Article Text

Abstract
Background High-risk human papillomavirus (HPV)-positive women require triage to identify those at higher risk of cervical intraepithelial neoplasia grade 2 or worse (CIN2+). We aimed to compare visual assessment of the cervix, manual cytology and automated cytology as triage tests to screen HPV-positive women, and to assess over-treatment rates after visual assessment and over-referral rates to colposcopy after cytology.
Methods The present cross-sectional study is nested in a large prospective screening trial in Cameroon. Evaluations of the tests have been conducted individually and in combination with HPV-16/HPV-18/45 genotyping. For the evaluation of over-treatment and colposcopic over-referral, we simulated two screening scenarios: (1) one-visit scenario (test-triage-and-treatment); and (2) two-visit scenario (test-triage-and-colposcopy).
Results 1582 women with a median age of 40 years (IQR 35–45) performed self-sampling for HPV testing, of which 294 (18.6%) were HPV-positive, and 12.2% had CIN2+. Sensitivities for CIN2+ detection were 77.1% for visual assessment, 80.0% for manual cytology, and 84.8% for automated cytology. Sensitivity of combined tests was higher compared with single tests. The highest sensitivity was obtained by the combination of genotyping and automated cytology (91.2%). In the one-visit scenario, the over-treatment rate was 83.9% in referred women, with a ratio of 6.2 treated women per CIN2+. In the two-visit scenario, the lowest over-referral rate would have been under manual cytology (45.0%), with a ratio of 1.8 referred women per CIN2+. Single and combined triage strategies by automated cytology gave rise to over-referral rates of 69.2% and 76.7%, respectively, and a ratio of 3.2 and 4.3 referred women per CIN2+, respectively.
Discussion Triage of HPV-positive women using a combination of genotyping and automated cytology for CIN2+ detection may provide public benefits in low- and middle-income countries.
- cervical cancer
- pathology
Data availability statement
Data are available upon reasonable request. In accordance with the journal’s guidelines, we will provide our data for the reproducibility of this study in other centers if such is requested.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, an indication of whether changes were made, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
HIGHLIGHTS
Combining single triage tests with HPV-16/HPV-18/45 genotyping improves sensitivity for CIN2+ detection.
The combined use of HPV genotyping and smartphone digital images of the cervix (D-VIA/VILI) improves sensitivity.
A completely automated screening process by HPV genotyping and automated cytology showed the highest sensitivity.
Introduction
In recent years, human papillomavirus (HPV) testing has been introduced as an alternative to cytology for cervical cancer screening in high-income countries and in some low- and middle-income countries. One limitation of primary HPV testing is its low specificity. Therefore, to avoid unnecessary colposcopy referral and over-treatment, appropriate HPV-positive triage is crucial. Depending on national guidelines, some countries may choose triage with one or two sequential tests followed by immediate treatment of positive women, or schedule an additional visit for colposcopy triage.
Triage with quality-assured cytology and referral to colposcopy in a second visit is a suitable option for high- and middle-income countries. Management of HPV-positive patients with negative cytology includes HPV testing at 12 months, allowing many infections to resolve spontaneously. Only women with persistent infection at 1 year should be referred to colposcopy.1 Quality of cytology diagnosis has improved since the introduction of computer-assisted screening,2 which determines the probability of containing abnormal cells.3 4 This could be useful in the triage of HPV-positive women as it provides accurate prognostic information without the need of visual assessment.5–7
An alternative to triage is to use HPV-16/18 genotyping as a molecular marker reflecting the underlying carcinogenic process,8 allowing HPV-16/18-positive women to be directly referred to colposcopy.9 Finally, the WHO recommends primary screening with HPV testing in low- and middle-income countries if resources are available, followed by visual inspection with acetic acid for triage and immediate treatment if positive.10
This cross-sectional study is nested in a large prospective trial termed the ‘3T-study’ (for ‘Test-Triage-Treat’ in a single visit) in Cameroon.11 Our aim was to assess and compare the performance of commonly used triage tests such as visual inspection of the cervix and manual cytology for the detection of cervical intraepithelial neoplasia grade 2 or more severe (CIN2+) in HPV-positive women, individually and in combination with HPV-16/HPV-18/45 genotyping. Additionally, performance of automated cytology as a possible tool for triage was evaluated. A further objective of the study was to simulate two scenarios to assess the over-treatment rate after visual assessment triage and over-referral rate to colposcopy after cytology triage.
Methods
Setting, Screening Program, and Study Design
This study is nested in a large prospective trial termed the ‘3T-study’ which started in September 2018 in the district hospital of Dschang (Cameroon). The study design has already been published.11 The data of the present study were retrieved between September 2018 and July 2019. Briefly, asymptomatic, non-pregnant women aged 30–49 years were eligible if they had no history of CIN treatment, no history of anogenital cancer, and no hysterectomy. The following clinical steps were applied after informed and signed consent: women meeting the inclusion criteria of the 3T-study were invited for an HPV self-test, using the point-of-care GeneXpert machine; HPV-negative women received counseling and recommendations to repeat screening after 5 years, while HPV-positive women were invited to undergo pelvic examination and visual assessment for triage using 3% acetic acid and Lugol’s iodine. Smartphone digital photographs were used as a diagnostic adjunct, to guide biopsies and to decide between either immediate thermal ablation or referral for a loop electrosurgical excision procedure; all HPV-positive women received cytology (manual and automated), biopsies, and endocervical brushing (see below). Study participants were informed about their histopathological results by phone and advised to return for treatment in case of missed CIN2+ on initial examination.
