Article Text

Abstract
Background Obstructive uropathy is present in almost 50% of patients with advanced cervical cancer and is associated with worse outcomes.
Objective To estimate the prognostic role of hydronephrosis and the impact of ureteral obstruction resolution in patients with locally advanced cervical cancer undergoing treatment.
Methods A retrospective cohort study was conducted of patients with International Federation of Gynecology and Obstetrics 2018 stage IIIB to IVA treated in a tertiary oncologic referral center in Brazil between January 2009 and June 2018. Three different groups were evaluated: (I) without hydronephrosis, (II) with hydronephrosis and urinary diversion, and (III) with hydronephrosis but no urinary diversion. Kaplan-Meier curves and log-rank tests estimated overall survival and progression-free survival based on the presence of hydronephrosis and urinary diversion. Clinicopathological variables were evaluated using univariate and multivariate Cox proportional hazard regression model for overall survival and progression-free survival.
Results A total of 151 patients were evaluated: group I – 62 (41.1%); II – 44 (29.1%), and III – 45 (29.8%). Stage, histological type or grade, tumor size, parametrial or lymph node involvement were not statistically different between groups. Group I had more favorable overall survival than groups II (p<0.003) and III (p<0.02); however, no difference was noted between groups II and III. Progression-free survival was similar between groups (log-rank test p=0.95). Univariate analysis revealed hydronephrosis (p=0.002) and concurrent chemoradiotherapy (p<0.001) as a prognostic factor for worse overall survival; while tumor size (p=0.023), pelvic lymphadenopathy (p=0.015), and histological type (p=0.03) were associated with worse progression-free survival. On multivariate analysis, hydronephrosis remained as an independently associated factor with worse overall survival (HR=2.06; 95% CI 1.12 to 3.79, p=0.02).
Conclusion Patients with locally advanced cervical cancer with hydronephrosis had lower overall survival even after controlling for potential confounding factors, but no difference in progression-free survival. Urinary diversion showed no impact on overall survival or progression-free survival.
- uterine cervical neoplasms
- ureter
- surgical procedures, operative
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, an indication of whether changes were made, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Obstructive uropathy in locally advanced cervical cancer can lead to worse outcomes, but it is uncertain if hydronephrosis changes overall survival in this population.
WHAT THIS STUDY ADDS
Patients without hydronephrosis had better overall survival than patients with hydronephrosis who underwent urinary diversion, and patients without hydronephrosis without urinary diversion.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
There were no differences in outcomes in patients with hydronephrosis regardless of urinary diversion, enabling individualized decisions for these patients.
INTRODUCTION
Cervical cancer is the second most diagnosed malignant tumor and the fourth leading cause of death among women worldwide.1 Due to the scant compliance with screening programs in developing countries, the diagnosis of advanced disease is common.2 Thus, there is a frequent association with complications such as anemia, sciatica, infection, vesicovaginal and rectovaginal fistula, rectal and bladder involvement, ureteral obstruction with hydronephrosis, and renal failure.3
Obstructive uropathy, present in 22–48% of locally advanced cervical cancers, can result in varying degrees of renal failure, compromising therapeutic options and leading to worse outcomes.4–6 The first-line treatment regimen for locally advanced cervical cancer with reduced risk of death, local and distant recurrence, is concurrent radiotherapy with cisplatin-based chemotherapy.7 Conversely, it is still uncertain whether the presence of hydronephrosis per se changes survival, given other confounding prognostic factors often related to tumor extension and the presence of pelvic and retroperitoneal lymph node metastasis.
Urinary diversion (ureteral stents, percutaneous nephrostomy or other) has emerged as an option to restore renal function and relieve obstructive symptoms. However, in cases of severe kidney injury, ureteral stents placement or percutaneous nephrostomy may not provide clinical benefits and could increase complications from interventions.8 9 This study aimed to evaluate the prognostic impact of hydronephrosis and urinary diversion in patients with locally advanced cervical cancer undergoing concurrent radiotherapy and/or chemotherapy.
