Article Text

Abstract
Objective To assess the strategy and value of centralized surveillance of hydatidiform mole at a regional hospital in China and to investigate the necessity of prophylactic chemotherapy for high-risk complete hydatidiform mole.
Methods Between February 2013 and February 2020, all women with hydatidiform mole in Dalian Women’s and Children’s Medical Center (Group) were registered for surveillance and treatment when indicated. Women with complete hydatidiform mole were categorized into low-risk and high-risk groups according to the criteria from Song Hongzhao’s trophoblastic neoplasia. Outcomes and treatments were analyzed retrospectively.
Results In total, 703 women with hydatidiform mole were registered for surveillance with a follow-up rate of 97.9% (688/703). 680 women were enrolled and 52 (7.6%) developed post-molar gestational trophoblastic neoplasia, all with low-risk International Federation of Gynecology and Obstetrics (FIGO) scores 0–5. Post-molar gestational trophoblastic neoplasia was diagnosed in 12.3% (51/413) of patients with complete hydatidiform moles and 0.4% (1/263) of patients were diagnosed with partial hydatidiform moles (χ2=32.415, p<0.001). Post-molar gestational trophoblastic neoplasia was diagnosed in 27.7% (28/101) of the high-risk complete hydatidiform mole group and in 7.4% (23/312) of the low-risk complete hydatidiform mole group (χ2=29.196, p<0.001). No difference in the pre-treatment assessments of patients with post-molar gestational trophoblastic neoplasia was found between the low-risk and high-risk complete hydatidiform mole groups (all p>0.05). All 52 patients with post-molar gestational trophoblastic neoplasia were cured, with a complete response rate of 61.2% (30/49) with first-line single-agent chemotherapy.
Conclusions A centralized hydatidiform mole surveillance program is feasible and effective and may improve the prognosis of patients with post-molar gestational trophoblastic neoplasia. Prophylactic chemotherapy is not recommended for women with high-risk complete hydatidiform mole with adequate surveillance.
- hydatidiform mole
Data availability statement
Data are available upon reasonable request. The data that supporting the findings of this study are available from the corresponding author upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, an indication of whether changes were made, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
HIGHLIGHTS
An effective gestational trophoblastic disease surveillance program was developed in a regional hospital in China.
The incidence of post-molar gestational trophoblastic neoplasia was 7.6%, with a 100% cure rate.
Prophylactic chemotherapy is not recommended for women with high-risk complete hydatidiform mole with adequate surveillance.
Introduction
Hydatidiform mole is a type of abnormal pregnancy and the most common form of gestational trophoblastic disease. Hydatidiform moles can be subdivided into complete hydatidiform mole and partial hydatidiform mole based on their histopathology and karyotype. Most women with hydatidiform mole are cured by suction evacuation and curettage, but some may develop post-molar gestational trophoblastic neoplasia, with rates of 15.0% for complete hydatidiform mole and 0.5–1.0% for partial hydatidiform mole.1
Women with high-risk hydatidiform mole, who are at a high risk for post-molar gestational trophoblastic neoplasia, typically have at least one of the following characteristics: age >40 years, pre-evacuation human chorionic gonadotropin (hCG) level >100 000 IU/L, excessive uterine enlargement, or theca lutein cysts >6 cm.2 Approximately 30–50% of high-risk hydatidiform mole cases progress to gestational trophoblastic neoplasia.3–5
Centralized care is needed for the optimal management of gestational trophoblastic disease.6 The UK model of centralized care for gestational trophoblastic disease has been successfully implemented since 1973 and is internationally recognized.7 However, this work lags behind in China. Since it may be difficult to establish nationwide centralized care for gestational trophoblastic disease in China, we chose to implement this program at a regional hospital. We describe our 7 years of experience with centralized surveillance of hydatidiform mole. This study aimed to assess the value of the centralized surveillance of hydatidiform mole at a regional hospital in China and to evaluate the necessity of prophylactic chemotherapy for high-risk complete hydatidiform mole.
