Article Text

Abstract
Objective There is an increase in patient-reported outcome assessments to gain information on new drug candidates from the patient’s perspective. A data gap remains in patient-reported outcome measurements for anti-programmed death 1 (anti-PD-1) therapies in endometrial cancer. We present patient-reported outcome measures collected from patients with mismatch repair-deficient/microsatellite instability-high advanced or recurrent endometrial cancer treated with dostarlimab, an anti-PD-1 monoclonal antibody, in an expansion cohort of the GARNET trial.
Methods GARNET (NCT02715284) is a phase I single-arm study of dostarlimab monotherapy in multiple tumor types. Patients with advanced or recurrent mismatch repair-deficient/microsatellite instability-high endometrial cancer were treated with 500 mg of intravenous dostarlimab once every 3 weeks for four cycles, then 1000 mg of intravenous dostarlimab every 6 weeks. Patient-reported outcome assessments were an exploratory endpoint, measured using the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire C30 (EORTC QLQ-C30).
Results At data cut-off, 88 patients with mismatch repair-deficient endometrial cancer were included in the analysis. Patient-reported outcome assessment completion was >95.5% throughout cycle 7 of the trial, with no individual domain completion <90.9%. Quality of life, emotional functioning, and social functioning showed improvement compared with baseline. All symptom scores showed either improvement or stability from baseline through cycle 7. Categorical change in response across all symptom scales and single-item response scores showed stability or improvement for most patients. For patients who saw a worsening of their categorical change in response, ≤7.4% experienced a 2-category worsening and ≤2.5% experienced a 3-category worsening.
Conclusions Most patients remained stable or had improved quality of life while receiving dostarlimab for the treatment of recurrent or advanced mismatch repair-deficient endometrial cancer.
Trial registration number NCT02715284.
- Uterine Cancer
- Endometrium
- Quality of Life (PRO)/Palliative Care
Data availability statement
Data are available upon reasonable request. Anonymized individual participant data and study documents can be requested for further research from www.clinicalstudydatarequest.com.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, an indication of whether changes were made, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Patients with advanced or recurrent endometrial cancer have limited treatment options after progression on first-line therapy. Few trials have reported detailed quality of life data in advanced or recurrent endometrial cancer, particularly in trials of anti-PD-(L)1 immunotherapies.
WHAT THIS STUDY ADDS
The GARNET trial of dostarlimab, an anti-PD-1 monoclonal antibody approved for patients with mismatch repair-deficient/microsatellite instability-high advanced or recurrent endometrial cancer, provides patient-reported outcome data suggesting that dostarlimab treatment does not impair functioning or quality of life in patients with advanced or recurrent endometrial cancer.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE, OR POLICY
A data gap exists in quality of life research in endometrial cancer clinical trials. This study is one of the first to address this data gap to help improve the evaluation of cancer treatments for this patient population.
Introduction
Endometrial cancer is the most common gynecological malignancy in the European Union and the USA, and the incidence is rising.1 2 Annually, approximately 15 000 patients in the USA and 11 000 patients in the European Union are diagnosed with either advanced or recurrent endometrial cancer.3 Early-stage endometrial cancer is often successfully treated by surgery alone or surgery with adjuvant radiation and/or chemotherapy. However, in advanced or recurrent endometrial cancer, treatment options are limited for patients with progression on or after first-line therapy (usually platinum-based). Single-agent chemotherapy and endocrine therapy are the most common therapies used in the second line, but they have limited efficacy, resulting in a median overall survival of <1 year.4–7
Approximately 25–30% of endometrial cancers are associated with DNA mismatch repair deficiency and microsatellite instability-high status, which is the highest prevalence seen across all cancers.8–11 Mismatch repair-deficient/microsatellite instability-high tumors are associated with an increased rate of recurrence in patients with high to intermediate risk endometrial cancer.11 12 The higher mutation rate seen in mismatch repair-deficient/microsatellite instability-high tumors is often accompanied by an increased expression of programmed death 1 (PD-1) receptor, which potentially makes these tumors responsive to anti-PD-1 therapy.13–17