METHODS
A retrospective cohort study was conducted of women with locally advanced cervical cancer (International Federation of Gynecology and Obstetrics (FIGO) 2018 stage IIIB to IVA) treated with chemotherapy and/or radiotherapy alone at Barretos Cancer Hospital between January 2009 and June 2018. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) recommendations were followed.10 Non-probability convenience sampling was performed for this study. Cases with uropathy prior to cervical cancer, lost to follow-up, or with missing data in the records were excluded. Three groups of patients were compared: group I – patients with locally advanced cervical cancer without hydronephrosis; group II – patients with locally advanced cervical cancer with hydronephrosis who underwent a urinary diversion; and group III – patients with locally advanced cervical cancer with hydronephrosis but no urinary diversion.
Variables Evaluated
Age, race (White, Black, pardo or other), disease stage (any IIIB, IIIC1, IIIC2 or IVA, according to the FIGO staging system) performed by imaging tests with MRI and/or CT,11 histological type (squamous cell carcinoma, adenocarcinoma or other), tumor size, the presence of parametrial involvement, pelvic or retroperitoneal lymph nodes, type of cancer treatment (concurrent chemoradiotherapy, radiotherapy or chemotherapy alone) were abstracted from individual patients' records. Creatinine clearance at admission was calculated using the Modification of Diet in Renal Disease formula.12 In addition, the following data regarding ureteral obstruction were analyzed: laterality (unilateral or bilateral); classification of pyeloectasis severity (mild, moderate, or severe) according to the radiologist’s subjective assessment on abdominal CT scan, MRI or ultrasound; and type of urinary diversion.
Data Collection
The REDCap (Research Electronic Data Capture) database13 was used for storing patient data. The local institutional review board approved this study under the Certificate of Presentation for Ethical Consideration number 98469218.6.0000.5437, and a waiver of informed consent was granted.
Outcomes
Primary outcome was overall survival and progression-free survival based on the presence of hydronephrosis and urinary diversion.
Statistical Analysis
Parametric data are presented as mean±SD and non-parametric data as median (IQR, 25th to 75th percentile). Categorical data are expressed as percentages. The normality of distributions was tested by the Shapiro-Wilk test. For parametric data, ordinary one-way analysis of variance with Tukey’s multiple comparisons test was used, while for non-parametric data, the Kruskal-Wallis test with Dunn’s post hoc test was performed. For categorical data, χ2 or Fisher’s exact test was applied.
Kaplan-Meier curves and log-rank tests estimated overall survival and progression-free survival. The significance of various clinicopathological variables for overall survival and progression-free survival was evaluated using univariate and multivariate Cox proportional hazard regression model. Covariates to be retained in the final model were chosen if p values were less than 0.1 on univariate analysis followed by a backward stepwise selection procedure (threshold p<0.05). Hazard ratios (HRs), 95% confidence intervals (CIs), and p values were summarized for covariates present in the final model. The analyses were performed using IBM-SPSS software v.21.0, a significance level of 5% was adopted, and only two-tailed values of p were considered throughout the statistical analysis.
RESULTS
During the study period, 194 patients with locally advanced cervical cancer were included, 151 of whom were eligible and analyzed. The reasons for exclusion were previous uropathy (n=8), lost to follow-up (n=33), and significant missing data in the records (n=2).
Patients were evaluated in three different groups: (I) 62 (41.1%) without hydronephrosis, (II) 44 (29.1%) with hydronephrosis, and urinary diversion, and (III) 45 (29.8%) with hydronephrosis but no urinary diversion (Table 1). In the group without urinary diversion the mean age of patients without ureteral dilation (53.6±15.2) compared with those with hydronephrosis and no urinary diversion was similar (52.3±14.7). Among patients with hydronephrosis mean age was lower in the group with urinary diversion (47.2±4.6, p<0.05) than in those without urinary diversion.
Clinicopathological features by hydronephrosis status
There was no statistically significant difference between the groups analyzed for disease stage, histological type or grade, tumor size, parametrial or lymph node involvement. The patients analyzed had stage IIIB (23.2%), IIIC1 (51%), IIIC2 (6.6%) or IVA (19.2%), most with squamous cell carcinoma (94.7%), and histological grade II (68.9%). In group I, 98.4% of the patients demonstrated evidence of parametrial involvement, while this finding was observed in all women in group III. Group I patients had a median tumor size of 6.2 cm (range 5.75–7.3), most with pelvic lymph node involvement (67.7%) and a minority with retroperitoneal lymphadenopathy (9.7%) at imaging evaluation.
