Article Text

Statistics from Altmetric.com
Even if molecular biomarkers that are impacting clinical practice in gynecologic oncology are limited, our community is living in the precision medicine era where the number of patients undergoing tumor genomic profiling is increasing, as is the number of new drug approval for cancers with specific genetic alterations. In this complex scenario, molecular data must be interpreted on a case-by-case basis, and the presence of molecular tumor boards in leading the decision-making process are crucial.
In fact, molecular tumor boards can identify possible therapeutic strategies based on tumor genomic alteration in patients for which the effectiveness of standard therapies is suboptimal or a standard approach does not exist. On the other hand, molecular tumor boards can avoid the use of anticancer drugs with an insufficient level of evidence, limiting unnecessary adverse effects and unjustified costs for the public healthcare system. Moreover, molecular tumor boards can play a pivotal role in the spreading of new concepts of cancer genomics, flattening the learning curve of precision medicine, making clinicians more comfortable with molecular concepts, like allelic fraction, tumor molecular drivers, and pathogenic versus non-pathogenic genetic variants. Notwithstanding the importance of molecular tumor boards is recognized and many efforts have been made to implement this tool in high volume cancer centers, limitations due to the absence of molecular tumor boards in general rural hospitals and geographical barriers are undermining the access of clinicians to these facilities. Furthermore, routine molecular tumor boards need to consider sub-specializations in oncology; thus, sub-specialists should attend the selective board, a factor that makes molecular tumor board organization more elaborate for a single institution.
To overcome the limits of conventional molecular tumor boards taking advantage of the yet established network between the gynecologic oncology community in Italy, the MITO group has recently inaugured the virtual molecular tumor boards by MITO, a fully virtual and nationwide molecular tumor board focused on gynecologic cancers. The project has been matched with the GYNecological cancers GEnetic profile Registry (GYNGER), an observational, retrospective–prospective clinical study aimed at collecting clinical and molecular data from patients, with a focus on those suffering from rare gynecological cancers.
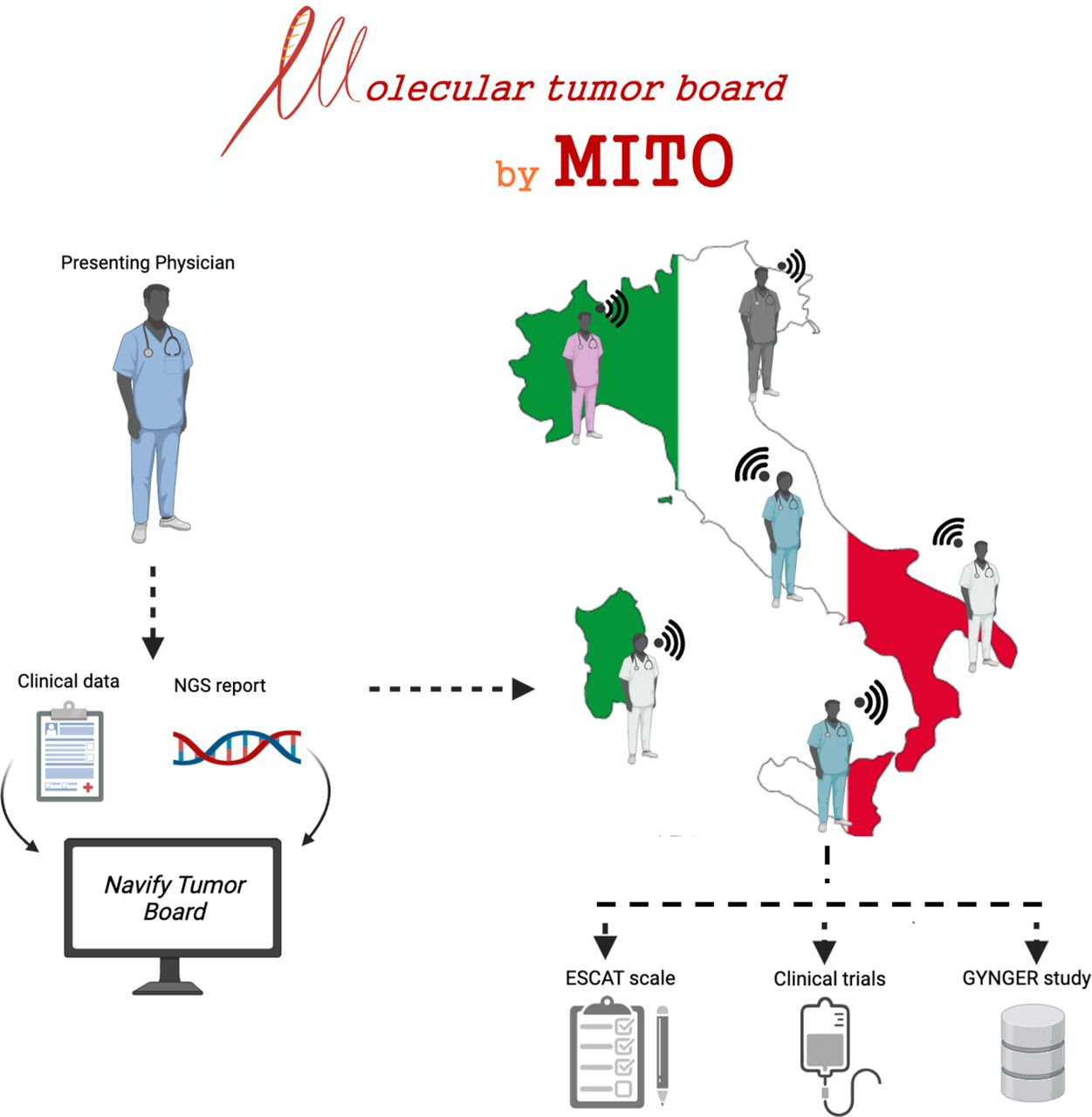