Dostarlimab (Jemperli) is an anti-PD-1 monoclonal antibody.18 The ongoing GARNET trial (NCT02715284) is a phase I, multi-center, open-label, single-arm study designed to assess the safety and anti-tumor activity of dostarlimab monotherapy in patients with advanced solid tumors.19 Dostarlimab has demonstrated clinical activity in various tumor types, including mismatch repair-deficient/microsatellite instability-high endometrial cancer, colorectal cancer, and non-small cell lung cancer.18 20 21 In patients with mismatch repair-deficient/microsatellite instability-high endometrial cancer, the observed objective response rate was 43.5% (95% CI 34.0% to 53.4%), with a disease control rate of 55.6% (95% CI 45.7% to 65.1%).22 The safety profile of dostarlimab is consistent with that of other anti-PD-1 antibodies; fewer than 4% of patients with mismatch repair-deficient/microsatellite instability-high endometrial cancer experienced a treatment-related adverse event that led to discontinuation, and no deaths were attributed to dostarlimab treatment.22
Dostarlimab is approved by the US Food and Drug Administration (FDA) as a monotherapy in adult patients with mismatch repair-deficient recurrent or advanced endometrial cancer that has progressed on or after prior treatment with a platinum-containing regimen and in adult patients with mismatch repair-deficient recurrent or advanced solid tumors that have progressed on or after prior treatment and who have no satisfactory alternative treatment options.23 24 In the European Union, dostarlimab is approved as a monotherapy in adult patients with mismatch repair-deficient/microsatellite instability-high recurrent or advanced endometrial cancer that has progressed on or following prior treatment with a platinum-containing regimen.22
Patient-reported outcome assessments measure the experiences related to an intervention of patients with cancer from the patient’s perspective. Well-developed questionnaires allow patients to provide a standardized response to obtain an adequate assessment of their perceptions.25 Several newer cancer treatments are offering longer periods of efficacy, which in turn lead to a longer course of anti-cancer treatment and the potential for accompanying adverse effects. Regulators, or professionals involved with the regulation of healthcare including pharmaceuticals and biologics, often working for government agencies such as the FDA or European Medicines Agency, are increasingly using patient-reported outcome data to gain information on drug tolerability to determine how the efficacy and safety of these products impact quality of life (QoL) and thus affect long-term adherence to these treatments.26 Both the American Society of Clinical Oncology and the European Society for Medical Oncology have proposed using patient-reported outcome measurements in addition to toxicity during clinical trials.25 26
The FDA recommends that patient-reported outcomes focus on three core concepts: symptomatic adverse events, or symptoms that can or might occur from use of a treatment; physical functioning, or the ability to perform activities that are instrumental to daily living; and disease-related symptoms, or symptoms that may accompany the primary cancer diagnosis.27 28 For endometrial cancer, most patient-reported outcome or QoL data have been obtained from patients with low-grade or early-stage disease, and few trials have reported QoL data in advanced or recurrent endometrial cancer.29 Furthermore, although patient-reported outcome measures have been used in clinical trials of anti-PD-1/PD-L1 immunotherapies, there has been a lack of consistent use across trials.30 However, these studies have shown that anti-PD-1/PD-L1 immunotherapies maintain QoL and contribute to less worsening of symptoms than standard of care, particularly in non-small cell lung cancer.31–33 In particular, a data gap remains in patient-reported outcome measurements for anti-PD-1/PD-L1 immunotherapies in endometrial cancer.
Because of the value found in patient-reported assessments, these outcome measurements were included in the GARNET trial of dostarlimab. In this analysis, patient-reported outcome assessments from patients with mismatch repair-deficient/microsatellite instability-high endometrial cancer in an expansion cohort of the GARNET trial are examined to look at the effect of dostarlimab treatment on the QoL of patients.
Methods
This trial was performed in accordance with the principles of the Declaration of Helsinki, Good Clinical Practices, and all local laws. The study protocol and/or other relevant documents received approval by the institutional ethics committee, institutional review board, and/or relevant competent authorities at each site.
Study Design
GARNET (NCT02715284) is a phase I single-arm study of dostarlimab monotherapy in multiple tumor types. The study consists of two parts: dose escalation and expansion. In parts 1 and 2A, the recommended therapeutic dose was determined to be 500 mg of intravenous dostarlimab once every 3 weeks for four cycles, followed by 1000 mg intravenous every 6 weeks until disease progression. The full study design, anti-tumor activity, and safety data have been previously published.19
Part 2B, an expansion cohort of the GARNET trial, enrolled patients with recurrent or advanced mismatch repair-deficient/microsatellite instability-high endometrial cancer, for whom patient-reported outcomes were assessed. Inclusion criteria and enrolling sites are provided in the online supplemental appendix.
