Article Text

Statistics from Altmetric.com
Oncologic outcomes in ovarian cancer are improved by maximal cytoreduction surgical effort. In order to achieve this goal, surgeons must have adequate training with expertise in complex multi-quadrant surgery. This requires a multidisciplinary group that includes a gynecologic oncologist, gastrointestinal surgeon, urologist, hepatobiliary surgeon and, occasionally, a thoracic surgeon. The training of surgical teams with the ability to perform high complexity surgery such as those required in ovarian cancer is a worldwide challenge. European Society of Gynaecological Oncology (ESGO) guidelines for ovarian cancer surgery propose performing at least 20 or 30 cases of cytoreduction of ovarian cancer in advanced stages to be considered a center of excellence in the treatment of epithelial ovarian cancer.1
Lower- and middle-income countries face multiple barriers that limit access to appropriate care for patients with ovarian cancer, and this often leads to poor clinical and oncologic outcomes. Training and practice environments with limited experience, poor capacity to integrate multidisciplinary groups, and limited infrastructures to manage complex pathologies are part of the problem and create challenges for both the physicians and for the health system. The gynecological cancer surgeon’s training in Latin America using cadaveric models is either limited or non-existent in most countries due to a lack of suitable training laboratories and the absence of experienced faculty to train surgeons. Because of this, the first international course of surgery in advanced ovarian cancer was held in Bogotá in February 2022, along with the adaptation of the practical center infrastructure in cadaveric models in Colombia.
