Article Text

Statistics from Altmetric.com
Introduction
Rectovaginal fistula (RVF) is an abnormal connection between the rectum and vagina. Common causes are pelvic irradiation, obstetric trauma, Crohn’s disease, and post-surgical complications. Conservative treatments are usually performed in patients unfit for surgery and are characterized by a high recurrence rate. A common surgical approach includes fistula debridement and repair or flap interposition. Simple anatomic fistula repair is associated with a lower success rate than vascularized flap interposition. The Martius flap is a vascularized muscle-adipose flap obtained from the bulbocavernosus muscle.1 The blood supply is provided by branches of the pudendal artery. RVF repair by Martius flap is a safe procedure which offers good cosmetic and functional results, improving wound healing through neovascularization. Before surgery, a protective ileostomy is usually required.
Case presentation
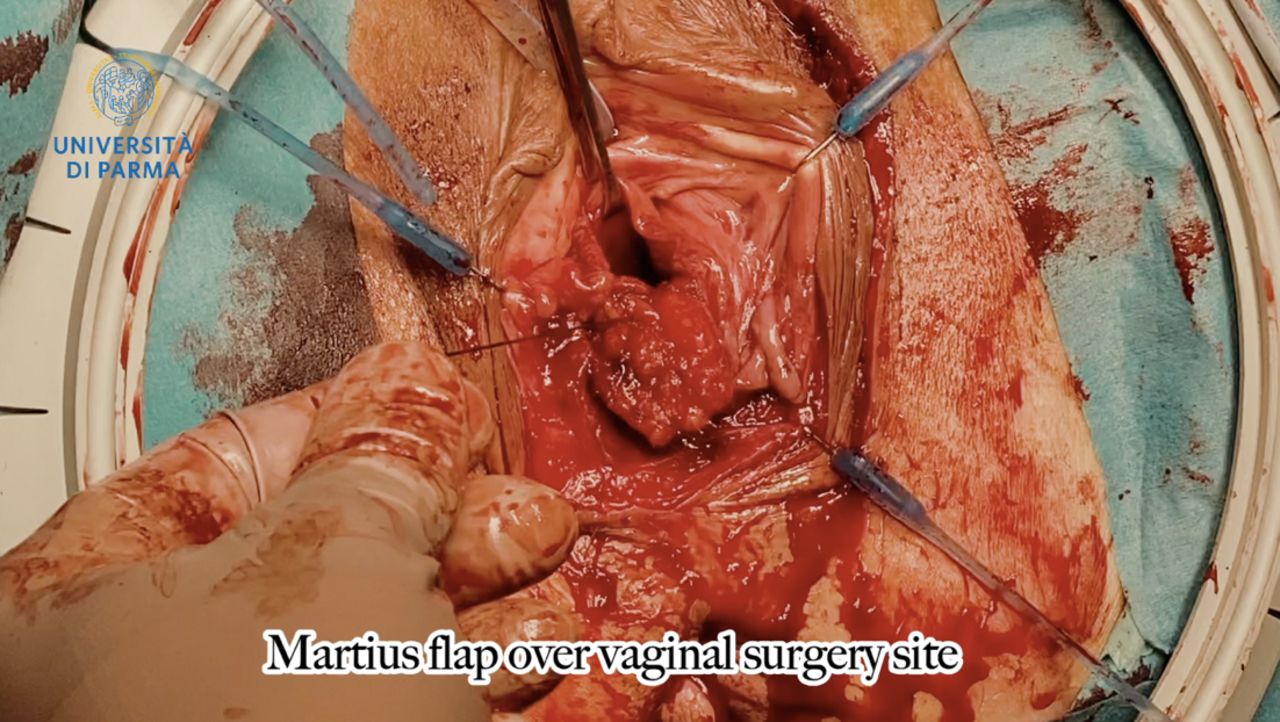
A 72-year-old woman with squamous cervical cancer, International Federation of Gynecology and Obstetrics stage IIB, was treated by exclusive chemoradiation at our department. After 3 years of negative follow-up, the patient was hospitalized for fecal vaginal discharge. Gynecological examination showed an RVF between the lower third of the posterior vaginal wall and the rectum. Colonoscopy confirmed the presence of an RVF of 2–3 mm diameter. Previous conservative treatments were ineffective. Therefore, after ileostomy, surgical treatment with a Martius flap was attempted. The surgical steps were as follows: (1) laterolabial skin incision; (2) labial dissection to identify the muscle-adipose flap; (3) mobilization of the flap; (4) opening of the lateral vaginal tunnel; (5) clamping of the superior pedicle; (6) transfer of the Martius flap to the vagina (Figure 1); (7) suture of the Martius flap over the vaginal surgical site; and (8) suture of the subcutaneous layer and skin. Amoxicillin, clavulanic acid, and metronidazole were administered 30 min before and continued for 7 days after surgery.

{kind=link}
Martius flap over the vaginal surgery site.
Results
The post-operative course was uncomplicated. After 6 months follow-up, no recurrence of RVF was observed. The patient reported a greatly improved quality of life.
Conclusion
The MF is an effective and safe procedure for RVF repair.
Ethics statements
Patient consent for publication
Footnotes
Contributors All authors discussed the results and contributed to the final manuscript. VAC is responsible for the overall content as guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.