Supplemental material
Patient-reported outcomes were an exploratory endpoint in patients enrolled in part 2B for expansion cohort A1 (mismatch repair-deficient endometrial cancer) under protocol amendment 3 (October 2017) and subsequent amendments, to support the analysis of health-related QoL. The patient-reported outcome assessment used was the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire C30 (EORTC QLQ-C30). The EORTC QLQ-C30 includes 15 domains: five functional scales (physical, role, emotional, cognitive, and social), three symptom scales (fatigue, nausea and vomiting, and pain), six single items (dyspnea, insomnia, appetite loss, constipation, diarrhea, and financial difficulties), and one global health status/QoL scale.
Patient-Reported Outcome Assessments
Patient-reported outcome assessments were collected every 3 weeks (±7 days) for the first 12 weeks, beginning on cycle 1/day 1, then every 6 weeks (±7 days) thereafter while the patient was receiving dostarlimab; they were collected before any other procedures were conducted at each assessment visit for all patients. Assessments were completed on paper and entered into the database by the clinical research team at each site. Once a patient discontinued treatment, patient-reported outcome assessments were performed during the end of treatment visit, the safety follow-up visit, and every 90 days (±14 days) during the post-treatment follow-up. After the safety follow-up visit, patient-reported outcome assessments may have been conducted via telephone.
Patient-Reported Outcome Assessment Inclusion Criteria
For a patient to be included in this analysis of the patient-reported outcomes assessments, they must have been included in cohort A1 of the GARNET trial, received any amount of dostarlimab, completed a patient-reported outcome assessment at baseline, and completed at least one follow-up of that instrument. Patients who fulfilled these inclusion criteria made up the patient-reported outcomes population.
Statistical Analysis
All analyses described were conducted on the patient-reported outcomes population as of the data cut-off date of March 1, 2020, and were considered exploratory in nature. Full statistical analysis, including the imputation method for missing data, can be found in the online supplemental appendix. Summary statistics were reported by visit. For functioning scales and disease-related symptoms, multi-item descriptive analyses were conducted, including an assessment of change from baseline. Study- and population-specific clinically meaningful important differences were not assessed within these data. The distribution of the change in response from baseline at each visit was reported for symptom scale items and six single response items. Patients reported their symptoms as one of four categories (not at all, a little, quite a bit, very much), which were then correlated to a change in baseline. Change from baseline was then calculated as one of the following: improved, defined as a 1-category decrease in response score; stable, defined as no change in response score; worsening 1, defined as a 1-category increase in response score; worsening 2, defined as a 2-category increase in response score; or worsening 3, defined as a 3-category increase in response score.
Results
At the time of data closure, 88 patients with mismatch repair-deficient endometrial cancer were included in the patient-reported outcomes analysis population. The number of patients ongoing in the trial and available to complete patient-reported outcome assessments decreased over the course of treatment (see online supplemental table 1).
Patient-reported outcome assessment completion was consistent across all domains, with the lowest rate of completion, 95.5%, observed at cycle 7 (percentage of missing data is shown in online supplemental table 1). The most common reason for non-completion was ‘administrative failure’, which refers to an entry not being recorded by the administrator of the assessment. Demographics and baseline characteristics are summarized in Table 1. The median age was 63 years (range 41–80 years); the majority of patients (65.9%) had endometrioid carcinoma, and all patients had received at least one line of prior anti-cancer therapy.
Demographics and baseline characteristics
Global Health Status and Functional Scales
The mean change in global health, or overall QoL, improved compared with baseline, beginning at cycle 2 and continuing over the course of dostarlimab treatment (Figure 1). Emotional and social functioning also showed a sustained improvement from cycle 2. The mean change in physical functioning and role functioning (the individual’s ability to fulfill responsibilities typical of their age or social setting) fell below baseline at cycles 2 and 3 but returned to baseline scores from cycles 3 through 7. No change from baseline was seen in cognitive functioning (Figure 1).