The molecular tumor board by MITO is reserved for the MITO group’s members. Launched in June 2021, to date the project totals approximately 50 fellows, including medical oncologists, gynecologists, pathologists, molecular biologists, geneticists, and clinical study coordinators. Virtual meetings are scheduled every 2 weeks on the videoconferencing platform Zoom, which the invited-only members can access via computer or mobile device. Until 72 hours before the planned meeting, members can submit anonymized clinical cases using the platform Navify Tumor Board (NTB, Roche Molecular Systems, Santa Clara, CA). All members are allowed to enter the Navify Tumor Board to study and prepare clinical case(s) days before the scheduled meeting. When a case is discussed for molecular data interpretation, the board’s final decision can be the ranking of a molecular alteration and its matched drug using the ESMO Scale for Clinical Actionability of molecular Targets (ESCAT), the patient’s referral to a biomarker-driven trial or expanded access program active in Italy (Table 1), and finally, the patient’s enrollment in the GYNGER study (Figure 1).
Main tumor agnostic/biomarker driven clinical trials based on NGS analysis active in Italy (December 2021)
{kind=link}
Data flow and organization of the virtual molecular tumor board by MITO. ESCAT, ESMO scale for clinical actionability of molecular targets; GYNGER, GYNecological cancers GEnetic profile Registry; NGS, next generation sequencing.
Ethics statements
Patient consent for publication
Ethics approval
This study does not involve human participants.
Footnotes
Twitter @Barto_Med
Contributors Conceptualization, MB and SP; writing—original draft preparation, MB; writing—review and editing, all authors; supervision, SP; funding acquisition, SP. All authors have read and agreed to the published version of the manuscript.
Funding The National Cancer Institute Fondazione G. Pascale has received Navify Tumor Board (Roche Molecular Systems, Santa Clara, CA) free of charge.
Competing interests This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. Others potential conflicts of interest outside the submitted work: SP has received honoraria from AZ, MSD, Roche, GSK, Pfizer, Clovis Oncology, Pharmamar and research funding from MSD, Roche, AZ, Pfizer. GS has received grant/research support from MSD Italia S.r.l., consultant for TESARO Bio Italy S.r.l, speakers bureau/honoraria from Clovis Oncology Italy S.r.l, consultant from Johnson & Johnson. FP reports grants from AstraZeneca, grants, personal fees and other from Roche, personal fees and other from Eli Lilly, personal fees from Amgen, personal fees from Ipsen, personal fees from MSD, personal fees from Takeda, grants and other from Eisai, other from Novartis and Pfizer. DL has declared from Amgen, other, personal, consultancy; from AstraZeneca, Advisory Board, personal, invited speakers, Principal Investigator; from Clovis Oncology, invited speaker, personal, institutional, financial interest, grant; from GSK, Advisory Board, personal, invited Speaker, Principal Investigator; from MSD, Advisory Board, personal, invited speakers, funding, institutional, financial interest; from Genmab, Coordinating PI, institutional, financial interest. The other authors have nothing to disclose.
Provenance and peer review Commissioned; internally peer reviewed.