The median (IQR) of patients' creatinine clearance levels at admission was statistically different among the groups: group I (97 mL/min (range 80.5–117)), group II (64 mL/min (range 34–98.5), p<0.001) and group III (77 mL/min (range 58–103), p<0.05). However, creatinine clearance rates in those with ureteral ectasia were not different, whether before or after urinary diversion (p=0.12) with 74.2% of patients having unilateral ureteral obstruction.
Regarding therapeutic regimens, 86.1% of patients underwent concurrent chemoradiotherapy with a total of 45 Gy in 25 fractions to the whole pelvis with weekly cisplatin or carboplatin, followed by brachytherapy. Comparison of women from group I with those of group II showed there were no differences in the treatment used. However, in group III, a significant number of patients underwent treatment exclusively with radiotherapy (26.7%), compared with 3.2% in group I (p<0.05).
In patients with hydronephrosis, 73 (82%) had moderate or severe dilation. While 23 (52.3%) patients who underwent urinary diversion had a cystoscopic ureteral stent placement, 17 (38.6%) underwent percutaneous nephrostomy, and 4 (9.1%) other procedures, such as cutaneous ureterostomy or ileal conduit urinary diversion. Patients with bilateral ureteral dilation had a higher rate of urinary diversion (38.6%), p<0.05 (Table 2). However, patients with unilateral left ureteral dilation had a lower rate of urinary diversion procedure (p<0.05).
Hydronephrosis and urinary diversion profile
There was a statistical difference in overall survival between patients with no ureteral dilatation and those with hydronephrosis, regardless of urinary diversion (group II p<0.003 and group III p<0.02). However, there was no difference in overall survival between groups II and III (p=0.52) (Figure 1). Median overall survival was not achieved in patients without hydronephrosis. The median (95% CI) overall survival in months in groups II and III was 21.9 (range 14.5–29.2) and 25 (range 11.46–38.4), respectively. For progression-free survival, there was no statistical difference between the groups (log-rank test p=0.95) (Figure 2).