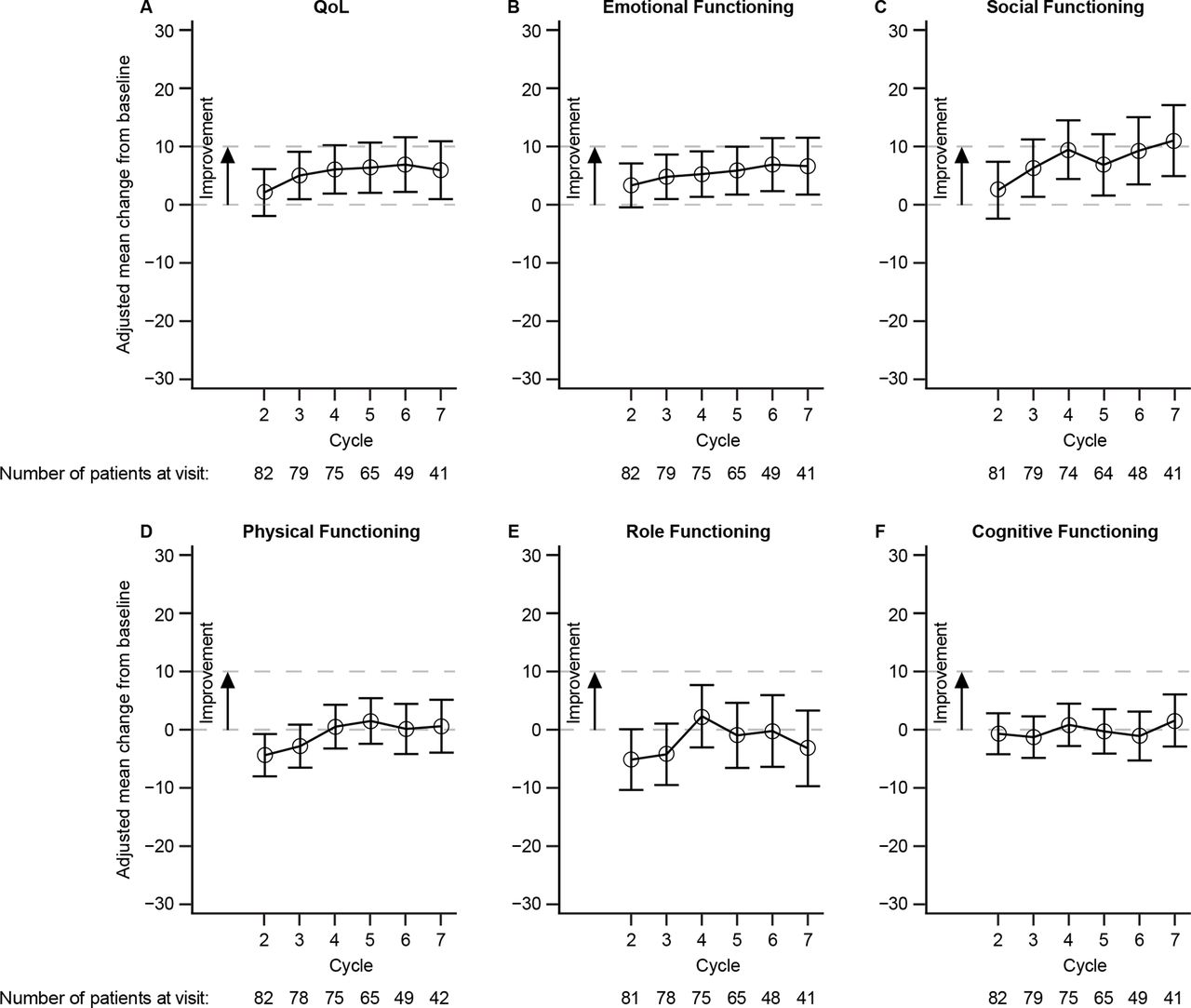
Mean change from baseline for EORTC QLQ-C30 QoL and Functional Scales. EORTC QLQ-C30, European Organization for Research and Treatment of Cancer Quality of Life Questionnaire C30; QoL, quality of life.
Symptom Scales
The three symptom scales measured on the EORTC QLQ-C30 had an improvement over baseline during dostarlimab treatment (Figure 2). Patients reported an improvement in pain beginning at cycle 2, and improvement in fatigue and nausea/vomiting was observed beginning at cycle 4. For all three symptom scales, once seen, improvement was sustained at least until cycle 7 of dostarlimab treatment.
