotherapy with or without consolidation during adjuvant CCRT in patients with ECC who had pathologically-proven pelvic LN metastasis followed by upfront type-III radical hysterectomy.
Patients and Methods
Patients. Following Institutional Review Board approval (2013-08-070), we reviewed electronic medical records to identify patients with primary ECC (FIGO stage IB-IIA) who underwent type III radical hysterectomy and pelvic LN dissection with adjuvant CCRT at the Samsung Medical Center of Sungkyunkwan University School of Medicine in Seoul, Korea, between November 1997 and September 2007.
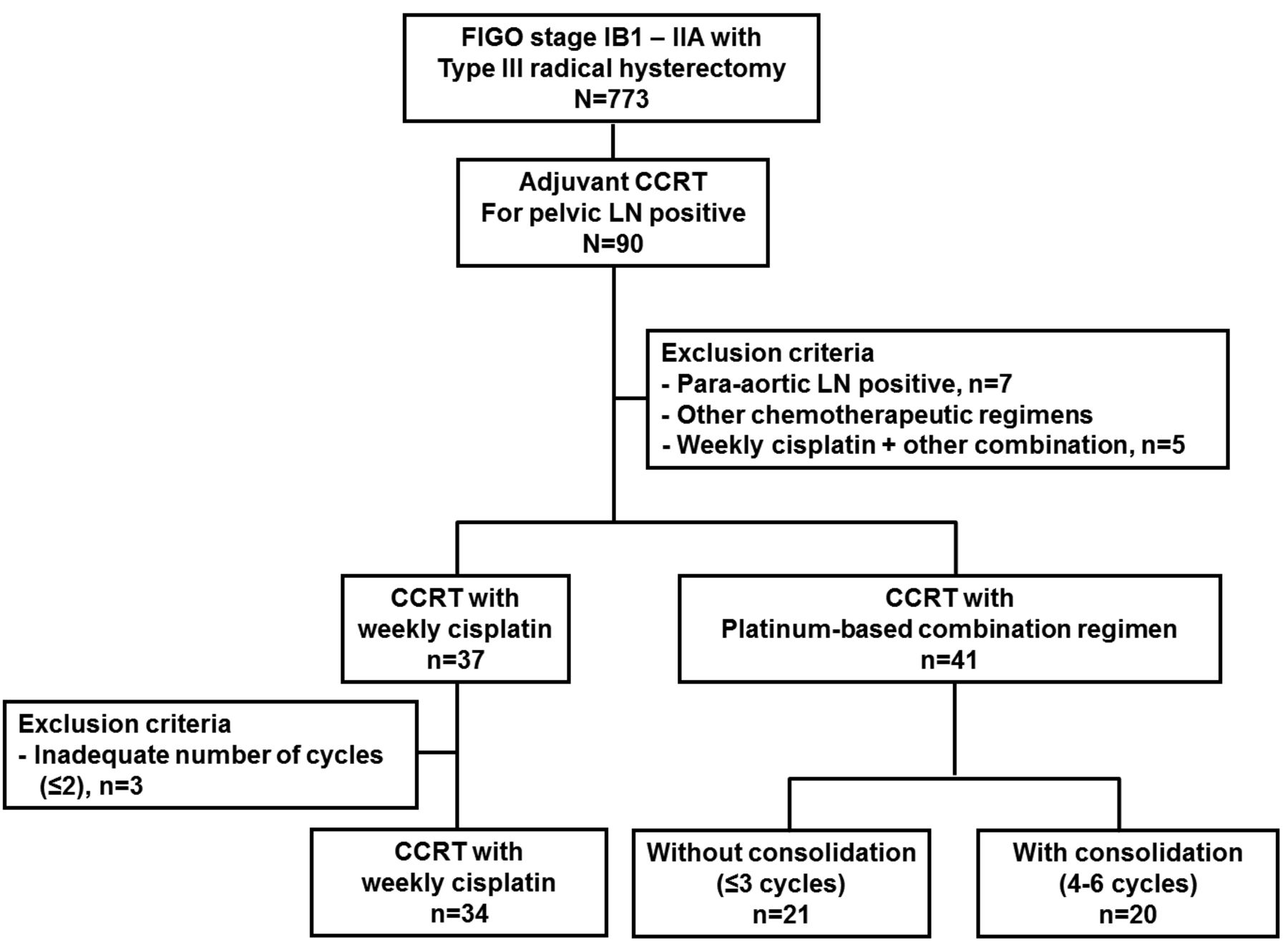
Flow chart of patients enrolled in the study. CCRT, Concurrent chemoradiation; LN, lymph node.