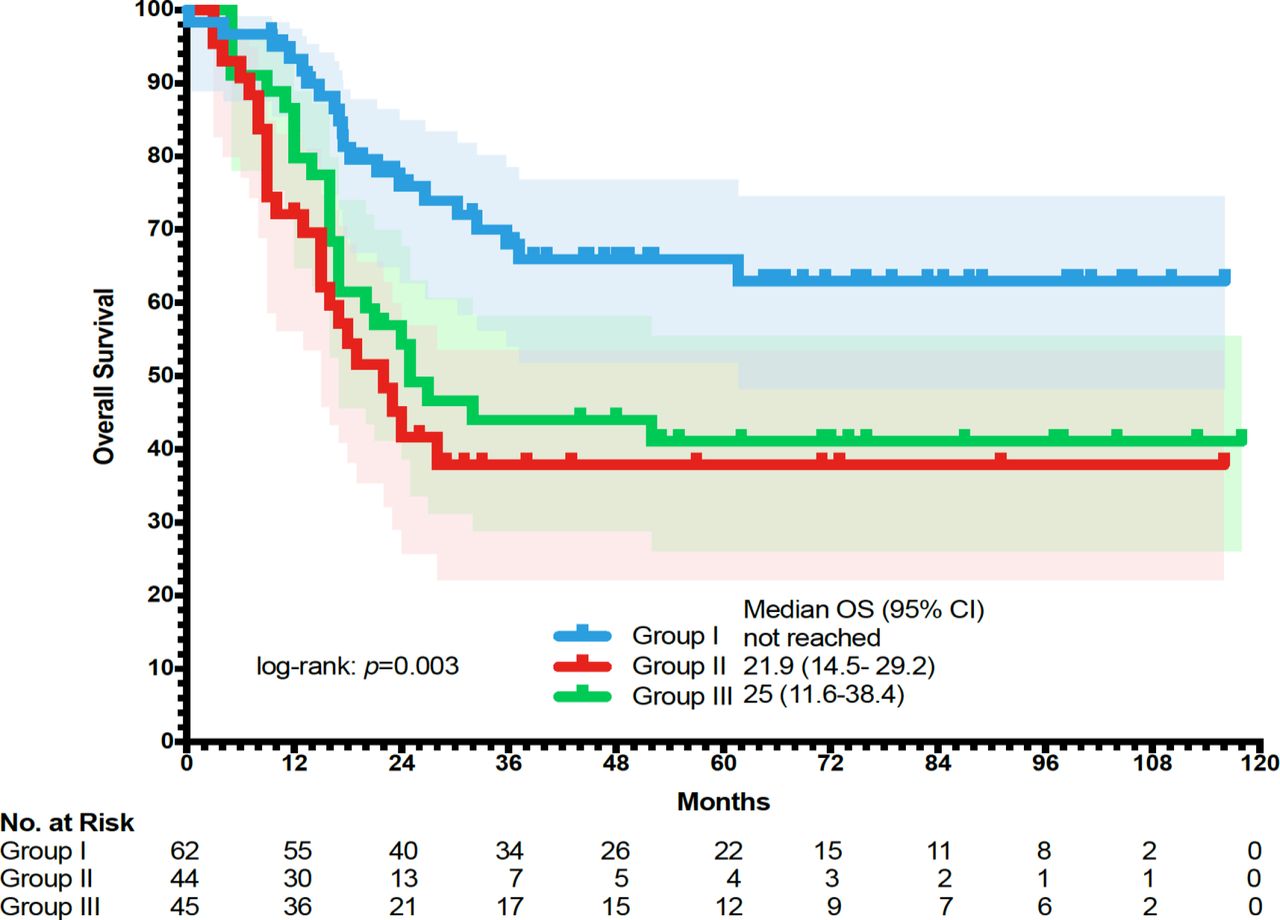
Overall survival (OS) by hydronephrosis.

{kind=link}
{kind=link}
Progression-free survival (PFS) by hydronephrosis.
Univariate analysis revealed that hydronephrosis (p=0.002) was associated with decreased overall survival (Table 3). Moreover, patients with larger tumor size (p=0.023) and positive pelvic lymph node status (p=0.015) had worse progression-free survival. Conversely, women with locally advanced cervical cancer who underwent concurrent chemoradiotherapy had improved overall survival (p<0.001) and those with squamous cell carcinoma (p=0.03) presented longer progression-free survival than the other histological subtypes. Following multivariate analysis, tumor size (HR=1.14; 95% CI 1.02 to 1.28, p=0.019), pelvic lymphadenopathy (HR=1.92; 95% CI 1.07 to 3.44, p=0.029), hydronephrosis (HR=2.06; 95% CI 1.12 to 3.79, p=0.02), and concurrent chemoradiotherapy (HR=0.43; 95% CI 0.21 to 0.87, p=0.019) independently impacted overall survival (Table 3). Tumor size (HR=1.18; 95% CI 1.05 to 1.33, p=0.006) and positive pelvic lymph node status (HR= 2.20; 95% CI 1.09 to 4.46, p=0.028) remained significantly associated with a shorter progression-free survival.
Prognostic factors by Cox proportional hazard regression
DISCUSSION
Summary of Main Results
Our study showed that patients with locally advanced cervical cancer with hydronephrosis had no difference in progression-free survival from those without obstructive uropathy but had lower overall survival even after controlling for potential confounding factors. However, performing urinary diversion had no impact on overall survival or progression-free survival. A large proportion of women had moderate to severe ureteral ectasia. In addition, the most frequent intervention for relief of ureteral obstruction was cystoscopic ureteral stent placement followed by percutaneous nephrostomy.