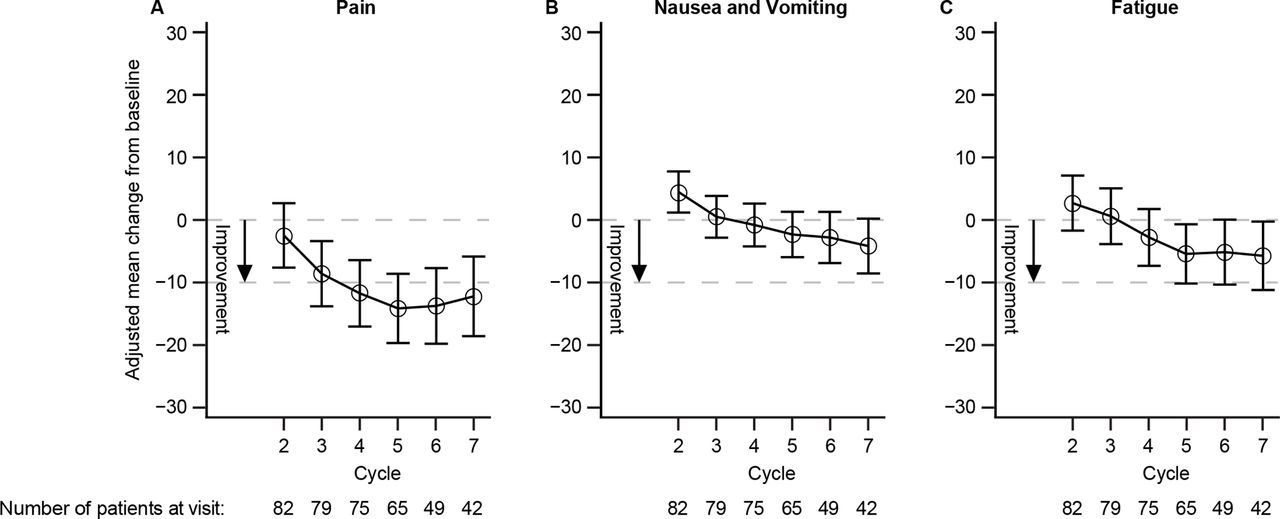
Mean change from baseline for EORTC QLQ-C30 symptom scores. EORTC QLQ-C30, European Organization for Research and Treatment of Cancer Quality of Life Questionnaire C30.
Single-Item Measurements
In two of the single-item measurements, the mean change from baseline demonstrated an improvement: insomnia, beginning at cycle 2, and appetite loss, beginning at cycle 4 (Figure 3A and B). Three single-item measurements remained stable from baseline: constipation, financial difficulties, and dyspnea (Figure 3C–E). The last single-item measurement, diarrhea, showed a slight improvement beginning at cycle 2, but this improvement was not sustained during cycles 6 and 7 (Figure 3F). Information on single-item measurement responses and categorical change in response can be found in the online supplement and in online supplemental Figures 1 and 2.
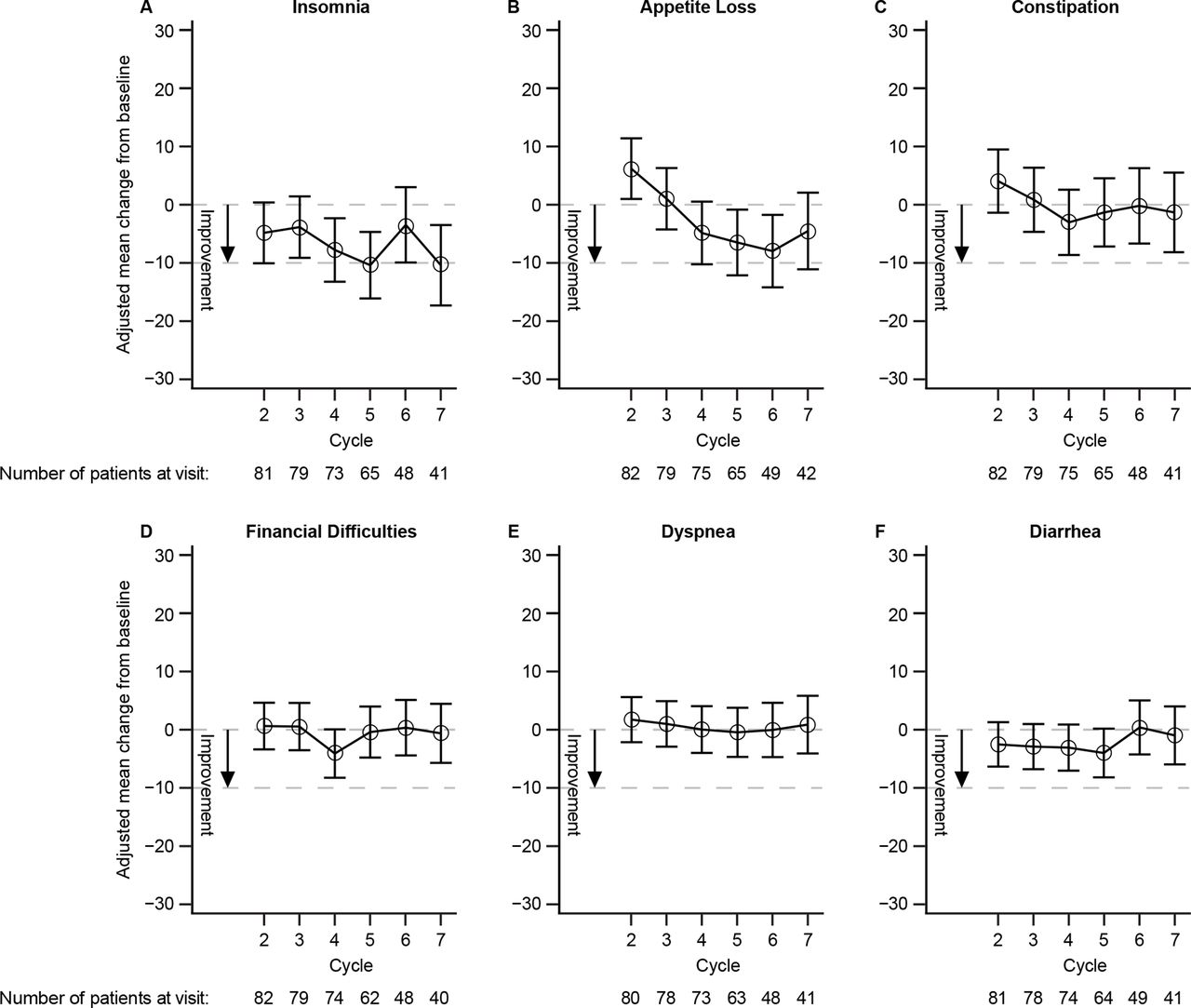
Mean change from baseline for EORTC QLQ-C30 single-item scores. EORTC QLQ-C30, European Organization for Research and Treatment of Cancer Quality of Life Questionnaire C30.
Change from Baseline by RECIST Overall Response
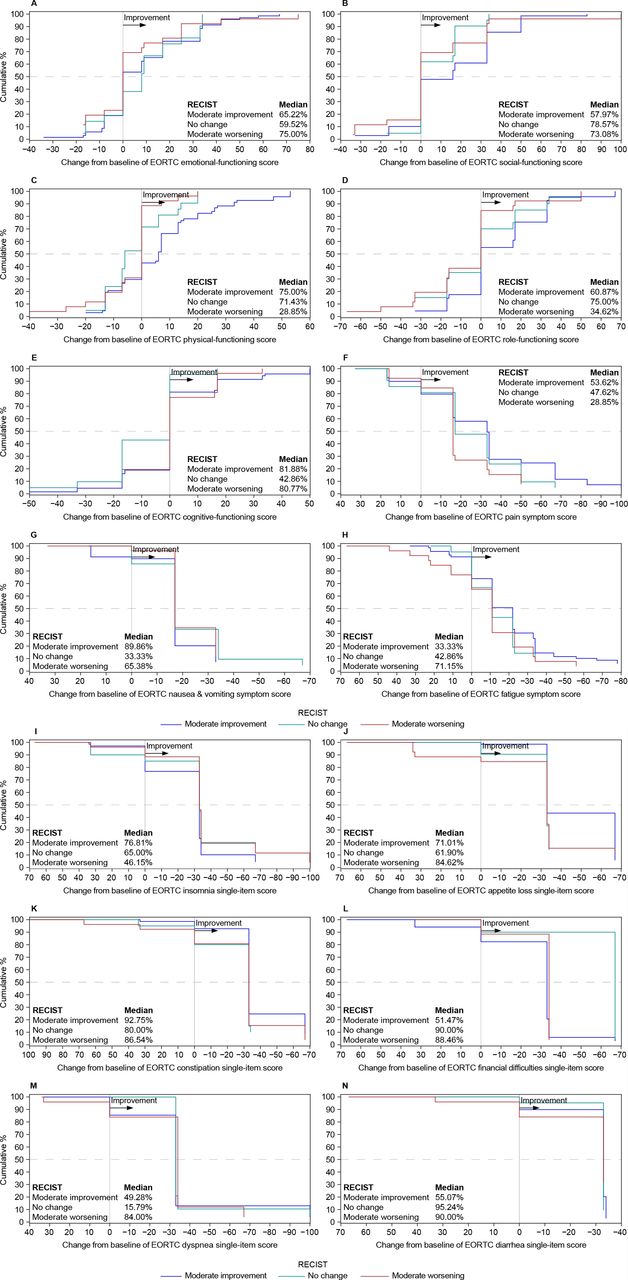
Patients were divided into sub-groups determined by their Response Evaluation Criteria in Solid Tumors (RECIST) overall responses, and the change from baseline for each measurement on the EORTC QLQ-C30 was examined (Figure 4). In patients with moderate tumor improvement per RECIST, improvement was seen across all measurements (low 33.33%, dyspnea; high 89.96%, nausea and vomiting). Patients with no change in tumor size also demonstrated improvement across all measurements (low 15.79%, dyspnea; high 95.24%, diarrhea). Improvements across all measurements were also seen in patients with moderate worsening per RECIST (low 28.85% physical functioning and pain; high 90.0% diarrhea).