This course will be held annually at the CLEMI (Latin-American Center of Investigations and Training in Minimally Invasive Surgery) located in Briceño, a small town near Bogotá, Colombia. In order to implement this course, our team performs a number of tasks, including the verification of cadaveric models for adequate conditions for the course, acquisition of adequate and sufficient surgical instruments for all the participants, and the adaptation of abdominal retractors capable of performing a complete abdominal cavity exposure in an adequate and practical way— perhaps one of the critical issues creating this course, as these abdominal wall retractors are not available in most surgical centers in our country and are considered to be non-existent for students in surgery practice.
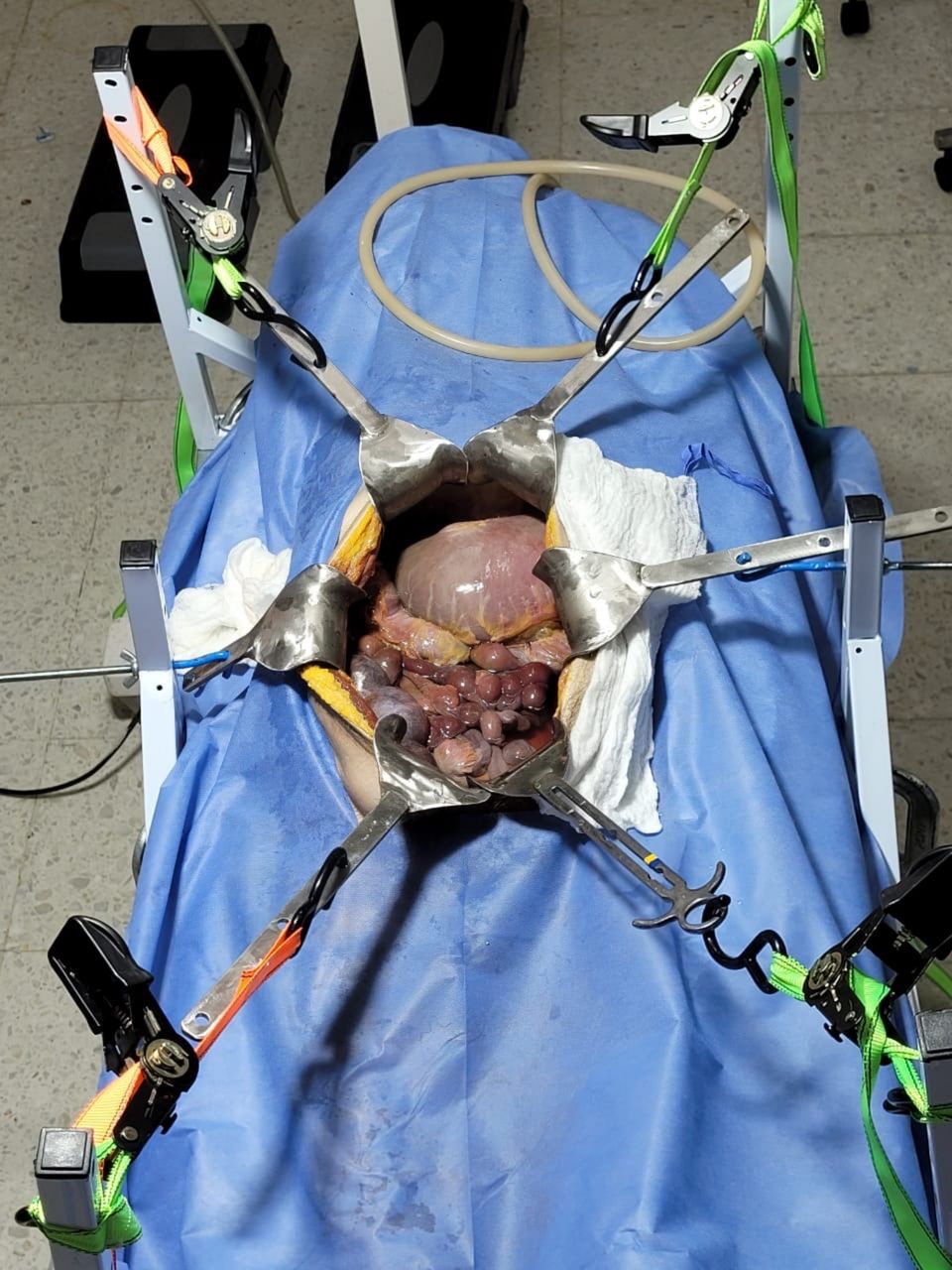
The course begins with didactic lectures, based in a hybrid way on the presentation of cases and videos supported by scientific evidence. Then, we proceed with a structured program performed using cadaveric models that develop highly complex surgical procedures (complete peritonectomy, intestinal resection, splenectomy, hepatic resection, diaphragm stripping, aortic lymphadenectomy). In this setting we use a ‘home-made’ retractor system (Figures 1 and 2). As part of the training, participants are taught how to set up this retractor to achieve the surgical objectives proposed. Each work group is made up of three gynecologic oncologists as students and two professors (one gynecologic oncologist and one oncologic surgeon). At the end of 2 days of work, the proposed goals are evaluated and participants are provided a feedback session where tips and recommendations are discussed.
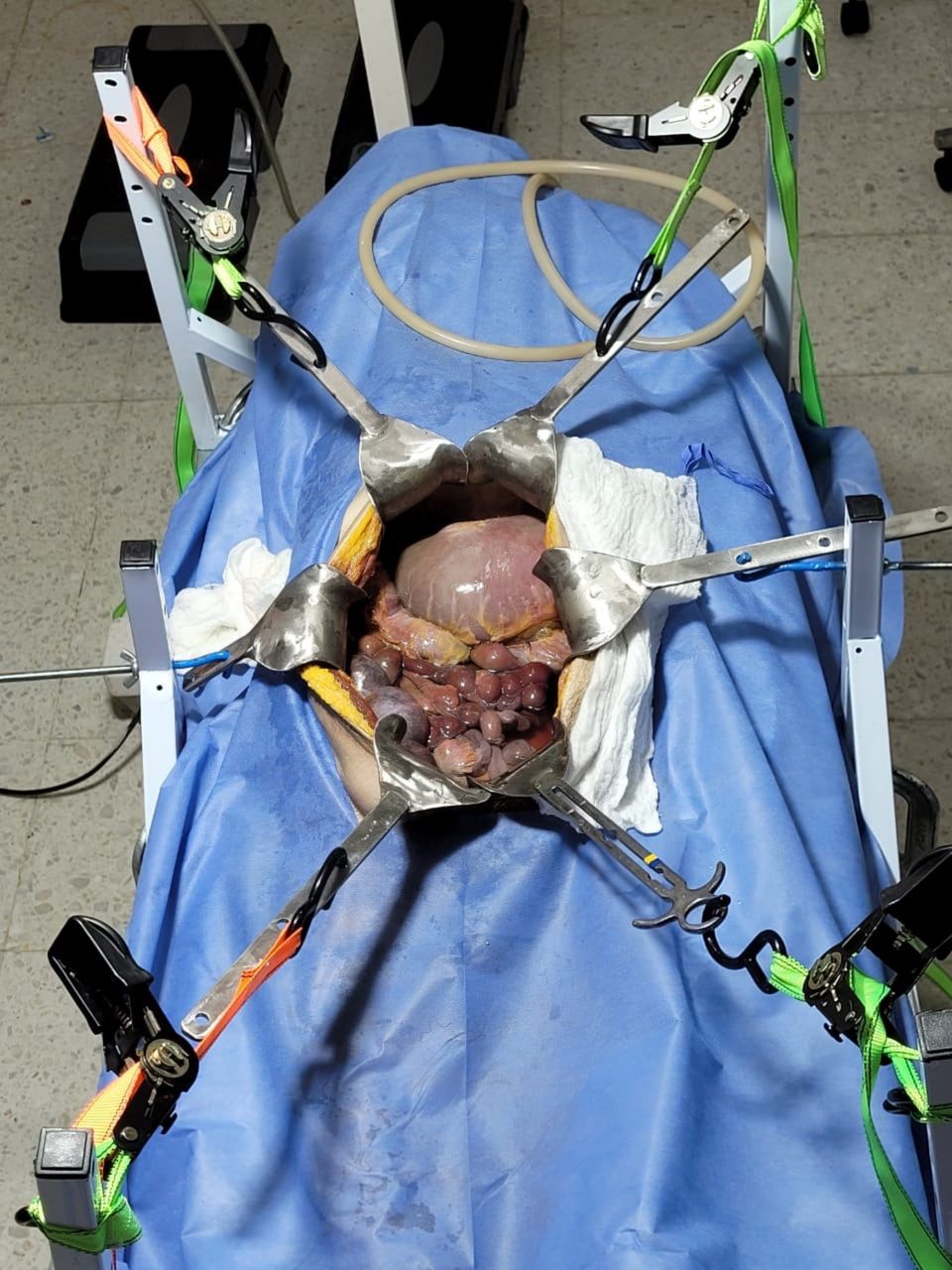
Abdominal wall retractor.

