Article Text

Statistics from Altmetric.com
Summary
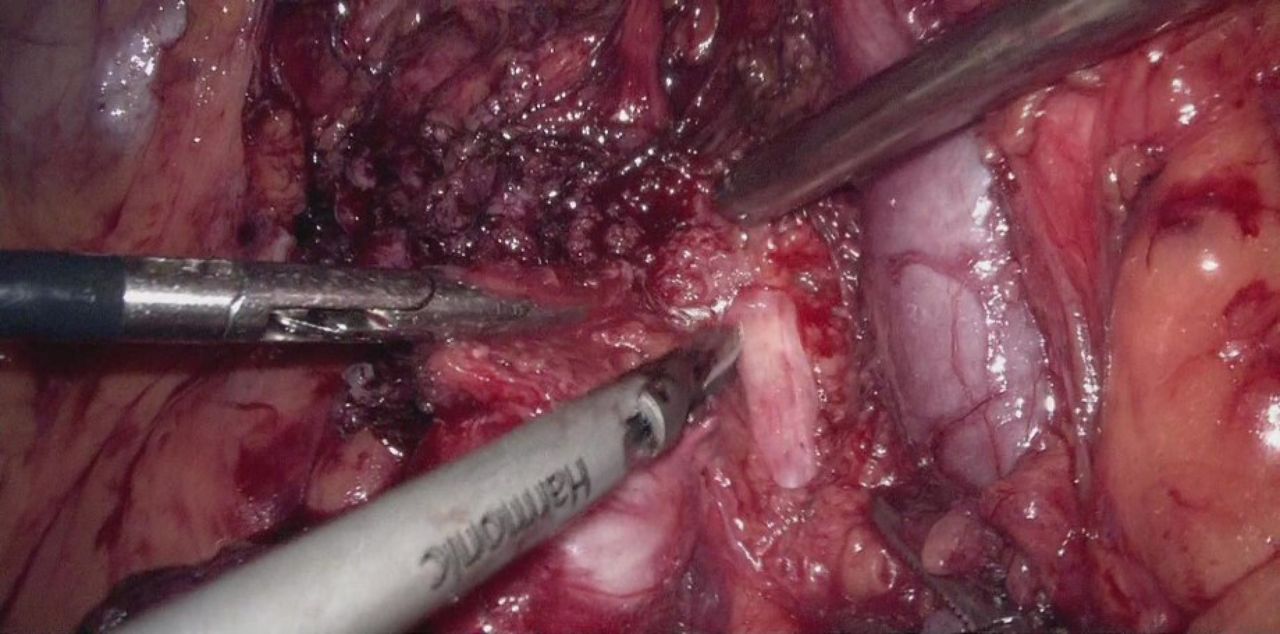
This study aimed to show laparoscopic resection of retroperitoneal leiomyosarcoma involving the right ureter, internal iliac artery, and adnexa in a patient with a history of total abdominal hysterectomy. We reported a 60-year-old woman who complained of low back pain for about 2 years. She was referred from a local clinic for a 5 cm×6 cm right adnexal mass indicated by transvaginal ultrasound. Her serum cancer antigen 125 level was in the normal range. PET/CT suggested a 5.2c m×4.5 cm right adnexal mass and showed no evidence of metastatic diseases. She received total abdominal hysterectomy because of leiomyoma 11 years previously and right nephrectomy because of non-functioning severe hydronephrotic kidney 6 months ago before her admission to our hospital. A diagnosis of pelvic malignancy was suspected, and laparoscopic resection was scheduled. The procedure began with the release of the bowels from the right adnexa and side wall peritoneum. It seemed that it was a bilobed mass involving both the intraperitoneal and the retroperitoneal region. We removed the right adnexa and collected it in a disposable pocket. Spindle cell tumor was diagnosed and there was insufficient evidence of malignancy by frozen section evaluation. We continued to dissect the remaining retroperitoneal mass. The key steps of the procedure are summarized in the video. The final pathologic report showed leiomyosarcoma involving the right ureter, internal iliac artery, and ovary. The patient received six courses of post-operative gemcitabine/docetaxel combination therapy. She was still in complete remission 6 months after surgery. Laparoscopic resection of retroperitoneal leiomyosarcoma from the obturator fossa was achieved successfully in a logical way (Online Supplemental Tables 1, 2). The critical point of the procedure is to have a good knowledge of the key anatomic landmarks of the pelvis.1
Supplemental material
Supplemental material

{kind=link}
Laparoscopic resection of retroperitoneal leiomyosarcoma.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the institutional review board of the Obstetrics and Gynecology Hospital of Fudan University(approved No.2022-13, approved date January 24, 2022) Participants gave informed consent to participate in the study before taking part.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
JuL and JiL contributed equally.
Contributors Conception and design: JuL, WJ. Collection and assembly of data: JuL, JiL, WJ. Data analysis and interpretation: JuL, JiL, WJ. Manuscript writing: JuL, JiL. Final approval of manuscript: JuL, JiL, WJ. Author acting as guarantor: WJ.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.