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cumulative distribution function of change in EORTC QLQ-C30 scores from baseline by RECIST overall response. The percent change from baseline for EORTC scores of patients experiencing one of three categories of RECIST (moderate improvement, no change, and moderate worsening). Median percentage of patients experiencing an improvement in change from baseline for EORTC score per RECIST category is indicated on each panel. EORTC QLQ-C30, European Organization for Research and Treatment of Cancer Quality of Life Questionnaire C30; RECIST, Response Evaluation Criteria in Solid Tumors.
Discussion
Summary of Main Results
Our study found that, for all disease-related symptoms and single-item scales, patient-reported outcome assessments demonstrated improvement or stability during dostarlimab treatment from cycles 2 through 7. The observations here were similar to those seen with other PD-(L)1 inhibitors. In this cohort of patients with mismatch repair-deficient/microsatellite instability-high endometrial cancer, the occurrence of 2- or 3-category worsening was seen most frequently in symptomatic gastrointestinal adverse events, although the occurrence was low throughout treatment (≤7.3%). Looking at the patient-reported outcome assessments in coordination with the safety data provides interesting insights into the patient experience during dostarlimab treatment. No grade ≥3 nausea adverse events were observed per National Cancer Institute Common Terminology Criteria for Adverse Events v4.03 (as measured by physicians), which coincides with the patient-reported outcome data showing no 3-category worsening in nausea. In contrast, for constipation one patient reported a worsening by three categories, which coincides with the single report of National Cancer Institute Common Terminology Criteria for Adverse Events grade 3 constipation (as measured by physicians). Gastrointestinal adverse events are known to occur with PD-(L)1 inhibitors, and they are seen with dostarlimab as well: nearly 16% and 13% of patients with mismatch repair-deficient endometrial cancer experienced diarrhea and nausea as treatment-related adverse events, respectively.34 The patient-reported outcome data presented here are in accordance with the gastrointestinal adverse events experienced by the patients, with more patients experiencing 2- or 3-category worsening of gastrointestinal adverse events.