Methods
Model of Centralized Surveillance of Hydatidiform Mole
Centralized surveillance of hydatidiform mole has been implemented in Dalian Women’s and Children’s Medical Center (Group) since February 2013. Ultrasound examination is performed routinely in early pregnancy. If ultrasound examination suggests hydatidiform mole or early pregnancy failure, uterine evacuation is performed and pathological examination is recommended for all products of conception. Pathological evaluation of hydatidiform mole is based on both morphology and p57Kip2 immunostaining combined with the assessment of ploidy by fluorescence in situ hybridization if necessary. Once the diagnosis of hydatidiform mole is confirmed, a pathological report is submitted to the gestational trophoblastic disease clinic.
The gestational trophoblastic disease clinic was established for centralized surveillance of hydatidiform mole, consultation of patients with suspected gestational trophoblastic neoplasia, and long-term surveillance of patients with gestational trophoblastic neoplasia, with a clinical nurse assisting in surveillance work. Women with hydatidiform mole are registered for centralized surveillance at their first visit in the gestational trophoblastic disease clinic, usually 1–2 weeks after evacuation. Clinical features, including maternal age, gravidity, parity, body mass index, history of hydatidiform mole, gestational age, main presenting symptoms, uterine size at evacuation, pre-evacuation ultrasound examinations, pre-evacuation human chorionic gonadotropin (hCG) level and histopathological diagnosis are requested for registration and recorded. Pelvic examination and transvaginal color Doppler ultrasonography are performed routinely for 1–2 weeks after evacuation. A second uterine curettage is not performed routinely unless ultrasound examination indicates intra-uterine residual hydatidiform mole.
Follow-up hCG monitoring of all registered women with hydatidiform mole is performed according to the UK hCG surveillance guidelines.1 If there is a rise or plateau (±10%) in the serum hCG level and irregular vaginal bleeding during surveillance, a second pregnancy or residual hydatidiform mole is excluded and serum hCG concentrations are then monitored weekly. Post-molar gestational trophoblastic neoplasia is diagnosed according to the International Federation of Gynecology and Obstetrics (FIGO) 2000 criteria.8
Patients who develop post-molar gestational trophoblastic neoplasia during surveillance are treated promptly at the Department of Gynecology Oncology; after treatment, they are followed regularly at the gestational trophoblastic disease clinic. Patients with hydatidiform mole with poor outcomes in previous pregnancies are referred to the reproductive clinic of our hospital for counseling and related examinations before planning a subsequent pregnancy.
Study Design and Population
All women with hydatidiform mole were registered for centralized surveillance between February 2013 and February 2020, excluding those who were suspected of having gestational trophoblastic neoplasia and referred for treatment from other hospitals. Special types of hydatidiform mole, including heterotopic hydatidiform mole and complete hydatidiform mole co-existing with a normal fetus, were also excluded. Women with complete hydatidiform mole were categorized into low-risk and high-risk groups according to the criteria of Song Hongzhao’s trophoblastic neoplasia.9 Patients with high-risk complete hydatidiform mole had at least one of the following characteristics: (1) maternal age >40 years; (2) excessive uterine enlargement for presumed gestational age (ie, >4 weeks of normal gestational age); (3) initial serum hCG level >500 000 IU/L; (4) theca lutein cysts >6 cm in diameter; or (5) a history of previous hydatidiform mole.
All patients with post-molar gestational trophoblastic neoplasia underwent a comprehensive evaluation prior to initial treatment, including a general physical examination, measurement of the serum hCG level, chest computed tomography (CT), and abdominopelvic Doppler ultrasound. If the lesion diameter was >1 cm on chest CT, brain magnetic resonance imaging (MRI) and CT scans of the abdomen and pelvis were indicated to exclude more widespread disease.
The study protocol was approved by the Ethics Committee of Dalian Women’s and Children’s Medical Center (Group) (approval no. 2017032). All patients were informed of the study details and signed informed consent forms.