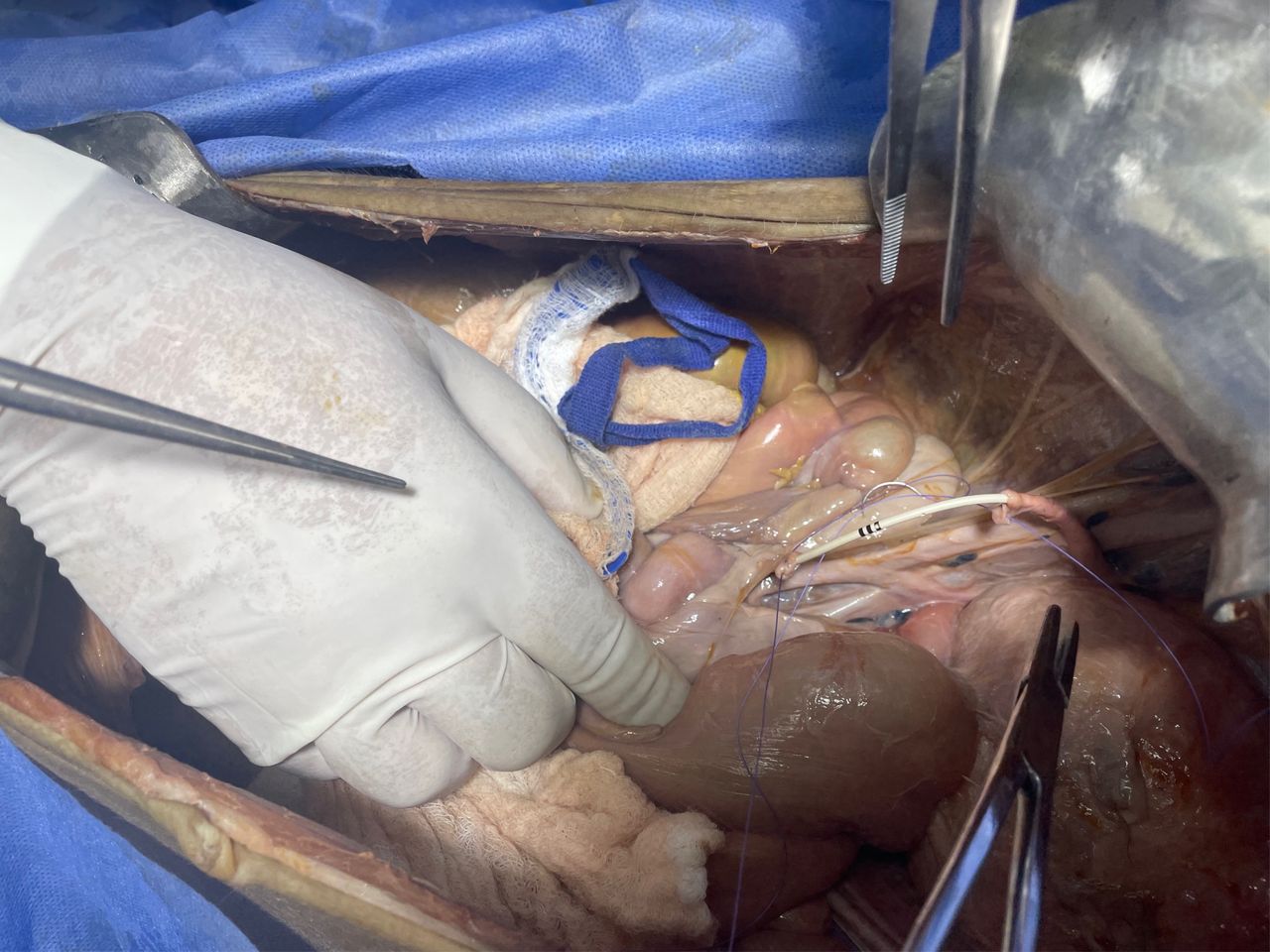
Abdominal wall retractor and abdomen exposure when performing a Boari-flap procedure.
High-quality training is feasible in low- and middle-income countries (Figure 3) for gynecologic oncology specialists and surgical oncologists. We must continue to strive in improving training and education within the confines of limited resources and look forward to the growth and expansion of our program.

{kind=link}
{kind=link}
{kind=link}
Course attendees from eight Latin-American countries.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Reference
Footnotes
Twitter @danielsanabrias
Contributors Study design: DS, RP; Data and images acquisition: DS, HA, LC, AA; Manuscript writing: DS, RP; Manuscript review: DS, RP, HA, LC, AA.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.