Results in the Context of Published Literature
QoL research has not been sufficiently studied in endometrial cancer, and it has been inconsistently studied with regard to PD-(L)1 inhibitors.30–32 A meta-analysis of patient-reported outcome assessments in randomized controlled trials of PD-(L)1 inhibitors showed that, when compared with standard-of-care therapy, patients receiving PD-(L)1 inhibitors maintained QoL and demonstrated less worsening of symptoms.31 However, the studies in the meta-analysis did not include endometrial cancer. The Gynecologic Cancer InterGroup Symptom Benefit Working Group has indicated that endometrial cancer-specific QoL research in clinical trials is necessary to improve outcomes in women with endometrial cancer. The GARNET trial, with the high percentage of completed assessments in patients with endometrial cancer, is one of the first to address this deficiency.29
Few studies have compared patient-reported outcome data with tumor response data. However, a meta-analysis of 21 studies, consisting of 2629 adults with cancer, showed that patient-reported outcome improvements were associated with patients who had complete and partial responses to therapy and could also be seen in those with stable disease and progressive disease.35 However, patients with complete and partial responses had the largest patient-reported outcome improvements. Because of inconsistency with the patient-reported outcome assessments used and the variability of the cancer types, treatments, and durations in the meta-analysis, it is difficult to draw significant conclusions.35 In the data presented here, improvement in patient-reported outcomes was seen regardless of tumor response per RECIST. The improvement in patient-reported outcomes seen in patients with moderate tumor worsening may be consistent with other studies which have reported symptom relief in patients with progressive disease.35 Indeed, patients with progressive disease reported improvements across all symptoms measured, with larger rates of improvement in symptom measurements than in functional measurements.