We excluded patients who were treated with neoadjuvant chemotherapy before surgery, those who had concomitant malignancy, and patients with sarcoma, malignant melanoma or neuroendocrine carcinoma of the cervix. Among patients who underwent type III radical hysterectomy (n=773), adjuvant CCRT due to pelvic LN metastasis was performed for 90 patients. We excluded patients with pathologically-proven (n=7) para-aortic LN metastasis and those who received insufficient chemotherapeutic doses (weekly cisplatin 1 or 2 cycles, n=3) or a sequential combination of weekly cisplatin plus combination chemotherapy (n=5). Finally, 75 patients (weekly cisplatin, n=34; platinum-based combination regimen without consolidation, n=21; platinum-based combination regimen with consolidation, n=20), were selected for analysis (Figure 1).
Treatment. After pathological confirmation, all patients underwent physical examination, intravenous pyelography (IVP), cystoscopy, chest x-ray, and magnetic resonance imaging (MRI) or computed tomography (CT) of the pelvis, as well as other routine laboratory tests prior to surgery. Positron-emission tomography (PET)/CT was performed in patients with IB2 and IIA or IB1 with suspicious pelvic LN metastasis on MRI or CT. Abdominal type III radical hysterectomy with bilateral pelvic LN dissection was performed. Bilateral salpingo-oophorectomy and para-arotic LN dissection, which is only indicated in cases with suspicious para-aortic LN metastasis on PET/CT, were not routine procedures. Patients who had more than one of the three high-risk factors (positive pelvic LN, microscopic parametrial invasion, and positive resection margins with tumor) underwent adjuvant CCRT and the patients with two or more of the three intermediate risk factors (stromal invasion of more than half of the cervix, lympho-vascular space invasion (LVSI), and a largest tumor diameter of 4 cm or greater) received adjuvant RT alone.
Adjuvant radiotherapy conditions were 1.8 Gy on days 1-5 of each week for a total of 28 fractions with a total dosage of 50.4 Gy of external radiation to a standard pelvic field. The concurrent chemotherapy used was one of the following regimens: a combination of cyclophosphamide with cisplatin, 5-fluoruracil (5-FU) with cisplatin, 5-FU with carboplatin, taxol with carboplatin, or weekly cisplatin. The combination chemotherapy consisted of group 1: cisplatin at 50 mg/m2 by 15-min intravenous infusion on day 1 and cyclophosphamide at a dosage of 750 mg/m2 per day given as a 2-min intravenous infusion on the same day, group 2: cisplatin at 60 mg/m2 by 15-min intravenous infusion on day 1 and 5-FU at a dosage of 1,000 mg/m2 per day, given as a 12-h intravenous infusion on days 1-5, group 3: carboplatin (AUC) 5 by 1-h intravenous infusion on day 1 and 5-FU at a dosage of 1,000 mg/m2 per day, given as a 12-h intravenous infusion on days 1-5, group 4: carboplatin AUC 5 by 1-h intravenous infusion on day 1 and paclitaxel at a dosage of 175 mg/m2 given as a 3-h intravenous infusion on day 1. The combination chemotherapy was repeated every three weeks, starting concurrently with radiation therapy. The weekly cisplatin regimen consisted of 30 mg/m2 over 1 h of intravenous infusion on day 1 every week, and six cycles of weekly cisplatin were provided if possible. The selection of a chemotherapeutic agent and the number of cycles was dependent on the attending physicians' preference. Basic eligibility criteria for CCRT included an Eastern Cooperative Oncology Group (ECOG) performance status of <2, adequate bone marrow function (white blood cell (WBC) count ≥3.5×109/l, neutrophil count ≥1.5×109/l, platelet count ≥100×109/l, and hemoglobin level ≥9.0 g/dl), adequate liver function (serum bilirubin level ≤2.0 mg/dl and serum aspartate aminotransferase (AST), alanine aminotransferase (ALT) and alkaline phosphatase levels two or more times greater than the upper limit of normal), and adequate renal function (serum creatinine level ≤1.5 mg/dl or creatinine clearance ≥60 ml/min).