Treatment Protocols
For patients with lesions confined to the uterus and without fertility requirements, hysterectomy could be considered and serum hCG levels were checked weekly until normalization after surgery. The first-line chemotherapy for patients with post-molar gestational trophoblastic neoplasia with a FIGO score of ≤6 was a single-agent regimen, including 8-day intravenous 5-fluorouracil, 5-day intravenous actinomycin D, 8-day intramuscular methotrexate with folinic acid, or biweekly pulsed intravenous actinomycin D. The fluorouracil regimen has been abandoned since 2015 because of inconvenience in terms of its use, such as 8 days per course of treatment, 8 hours per day of continuous intravenous drip, and side effects such as diarrhea and stomatitis. Due to the side effects of 5-day intravenous actinomycin D such as nausea, vomiting, stomatitis, alopecia, and myelosuppression, we switched to the 8-day intramuscular methotrexate with folinic acid regimen beginning in January 2015 and to the biweekly pulsed intravenous actinomycin D regimen beginning in June 2016. Patients resistant to the 8-day intramuscular methotrexate with folinic acid regimen were switched to actinomycin D or first-line combination regimens including floxuridine, actinomycin D, and vincristine; etoposide, methotrexate, actinomycin D, cyclophosphamide, and vincristine; or etoposide combined with actinomycin D. For patients with high-risk FIGO scores (≥7), the first-line treatment was the floxuridine, actinomycin D, and vincristine or etoposide, methotrexate, actinomycin D, cyclophosphamide, and vincristine regimen. Patients developing resistance to the first-line combination regimens were switched to floxuridine, actinomycin D, etoposide, and vincristine or paclitaxel and etoposide alternating with paclitaxel and cisplatin chemotherapy regimens.
During treatment, patients had their serum hCG levels measured weekly. Drug resistance was defined as stable or increased hCG over two courses of treatment and the patient was switched to more intensive therapy. Remission was achieved when hCG levels reached and remained normal for at least three consecutive weeks. After achieving a normal hCG level, 2–3 courses of consolidation therapy were administered according to the patients' risk scores. After the last course of chemotherapy, the levels of hCG were checked monthly for at least 1 year. Relapse was defined as increasing and abnormal hCG test results with or without invasive lesions after remission. The final follow-up was performed in August 2020.
Statistical Methods
Statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS) V.22.0 software (SPSS, Chicago, Illinois, USA). Count data are expressed as rates and were compared using the non-parametric χ2 test. Measurement data conforming to a normal distribution are expressed as mean±SD and were compared using the t-test; otherwise, measurement data are expressed as median values and were compared using the Mann–Whitney U test. Differences were statistically significant at p<0.05.
Results
A total of 703 women with hydatidiform mole were diagnosed and registered at Dalian Women’s and Children’s Medical Center (Group). Fifteen women (nine with complete hydatidiform mole and six with partial hydatidiform mole) were lost to follow-up, and the follow-up rate was 97.9% (688/703). Among the eight women who were excluded from the study, three had a complete hydatidiform mole co-existing with a normal fetus, three had a complete hydatidiform mole and accidentally became pregnant before the hCG level decreased to normal, one chose to receive prophylactic chemotherapy at another hospital, and one had a right tubal interstitial complete hydatidiform mole. The remaining 680 women, including 413 (60.7%) with complete hydatidiform mole, 263 (38.7%) with partial hydatidiform mole, and four (0.6%) with unclassified hydatidiform mole, were included in the study and completed their follow-up without prophylactic chemotherapy (Figure 1). The mean age was 31.7±6.8 years (range 16–55) and 247 (36.3%) were prima gravidas. Of the 680 patients, 52 (7.6%) developed post-molar gestational trophoblastic neoplasia and their median age was 32 years (range 19–53). Post-molar gestational trophoblastic neoplasia was diagnosed in 12.3% (51/413) of patients with complete hydatidiform moles and in 0.4% (1/263) of patients with partial hydatidiform moles, with a significant difference between complete hydatidiform moles and partial hydatidiform moles (χ2=32.415, p<0.001). Fifty-two patients with post-molar gestational trophoblastic neoplasia had a low-risk FIGO score (0–5), with 50 (96.2%) having a score <5 (Table 1). Thirty-five patients were diagnosed with FIGO stage III according to the results of chest CT scans, with seven patients having a FIGO score of 0 and lung micrometastases.
