Article Text

Statistics from Altmetric.com
A 65-year-old patient presented with endometrial adenocarcinoma G2, myometrial invasion >50%, and enlarged precaval (6×3 cm) and retrocaval (3×1.5 cm) lymph nodes up to the level of the renal veins on computed tomography. Clinical stage was cT1bN2M0, IIIC2.
According to the Russian guidelines on the treatment of uterine malignancy, surgery is the treatment of choice for these patients.1 Total hysterectomy with pelvic and para-aortic lymphadenectomy was planned.
Left extraperitoneal laparoscopic para-aortic lymphadenectomy for cervical cancer was first described by Dargent et al. The feasibility and advantages of this approach as a staging procedure for gynecologic malignant tumors have been shown in different studies.2 3 However, the standard left extraperitoneal approach provides limited access to the paracaval and retrocaval areas, so the right extraperitoneal approach was used for this patient.
Video 1 describes the benefits and feasibility of dissection of precaval and retrocaval bulky nodes by the right extraperitoneal laparoscopic approach. The right extraperitoneal access was created in the same way as from the left side.4 After placement of a 10 mm balloon trocar, the pneumo-extraperitoneum was created; 5 mm and 12 mm trocars were then placed on the right anterior axillary line and the right mid-clavicular line.
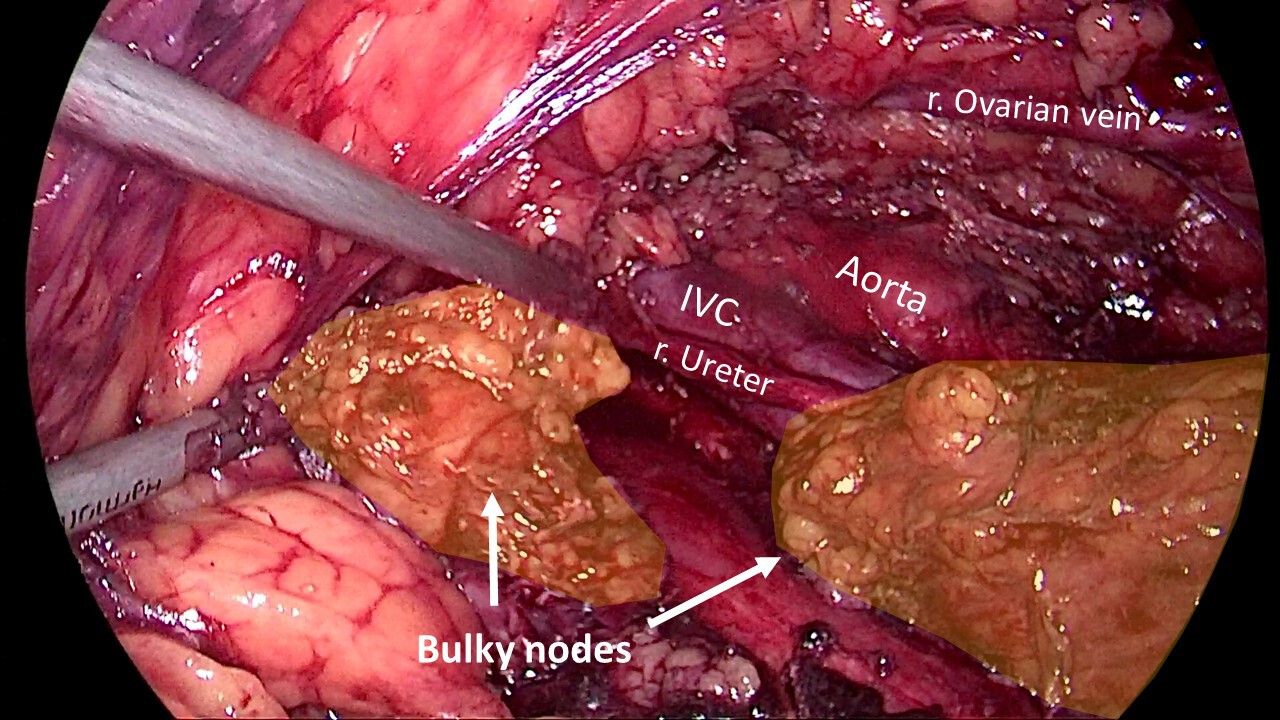
The main part of the surgery was performed with ultrasonic scissors. Using blunt dissection and sliding movements, enlarged nodes were carefully separated from the vena cava and the common iliac vein. Retrocaval nodes were separated from the posterior wall of the vena cava first and then from the surrounding tissue. The completely removed bulky nodes are shown in Figure 1.

{kind=link}
Completely removed precaval and retrocaval bulky lymph nodes.
The final pathologic evaluation confirmed metastasis in the para-aortic and pelvic nodes from both sides.
The main limitation of this approach is the insufficient access to the left aortic lymph nodes.
The surgery was carried out in the Gynecologic Oncology department of Kaluga Regional Cancer Center, Russian Federation.
Data availability statement
There are no data in this work.
Footnotes
Contributors All authors conceived the study concept and advised on the surgical procedure. All authors participated in writing the manuscript and approved the final version. All authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.