Results in the Context of Published Literature
Findings of a systematic review support the negative impact of hydronephrosis on the overall survival of patients with cervical cancer; however, differences in progression-free survival rates are less clear.14 Rose et al demonstrated an association of worse overall survival and progression-free survival in IIIB patients with hydronephrosis, even though they received similar doses of radiation and cisplatin-based chemotherapy.5 These results should be cautiously interpreted because the study was limited to patients whose renal function was normal or improved after urinary diversion. Disease severity in patients with hydronephrosis may vary by degree of parametrial involvement, tumor size, and lymph node involvement.5 Presence of hydronephrosis alone may lead to a worse prognosis than for disease with hydronephrosis and extension to the pelvic wall, thus leading to the proposal for stage IIIB substratification.4 15 16 The lower median overall survival in patients with hydronephrosis despite progression-free survival, similar to that of patients without hydronephrosis in our study, can be partially explained by the inflammatory and infectious complications associated with obstructive uropathy, the loss of renal function, possible immediate and late complications of invasive procedures such as vena cava filter passage due to thromboembolic predisposition, higher incidence of readmissions, and hospital-acquired complications. Interestingly, hydronephrosis in our analysis remained an unfavorable prognostic factor in multivariate analysis irrespective of creatinine clearance levels, corroborating findings from other studies.4 5 15 16
Survival data from patients with locally advanced cervical cancer regarding the impact of hydronephrosis and renal dysfunction are still scarce, heterogeneous, and often based on anecdotal evidence.14 In this study, although patients with hydronephrosis had lower levels of creatinine clearance on admission than those without ureteral dilation, there was no difference between those with hydronephrosis which underwent urinary diversion or not. Moreover, creatinine clearance levels were not associated with worse overall survival or progression-free survival. Therefore, the reliable cut-off creatinine clearance level is still a subject of controversy for decision-making for relief of ureteral obstruction. Alternatively, even though it is suggested that diuretic scintigraphy revealing ≥20% of kidney function is the commonly accepted threshold of kidney salvageability, it is noteworthy that a recent study showed that gynecologic oncology patients with <20% of renal function may recover from acute kidney injury after placement of a stent or percutaneous nephrostomy tube.17 18
Rose et al reported a correlation between relief of ureteral obstruction and improved overall survival and progression-free survival5; however, our study did not confirm these findings. It is worthwhile mentioning that patients in the current study were included irrespective of improvement in renal function after urinary diversion, which may explain the different findings. Choosing to relieve urinary obstruction in patients with locally advanced cervical cancer is complex, and shared decision-making is of utmost importance. Hydronephrosis may have substantial implications for therapeutic options. Thus, patients with obstructive uropathy are at increased risk of chronic kidney disease and, due to chemotherapy nephrotoxic properties, they often need dose reduction or omission.6 Hydronephrosis can lead to complications such as urinary tract infections, chronic low back pain, nausea, vomiting, bleeding, and chronic kidney failure.19 Moreover, evidence suggests that radiotherapy may eventually induce acute urinary obstructive disease.20 Thus, some authors consider early urinary diversion in cases of bilateral hydronephrosis with low creatinine clearance (<50 mL/min).20 On the other hand, despite the introduction of percutaneous techniques guided by ultrasound and CT, in addition to cystoscopic endourology, there is still a risk of urinary adverse events, such as low urinary symptoms, hematuria, urinary incontinence and retention, renal colic, nephrolithiasis, obstruction, multiple interventions, need for hospitalization, and increased exposure to healthcare-associated infections.8 9
Strengths and Weaknesses
The strengths of our study include the fact that we specifically evaluated patients with locally advanced cervical cancer (FIGO 2018 stage IIIB to IVA) according to presence or absence of hydronephrosis. In addition, we reported on a patient population from a single institution with consistent patterns of practice. There are several major weaknesses of our study. Among them, its retrospective nature and the sample size. We did not evaluate whether diuresis was present in patients with hydronephrosis without urinary diversion, which could be a possible bias in the overall survival and progression-free survival results, because residual diuresis may influence a slower rate of progression to end-stage renal disease. It can also be considered a limitation to reproducibility that assessment of the severity of hydronephrosis was subjective and that patients with FIGO stage IVB cervical cancer were not evaluated. In addition, no data were provided as to the specific treatments received by the patients or their mode of surveillance which might have impacted oncologic outcomes.
Implications for Practice and Future Research
A prospective multicenter study is warranted for a more in-depth analysis of the best time for urinary diversion, the ideal strategy of approach, and to determine the criteria to offer expectant management in patients with cervical cancer.
CONCLUSIONS
Hydronephrosis in locally advanced cervical cancer may be an ominous predictor of poor overall survival based on retrospective literature. However, limited data support urinary diversion as a treatment of ureteral obstruction to improve overall survival and progression-free survival. Potential risks must be balanced against possible benefits from expectant management and ureteral stenting or percutaneous nephrostomy. Therefore, a comprehensive medical evaluation must be performed, considering health resources, social and economic situation, so that a shared and individualized approach can be taken for patients with locally advanced cervical cancer, in order to plan the optimal treatment with improvement in prognosis and quality of life.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
References
Footnotes
Contributors LN: project conceptualization, project development, investigation, project administration, data collection, data analysis, and manuscript writing. JRZ: manuscript writing. CEMCA: manuscript writing. RLS: manuscript writing. MHS: manuscript writing. RDR: project conceptualization, project development, investigation, project administration, and manuscript writing. LN: guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.