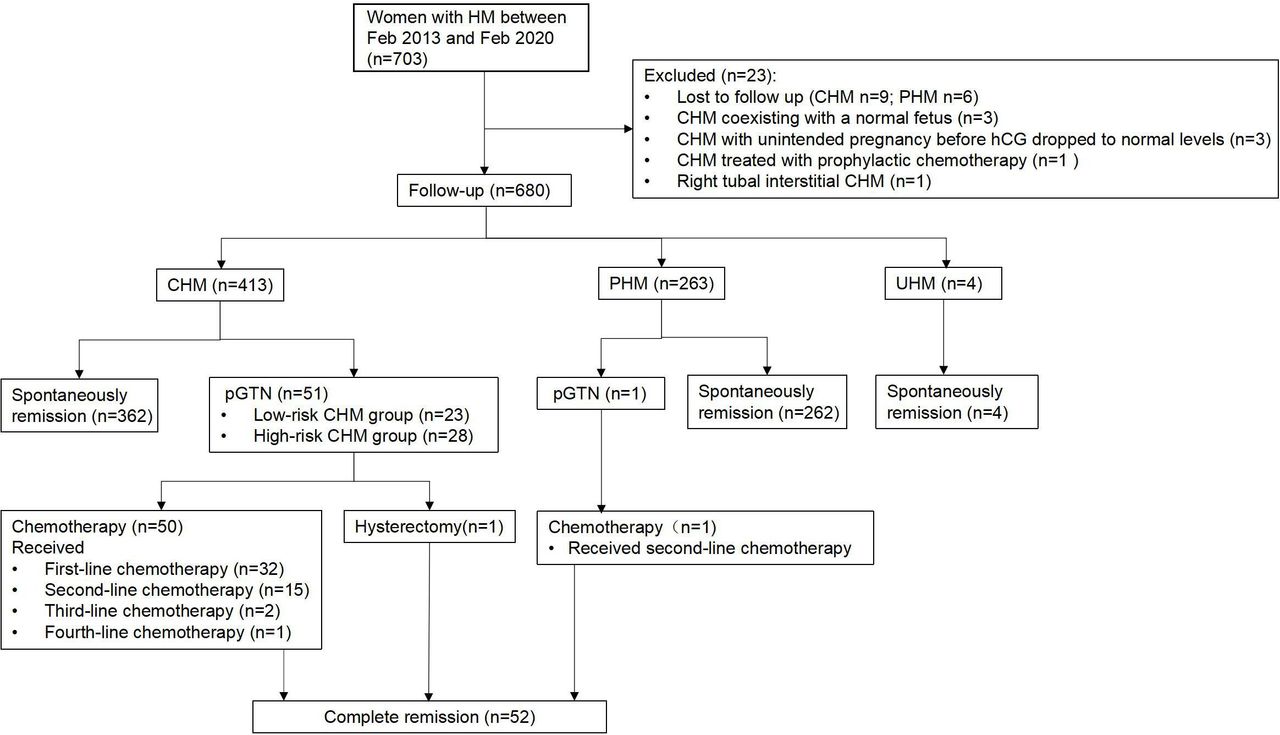
{kind=link}
Flowchart of the outcomes of women with hydatidiform mole. CHM, complete hydatidiform mole; HM, hydatidiform mole; pGTN, post-molar gestational trophoblastic neoplasia; PHM, partial hydatidiform mole; UHM, unclassified hydatidiform mole.
International Federation of Gynecology and Obstetrics (FIGO) prognostic score analysis of the 52 patients with post-molar gestational trophoblastic neoplasia in different FIGO anatomical stages
According to Song Hongzhao’s trophoblastic neoplasia, 101 (24.5%, 101/413) women with complete hydatidiform mole were classified into the high-risk group with one or more risk factors as follows: (1) age >40 years (n=59); (2) excessive uterine enlargement for presumed gestational age (n=18); (3) initial serum hCG level >500 000 IU/L (n=48); (4) theca lutein cysts >6 cm in diameter (n=9); and (5) recurrent hydatidiform mole (n=9). In total, 86, eight, and seven women had one, two, and three high-risk factors, respectively, and 312 women without risk factors were classified into the low-risk complete hydatidiform mole group. Twenty-eight (28/101, 27.7%) and 23 (23/312, 7.4%) women developed post-molar gestational trophoblastic neoplasia in the high-risk and low-risk complete hydatidiform mole groups, respectively. The incidence of post-molar gestational trophoblastic neoplasia in the high-risk complete hydatidiform mole group was significantly higher than that in both the overall complete hydatidiform mole group (χ2=14.747, p<0.001) and low-risk complete hydatidiform mole group (χ2=29.196, p<0.001). The incidence of post-molar gestational trophoblastic neoplasia in the low-risk complete hydatidiform mole group was significantly lower than that in the overall complete hydatidiform mole group (χ2=4.803, p=0.028). A comparison of the pre-treatment assessment of patients with post-molar gestational trophoblastic neoplasia in the low-risk and high-risk complete hydatidiform mole groups showed there was no significant difference in the interval from the end of the index pregnancy to treatment (p=0.84), pre-treatment serum hCG level (p=0.31), FIGO anatomical staging (p=0.49), or FIGO score (p=0.06) (Table 2).