The trial obtained approval from the Cantonal Ethics Board of Geneva (CCER, N°2017–0110) and the Cameroonian National Ethics Committee for Human Health Research (N°2018/07/1083/CE/CNERSH/SP). The study protocol was registered under ClinicalTrials.gov (number NCT03757299).
Study Procedures
Sociodemographic characteristics and medical history were obtained through a standardized questionnaire. Women were then asked to provide a self- collected vaginal sample for HPV testing with a swab (FLOQSwabs).
HPV testing: the swab was rinsed in a vial with 20 mL of sodium chloride 0.9%, vortexed for 30 s, and transferred into a single-use cartridge that holds PCR reagents of the GeneXpert analyzer (4-module configuration). The Xpert HPV assay specifically identifies HPV types 16 and 18/45 in two distinct detection channels and reports 11 other high-risk types in a pooled result. It uses an internal assay control for specimen adequacy in the detection of a Human reference gene and an internal Probe Check Control.
Visual assessment and treatment were performed by trained midwives. As a complement to naked-eye inspection (VIA/VILI), we introduced digital imaging of the cervix (D-VIA/VILI) using a Samsung Galaxy S5 smartphone and the application ‘Exam’.12 13 Furthermore, we implemented an ABCD mnemonic method for visual assessment according to the following criteria: A for ‘Acetowhiteness’, B for ‘Bleeding of a lesion in the transformation zone’, C for ‘Coloring confirmation with Lugol’s iodine’, and D for ‘Diameter of the acetowhite area’ (≥0.5 cm).11 To be considered ABCD-positive, at least one of the following conditions needed to be fulfilled: presence of criteria A and D combined or criterion B (with or without presence of A, C or D). Decision to treat or not was based on VIA/VILI and D-VIA/VILI combined diagnosis. All smartphone cervigrams were ultimately reviewed by expert colposcopists.
Cytology: Cervical cells were collected using a plastic spatula and preserved in alcohol-based fluid (BD SurePath). The vials were transported to Switzerland (Unilabs, Geneva), where thin layer slides were prepared with a fully robotic system. All slides were first automatically scanned with the BD FocalPoint system, followed by guided assisted manual screening according to the manufacturer’s instructions. Cytotechnicians were blinded from the histopathologic and visual assessment diagnoses, but were aware of the HPV-positive status.
Manual screening: Cytological diagnosis was provided using the Bethesda classification system with ASC-US (atypical squamous cells of undetermined significance) as threshold of positivity.
Automated screening: The BD FocalPoint system scans the slides using a video-equipped microscope, and image interpretation software analyzes the complex images. It differentiates and measures features from each slide and translates this information into an anomaly score from 0.0 to 1.0. Each slide is ranked based on this anomaly score and classified into ‘Review’ and ‘No further review’ (NFR). Review slides are then ranked into five quintiles from highest probability (quintile 1) of high-grade squamous intraepithelial lesion to lowest (quintile 5), helping to understand the inherent risk of high-grade squamous intraepithelial lesion in each slide.4 5
For our analyses, we defined: (1) a high-risk group (quintiles 1 and 2), considered positive for CIN2+ prediction; and (2) a low-risk group (quintiles 3–5 and the NFR category), considered negative for CIN2+ prediction.
Histopathology: Assessment of cervical tissue obtained from biopsies and endocervical brushing served as the reference standard for diagnostic accuracy. Biopsies were performed at 6 o’clock within the transformation zone and near the squamocolumnar junction when no lesion was seen, or at the site of the anomaly when present. Slides were prepared in the Division of Pathology (Geneva University Hospitals). Two gyneco-pathologists blinded from cytology results provided adjudicated diagnosis.
Screening Scenarios and Outcomes
Retrieved data from the 3T-study made it possible to compare the diagnostic performance of various triage methods of HPV-positive women and simulate two screening scenarios using different strategies for immediate treatment or referral to colposcopy:
One-visit scenario (Test-Triage-Treat). Immediate treatment if: (i) positive visual assessment (single test); (ii) positive HPV-16/HPV-18/45 genotyping and/or positive visual assessment (combined test).
Two-visit scenario (Test-Triage-Colposcopy). Referral to colposcopy if: (i) positive manual cytology (single test); (ii) positive HPV-16/HPV-18/45 genotyping and/or positive manual cytology (combined test); (iii) positive automated cytology (single test); (iv) positive HPV-16/HPV-18/45 genotyping and/or positive automated cytology (combined test).
For the combined triage tests, the result was considered negative if both tests were negative. If one of the tests was negative and the other one did not have a valid result, the case was excluded from the analysis.