Strengths and Weaknesses
The addition of patient-reported outcome assessments to this cohort (mismatch repair-deficient/microsatellite instability-high endometrial cancer) of the GARNET study provided an opportunity to obtain valuable knowledge on the QoL of patients with endometrial cancer being treated with dostarlimab. As a limitation, GARNET as a single-arm study offered no standard of care as a comparator, although data from phase III trials of dostarlimab will be able to clarify comparisons in the future.
Implications for Practice and Future Research
To date, a data gap exists in QoL research in clinical trials of endometrial cancer, particularly in those patients with advanced or recurrent endometrial cancer. With the inclusion of patient-reported outcome assessments in the GARNET trial, this study is one of the first to address this data gap to help improve the evaluation of cancer treatments for this patient population. This study begins to validate the use of patient-reported outcome assessments in endometrial cancer and encourages their future use in phase III trials of GARNET to increase understanding of QoL of patients with advanced or recurrent endometrial cancer treated with PD-(L)1 inhibitors.
Conclusions
The patient-reported outcome assessments included in this analysis suggest that treatment with dostarlimab does not impair patient functioning or QoL. This result supports the observation that most patients maintain or note improved QoL while receiving dostarlimab for the treatment of recurrent or advanced mismatch repair-deficient endometrial cancer, independent of tumor response. These data, along with the efficacy and safety profile, support the use of dostarlimab in patients with mismatch repair-deficient/microsatellite instability-high recurrent or advanced endometrial cancer. Further QoL data will be available from part 1 of the phase III RUBY trial, which will evaluate the efficacy and safety of dostarlimab in combination with carboplatin–paclitaxel in patients with recurrent or primary advanced endometrial cancer compared with carboplatin–paclitaxel alone.
Data availability statement
Data are available upon reasonable request. Anonymized individual participant data and study documents can be requested for further research from www.clinicalstudydatarequest.com.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Western Institutional Review Board (WIRB) Pr. No. 20160056. Written approval was obtained from all subjects or a legal surrogate.
Acknowledgments
We would like to thank Jennifer Hanlon (GSK, Waltham, MA, USA) for her contributions to the analysis. Writing and editorial support, funded by GSK (Waltham, MA, USA) and coordinated by Hasan Jamal of GSK, was provided by Shannon Morgan-Pelosi and Jennifer Robertson of Ashfield MedComms, an Inizio company (Middletown, CT, USA).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors RK: Conceptualization, investigation, resources, writing – original draft, writing – review and editing, visualization. CM: Conceptualization, investigation, resources, writing – original draft, writing – review and editing, visualization. AR: Conceptualization, investigation, resources, writing – original draft, writing – review and editing, visualization. SB: Conceptualization, formal analysis, resources, writing – original draft, writing – review and editing, visualization, supervision, guarantor. JH: Conceptualization, formal analysis, writing – original draft, writing – review and editing, visualization. EI: Conceptualization, methodology, validation, formal analysis, resources, investigation, resources, writing – original draft, writing – review and editing, visualization, supervision, project administration. JB: Conceptualization, investigation, resources, writing – original draft, writing – review and editing, visualization.
Funding This study (NCT02715284) was sponsored by GSK, Waltham, MA, USA.
Competing interests RK reports grants from Clovis and MSD; honoraria and consultancy fees from AstraZeneca, Basilea Pharmaceutica, Clovis, Eisai, Incyte, MSD, and PharmaMar; and personal fees from GSK. CM reports institutional grants from GSK. AR reports institutional grants from Eisai, PharmaMar, and Roche; and advisory roles at AstraZeneca, GSK, PharmaMar, and Roche. SB is an employee of GSK. JH and EI are former employees of GSK. JB reports honoraria from Olympus; consulting or advisory role at AstraZeneca, Caris, Clovis, Genentech, and GSK; and speakers’ bureau at Clovis.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.