Characteristics of groups 1 (weekly cisplatin), 2 (combination chemotherapy without consolidation) and 3 (combination chemotherapy with consolidation) of patients with early-stage cervical carcinoma with lymph node (LN) involvement.
Patients underwent follow-up examinations approximately every three months for the first two years, every six months for the next three years, and annually every year thereafter. During the routine follow-up, imaging studies (including CT or MRI and chest x-ray) were performed yearly. When tumor recurrence was suspected based on clinical findings or imaging studies, we usually used PET imaging to investigate the extent of disease. If distant metastasis was suggested on PET, CT or MRI, a biopsy of the lesion was performed on a case-by-case basis.
Recurrence, disease-free survival and overall survival. Patterns of recurrence were divided into the following three groups: I) locoregional recurrence developed in the pelvis; II) lymphatic recurrence developed in distant nodes, including the para-aortic and supraclavicular nodes; III) hematogenous/distant metastasis in the lung, liver or other organs with or without another pattern of recurrence. We defined disease-free survival as the time from the initial treatment to relapse or the last follow-up visit; overall survival was the time from the initial treatment to death due to cervical carcinoma or the last follow-up visit.
Statistical methods. Comparisons of means or medians were performed using one-way analyses of variance (ANOVA) as a parametric test or Kruskal-Wallis tests as a non-parametric test. Frequency distributions between categorical variables among the groups were compared using the χ2 test. Fisher's exact test was used if the expected frequency was <5. The overall and disease-free survival curves were calculated according to the Kaplan-Meier method using the log-rank test. The Cox proportional-hazards model was used for multivariate analyses. Statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS) software (version 12.0; SPSS, Chicago, IL, USA). p-Values ≤0.05 were considered statistically significant, and all p-values were two-sided.
Results
Among 75 patients, 34 received weekly cisplatin. Combination chemotherapy was given without consolidation in 21 patients and with consolidation in 20 patients. As shown in Table I, there were no differences among groups in terms of age, pelvic LN counts with tumor as well as LN-harvesting counts, distribution of histological subtypes, microscopic parametrial invasion, vaginal resection margin with tumor, deep tumor invasion, and lymphovascular space invasion (LVSI). In contrast, we observed a higher incidence of FIGO stage IIA disease in the combination-chemotherapy group than in the weekly-cisplatin group (26.8% vs. 8.8%, p=0.044), and larger tumor size in the combination-chemotherapy group with consolidation than in those without consolidation (3.5 cm±1.2 cm vs. 4.8 cm±1.4 cm, p=0.047). The mean follow-up was 59.0 months with a standard deviation of 28.0 months, and the five-year survival rate was 84.4%. There were 25 cases of cervical cancer recurrence (33.3%) and 13 cases of cancer-specific death (17.3%).
Number of cycles of chemotherapy in groups 1 (weekly cisplatin), 2 (combination chemotherapy without consolidation) and 3 (combination chemotherapy with consolidation chemotherapy) of patients with early-stage cervical carcinoma with lymph node involvement.
Table II shows in detail the chemotherapeutic regimens and cycles in each group. The completion rate of the scheduled number of cycles of chemotherapy was 82.1%, 90.5% and 95.0% in the weekly-cisplatin, combination-chemotherapy without consolidation and with consolidation groups, respectively. In the combination-chemotherapy group, 5-FU with cisplatin was the most popular regimen regardless whether patients received consolidation chemotherapy.