Comparison of the pre-treatment assessment of patients with post-molar gestational trophoblastic neoplasia in low-risk and high-risk complete hydatidiform mole groups
Of the 52 patients with post-molar gestational trophoblastic neoplasia, 51 (98%) were cured by chemotherapy alone and one was cured by hysterectomy. The patient aged 53 years diagnosed with FIGO stage I with a score of 3 had no wish for fertility and requested a hysterectomy, and her serum hCG spontaneously fell to normal after surgery. The chemotherapy regimens and outcomes for the 51 patients with post-molar gestational trophoblastic neoplasia who received chemotherapy alone, including one following partial hydatidiform mole and 50 following complete hydatidiform mole, are shown in Table 3.
Overall treatment outcomes of the 51 patients with post-molar gestational trophoblastic neoplasia treated with chemotherapy
Two patients diagnosed with FIGO stage III with a score of 3 and FIGO stage III with a score of 5, respectively, requested first-line combination chemotherapy with floxuridine, actinomycin D, and vincristine due to concerns about resistance to single-agent chemotherapy and were cured. Forty-nine patients commenced single-agent chemotherapy including 8-day intravenous 5-fluorouracil (n=3), 5-day intravenous actinomycin D (n=15), 8-day intramuscular methotrexate with folinic acid (n=21), and biweekly pulsed intravenous actinomycin D (n=10) treatments, producing an overall successful treatment rate of 61.2% (30/49). Subsequently, 19 patients needed second-line chemotherapy. Eight patients resistant to the 8-day intramuscular methotrexate with folinic acid were switched to biweekly pulsed intravenous actinomycin D, seven of whom achieved complete remission. Altogether, nine patients were cured by second-line multi-agent chemotherapy, including etoposide +actinomycin D (n=2), etoposide, methotrexate, actinomycin D, cyclophosphamide, and vincristine (n=4), and floxuridine, actinomycin D, and vincristine (n=3). Three patients received third-line treatment with etoposide, methotrexate, actinomycin D, cyclophosphamide, and vincristine, of whom two achieved complete remission and one was cured by a further treatment change to floxuridine, actinomycin D, etoposide, and vincristine. There were no serious adverse events or deaths associated with chemotherapy.
After treatment, all the patients with post-molar gestational trophoblastic neoplasia were followed up regularly and survived without relapse. Their median follow-up time was 51.7 months (2.7–88.2 months). Of the 18 patients with pregnancy intentions, 13 had subsequent pregnancies and successful full-term deliveries.
Discussion
Summary of Main Results
All 52 patients with post-molar gestational trophoblastic neoplasia were cured, with a complete response rate of 61.2% to first-line single-agent chemotherapy. No difference in the pre-treatment assessments of patients with post-molar gestational trophoblastic neoplasia was found between the low-risk and high-risk complete hydatidiform mole groups (all p>0.05).
Results in the Context of Published Literature
Centralized care is needed for optimal management of rare diseases such as gestational trophoblastic disease. The UK Registration Scheme for hydatidiform mole has made remarkable achievements in gestational trophoblastic disease management. The UK owns the world’s largest gestational trophoblastic disease database, with more than 50 000 patients with gestational trophoblastic disease registered. Ninety-four percent of patients with post-molar gestational trophoblastic neoplasia had a low-risk FIGO score, and the cure rate was 100%.10 Dalian City is a medium-sized city in China with a population of approximately 6 million. Our hospital covers all of Dalian City and covers the diagnosis and treatment of patients with gestational trophoblastic disease in the region.
