Article Text

Statistics from Altmetric.com
Ovarian cancer is the most lethal gynecological malignancy due to its late detection and high recurrence rate. Recurrences after 6 months of platinum based treatment may have the most benefit from secondary and tertiary cytoreductive surgery. Isolated and resectable disease is the main significant predictor of successful cytoreduction with subsequent survival benefits.1 Moreover, isolated lymphatic relapse represents the main indication of surgical treatment, improving prognosis. Localized lymph node recurrence is suitable for minimally invasive surgery, providing better perioperative and long term outcomes, but highly advanced surgical skills and experience are required. 2 3
We present the case of a 59-year-old patient with a second high grade serous epithelial ovarian cancer recurrence treated with robotic surgery. At the first diagnosis (International Federation of Gynecology and Obstetrics (FIGO) stage IIIC), the patient underwent laparoscopic cytoreduction followed by platinum based chemotherapy. The patient experienced the first right obturator lymphatic recurrence 50 months later, and laparoscopic complete debulking and systemic therapy were performed. After 12 months from the first recurrence, imaging showed an isolated lymph node relapse in the right obturator fossa with pelvic side wall involvement. A complete (no residual tumor) robotic assisted laparoscopic cytoreduction was performed, sparing the obturator nerve. No intraoperative or postoperative complications were observed. No relapse was reported after 2 years of follow-up.
{kind=link}
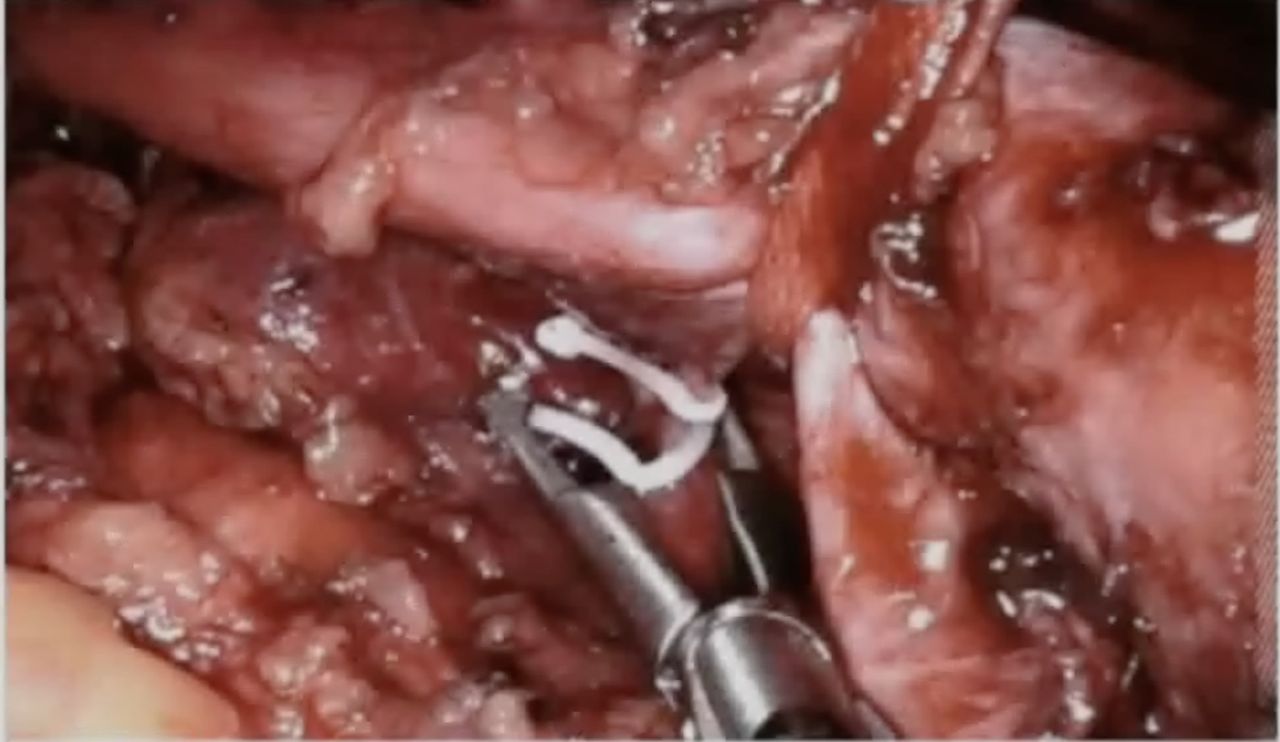
Clipping and sectioning of the superior gluteal vein to reach and resect the lymph node metastasis.
Minimally invasive surgery is a valid option for secondary cytoreduction in selected isolated ovarian cancer recurrence. Complete debulking through minimally invasive surgery is feasible and enhances the chances of a favorable result. The robotic approach represents a technological advance over traditional laparoscopy, allowing radical surgery even in a complex case of ovarian recurrence involving the pelvic side wall.4 Robotic surgery may be considered for highly selected recurrent ovarian cancer cases in referral oncological centers with extensive experience in minimally invasive surgery.
Disclaimer: this video summarises a scientific article published by BMJ Publishing Group Limited (BMJ). The content of this video has not been peer-reviewed and does not constitute medical advice. Any opinions expressed are solely those of the contributors. Viewers should be aware that professionals in the field may have different opinions. BMJ does not endorse any opinions expressed or recommendations discussed. Viewers should not use the content of the video as the basis for any medical treatment. BMJ disclaims all liability and responsibility arising from any reliance placed on the content.
Data availability statement
All data relevant to the study are included in the article.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants but in our center, institutional review board approval was not required because the study involved analysis of existing data. Informed consent was obtained from the patient for the anonymized insertion of the data regarding her treatment and oncologic outcome in our research databases. The ethic committee approved the collection of data for research purposes.
Footnotes
Contributors MCDD: conception and design of the video article, manuscript preparation, data collection, patient recruitment, and video producer and interpretation. GC: conception and design of the video article, manuscript preparation, and video analysis and interpretation. GZ: conception and design of the video article, manuscript preparation, and data collection. CR: conception and design of the study, patient recruitment, and video analysis and interpretation. GS: conception and design of the study, patient recruitment, video analysis and interpretation, and supervisor of all activities. VC: conception and design of the video article, data analysis and interpretation, patient recruitment and responsible surgeon, supervisor of all activities, and responsible for the overall content of the video article as guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.