Overall, the combination chemotherapy groups, both with and without consolidation, did not have a significant difference in disease-free survival and overall survival from the weekly-cisplatin group in univariate analysis (Figure 2). In multivariate analysis, after adjusting for clinical stage (which significantly differed among groups) and other clinicopathological factors such as histology and pelvic LN metastasis, combination chemotherapy both with and without consolidation was associated with improved disease-free survival (HR=0.23, 95% CI=0.06-0.88, p=0.032, and HR=0.29, 95% CI=0.09-0.91, p=0.034, Table III); combination chemotherapy with consolidation significantly improved overall survival (HR=0.11, 95% CI=0.02-0.87, p=0.037, Table IV) when compared with the weekly-cisplatin group, respectively. In addition, we investigated whether recurrence patterns differed according to chemotherapeutic regimens and cycles. Although there were no cases of locoregional recurrence neither in the combination-chemotherapy group with or without consolidation. Overall, significant differences of recurrence patterns were not observed (data are not shown).
Discussion
In this study, we found that platinum-based combination chemotherapy during adjuvant CCRT after type-III radical hysterectomy was associated with better disease-free survival than a weekly cisplatin single regimen in patients with ECC with pelvic LN metastasis. Furthermore, consolidation chemotherapy after adjuvant CCRT significantly improved overall survival in those patients.
Previously our group had reported preliminary data that consolidation chemotherapy may not be associated with improved survival compared to a regimen without consolidation chemotherapy in patients with ECC treated with radical surgery and adjuvant CCRT due to high risk factors for recurrence (9). In that study, we included platinum-based combination chemotherapy regimens only and high risk factors were defined as pelvic LN metastasis, microscopic parametrial invasion, and vaginal resection margins with tumor. During the relatively short follow-up period, the estimated 2-year overall survival was 95.8% in the adjuvant CCRT alone group and 100% in the consolidation chemotherapy group, which were not statistically significant difference. On the other hand, longer follow-up period (59±28 months), difference in inclusion criteria, such as focusing on the pelvic LN metastasis only among factors for high risk of recurrence, and including a weekly-cisplatin alone group, may explain the clinically significant findings of the present study.
Among several postsurgical pathological findings, pelvic LN metastasis, microscopic parametrial invasion, and vaginal resection margin with tumor are considered as high risk factors for recurrence of ECC in patients treated with radical surgery (5). For this reason, at present, subsequent adjuvant CCRT is recommended to lower the risk of recurrence in this group of patients based on the results from a prospective randomized trial (GOG 109/SWOG 8797/RTOG 91-12) (10). However, the relative importance of the contributors of these postoperative risk factors to recurrence has been suggested. For example, LN metastasis has the greatest prognostic significance for recurrence among the other factors (11, 12), but even in patients with LN metastasis, disease-free survival or survival benefit after adjuvant CCRT was reported to differ according to the number of positive LNs involved (12, 13). Furthermore vaginal resection margin was not an independent prognostic factor for recurrence after adjusting for the other factors of recurrence (11, 12) and microscopic parametrial invasion might be a surrogate marker for large tumor size, which suggests that these factors may not necessarily function independently. As a result, we only included pelvic LN metastasis, which is the single most evident and independent risk factor with the greatest significance for recurrence, as an inclusion criterion among several risk factors and divided those patients into two groups based on the number of LNs with tumor (1 vs. ≥2)(13) based on the results of the previous study, in which when only one LN was positive there was smaller absolute benefit from adjuvant CCRT than in the cases of more than one positive LN, for the multivariate analysis in this study.

Disease-free (A) and overall (B) survival based on type of chemotherapy in patients with early-stage cervical cancer who had pelvic lymph node metastasis after type-III radical hysterectomy with pelvic LN dissection, who were treated with adjuvant therapies.
Univariate and multivariate analysis for disease-free survival of patients with early-stage cervical carcinoma with pelvic lymph node involvement (group 1, weekly cisplatin; group 2, combination chemotherapy without consolidation; group 3, combination chemotherapy with consolidation).