Based on the experience of the UK, we have developed an effective gestational trophoblastic disease surveillance program in our regional hospital. There are three key points in the implementation of centralized management of hydatidiform mole. The first is hydatidiform mole diagnosis, which depends on pathological examination. To reduce missed hydatidiform mole diagnoses, all products of conception from non-viable pregnancies should undergo histological examination.11 The second is that the set-up of the gestational trophoblastic disease clinic has effectively addressed the concentration of women with hydatidiform mole; and the third is the effective surveillance of women with hydatidiform mole. Education and communication—namely, alleviating patient anxiety about the disease and increasing patient awareness of the importance of follow-up and strict contraception during surveillance—are essential for improving patient compliance. To help patients acquire relevant information, we provide both patient information websites and telephone counseling services. To reduce the follow-up burden on patients, we adopted the UK hydatidiform mole hCG surveillance protocol, which has been shown to be safe and effective.12 hCG testing is not free but is affordable for patients, with a price of $6.5 (42¥) for each test. Patients can choose the nearest hospital for hCG testing and report the results by telephone, and they will be asked to return for further assessment if the results are abnormal. If a patient’s follow-up is interrupted for more than 4 weeks, our clinical nurse will call to remind her about the surveillance. In other words, for our patients' convenience, we tried our best to motivate them to complete the follow-up and our follow-up rate was 97.9% (688/703).
In our study, the risk of malignant transformation was increased in patients with high-risk complete hydatidiform mole while these risk factors did not affect the prognosis in patients with post-molar gestational trophoblastic neoplasia with prompt diagnosis and treatment. Our study provides evidence that prophylactic chemotherapy is not necessary for patients with high-risk complete hydatidiform mole with adequate hCG follow-up, which is consistent with a recent Cochrane review.13
Strengths and Weaknesses
A major strength of the present study was the simplicity of the centralized gestational trophoblastic disease management model and the high follow-up rate. Since there is no consensus on the optimal single-agent regimen in patients with low-risk gestational trophoblastic neoplasia, we have been improving our treatment strategy and the two regimens currently in use are 8-day intramuscular methotrexate with folinic acid and biweekly pulsed intravenous actinomycin D. Since September 2020 we have participated in a randomized clinical trial (NCT04562558; 8-day intramuscular methotrexate with folinic acid vs biweekly pulsed intravenous actinomycin D) initiated by Peking Union Medical College Hospital, which aims to provide high-certainty evidence of the optimal single-agent regimen for Asian patients with low-risk gestational trophoblastic neoplasia (score 0–4).
Implications for Practice and Future Research
Our work is performed on a hospital basis, making it easy for other regions to learn from our program. Based on the establishment of regional gestational trophoblastic disease centers, the cooperation of multiple centers will promote the standardized diagnosis and treatment of gestational trophoblastic disease and benefit the majority of patients with gestational trophoblastic disease in China.
Conclusions
The centralized hydatidiform mole surveillance program is feasible and effective at our regional hospital in China and has resulted in a 97.9% follow-up rate and a 100% cure rate for post-molar gestational trophoblastic neoplasia. Prophylactic chemotherapy is not recommended for women with high-risk complete hydatidiform mole with adequate surveillance.
Data availability statement
Data are available upon reasonable request. The data that supporting the findings of this study are available from the corresponding author upon reasonable request.
Ethics statements
Patient consent for publication
Acknowledgments
The authors thank Michael J Seckl from the Gestational Trophoblastic Neoplasia Screening and Treatment Center, Charing Cross Hospital, Imperial College, London, for guidance on the centralized care of gestational trophoblastic disease.
Footnotes
Contributors LJ and YX contributed to the study conception and design, drafting of the manuscript and analysis and interpretation of the data. LJ, YW, JJ, XW, WZ and CZ contributed to the acquisition of the data, interpretation of the analysis results, and critical revision of the manuscript for important intellectual content. LJ is responsible for the overall content as the guarantor. All authors read and approved the final manuscript.
Funding This work was supported by the Natural Science Foundation of Liaoning Province, China (2020-MS-335).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.