In the only prospective randomized trial (GOG 109/SWOG 8797/ RTOG 91-12) addressing the beneficial role of adjuvant CCRT after radical hysterectomy and LN dissection (10), clinicians administered FP (5-FU at 1,000 mg/m2 plus cisplatin at 70 mg/m2, intravenously) every three weeks for four cycles. The first and second cycles were started on days 1 and 22 of their RT, respectively, and the third and fourth cycles were scheduled after completion of RT. However, based on the results from studies addressing the use of weekly cisplatin during primary CCRT for bulky stage-IB cervical cancer (14) or locally advanced cervical cancer (IIB to VIA) (15), many clinicians now use six cycles of weekly cisplatin as a chemotherapeutic regimen during adjuvant CCRT after radical hysterectomy. Therefore, the optimal chemotherapeutic regimen during adjuvant CCRT after radical hysterectomy in ECC with risk factors for recurrence remains unknown, and our results suggest that platinum-based combination chemotherapy during adjuvant CCRT confers a better prognosis than the cisplatin single-regimen for ECC with pelvic LN metastasis.
Univariate and multivariate analysis for overall survival of patients with early-stage cervical carcinoma with pelvic lymph node involvement (group 1, weekly cisplatin; group 2, combination chemotherapy without consolidation; group 3, combination chemotherapy with consolidation).
The ideal number of cycles of combination chemotherapy during adjuvant CCRT is still unclear. At our institution, we considered adjuvant CCRT to include not only six cycles of weekly cisplatin but also three cycles of combination chemotherapy (first dose on RT on first day, second and third doses in the fourth and seventh week in each) during RT, which usually takes about six or seven weeks; further chemotherapy (including the fourth to sixth cycles) was classified into consolidation chemotherapy. Interestingly, even though platinum-based combination chemotherapy during adjuvant CCRT led to improved disease-free survival against weekly cisplatin, regardless of consolidation status, only platinum-based combination chemotherapy with consolidation was associated with improved overall survival as well as with disease-free survival. This may suggest the clinically significant role of consolidation chemotherapy after radical hysterectomy with adjuvant CCRT in ECC with pelvic LN metastasis. A large-scale, randomized phase III trial is ongoing to determine whether administering adjuvant systemic chemotherapy after adjuvant CCRT will improve disease-free survival compared to adjuvant CCRT-alone in patients with ECC found to have positive LN and/or positive parametrium after radical hysterectomy (RTOG 0724, NCT00980954).
Besides the small number of patients and the heterogeneous population, selection bias from the retrospective design is the potential limitation in this study. Regarding the feasibility of each chemotherapeutic regimen during RT, completion rate of the planned cycle of the chemotherapy during RT in each group was relatively high, especially in combination groups. However, some patients might have had three cycles of combination chemotherapy instead of six cycles due to intolerance to the regimens. For example, patients in the combination-chemotherapy group without consolidation were on average older than those of the consolidation group. Apart from the feasibility related with chemotherapy, consolidation was performed in patients with more advanced stage of disease, suggesting that the attending physician might have preferred the higher number of cycles of chemotherapy during RT in such cases. Future well-designed studies stratified by several clinical factors should be needed.
There were no cases of locoregional recurrence in the combination-chemotherapy group; however, the recurrence patterns among groups were not statistically significant different, possibly due to the low number of recurrences among patients.
In conclusion, we found that platinum-based combination chemotherapy during adjuvant CCRT after type-III radical hysterectomy with pelvic LN dissection confers better disease-free survival than a weekly cisplatin single regimen in patients with ECC with pelvic LN metastasis. Furthermore consolidation chemotherapy after adjuvant CCRT may contribute to the increased overall survival of these patients.
Acknowledgements
This study was supported by a grant of the Korea Healthcare technology R&D Project, Ministry for Health &Welfare Affairs, Republic of Korea (A092255).
Footnotes
-
Conflicts of Interest
The Authors declare that there are no conflicts of interest in regard to this study.
- Received July 12, 2013.
- Revision received August 16, 2013.
- Accepted August 22, 2013.
- Copyright© 2013 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}