Statistical Analysis
Sensitivity, specificity, positive predictive value, and negative predictive value for CIN2+ and CIN3+ detection were calculated as proportions with their associated 95% confidence intervals (95% CI). Sensitivities versus false positive rate (FPR=1−specificity) were determined to evaluate the diagnostic ability of the triage tests.
To assess the proportion of over-treatment and over-referral to colposcopy for each triage scenario, we divided the number of women with normal histologic results by the number of women referred for treatment or colposcopy. We also calculated the number of treatments per CIN2+ and colposcopies required to detect one case of CIN2+.
The Student’s t-test, Mann–Whitney test or Pearson’s χ2 test (as appropriate) were used to compare outcomes of interest between groups. All analyses were two-sided and p values <0.05 were considered statistically significant. Analyses were carried out using the STATA software, version 14 (StataCorp, College Station, TX). In accordance with the journal’s guidelines, we will provide our data for the reproducibility of this study in other centers if such is requested.
Results
Study Population
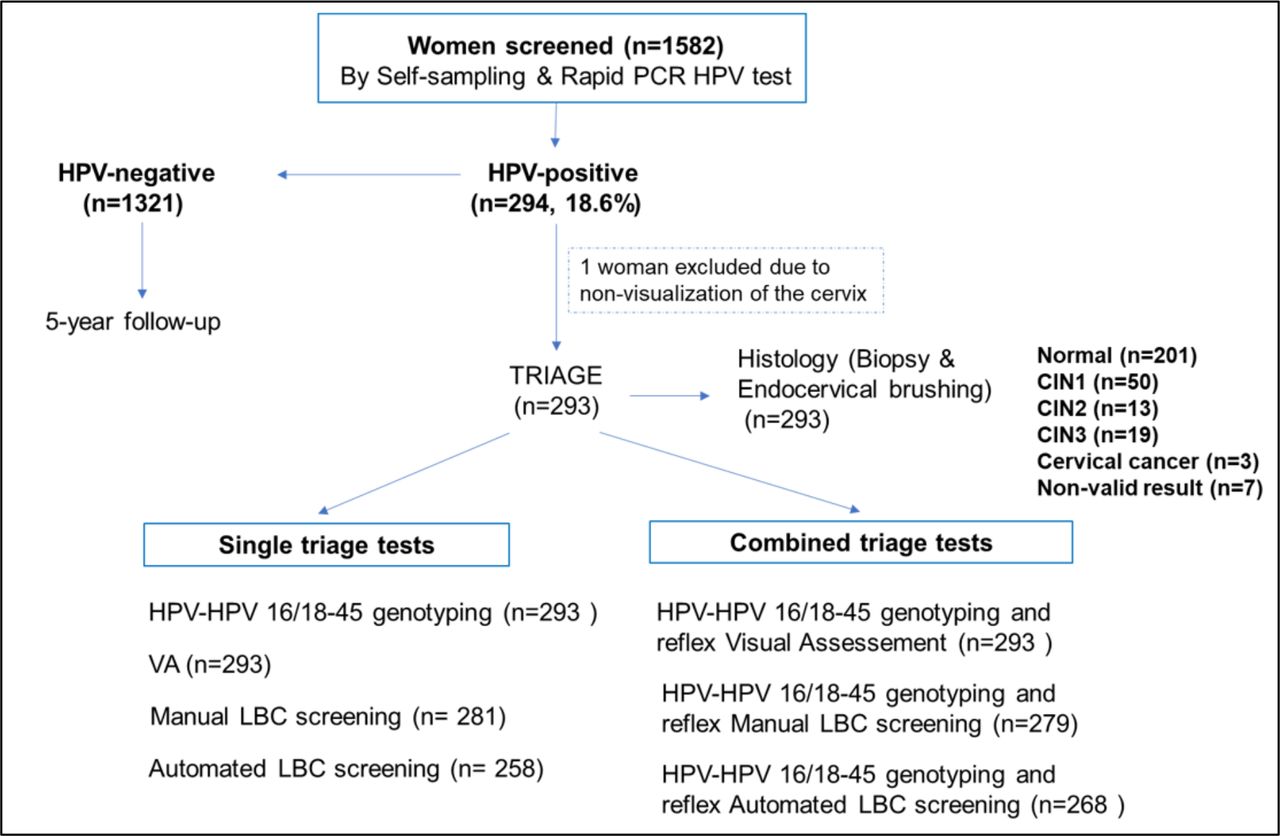
Overall, 1598 eligible women accepted to participate in the 3T-study between September 2018 and July 2019, of which 1582 (99.0%) performed self-sampling for HPV testing, and 294 (18.6%) were HPV-positive. Among HPV-positive women, 293 (99.7%) underwent triage and had biopsies and endocervical brushing performed. A total of 286 (97.6%) women had a successful histopathological diagnosis, of which 87.8% were diagnosed as normal or CIN1, and 12.2% had pathological results (13 CIN2, 19 CIN3, three cancers) (Figure 1).
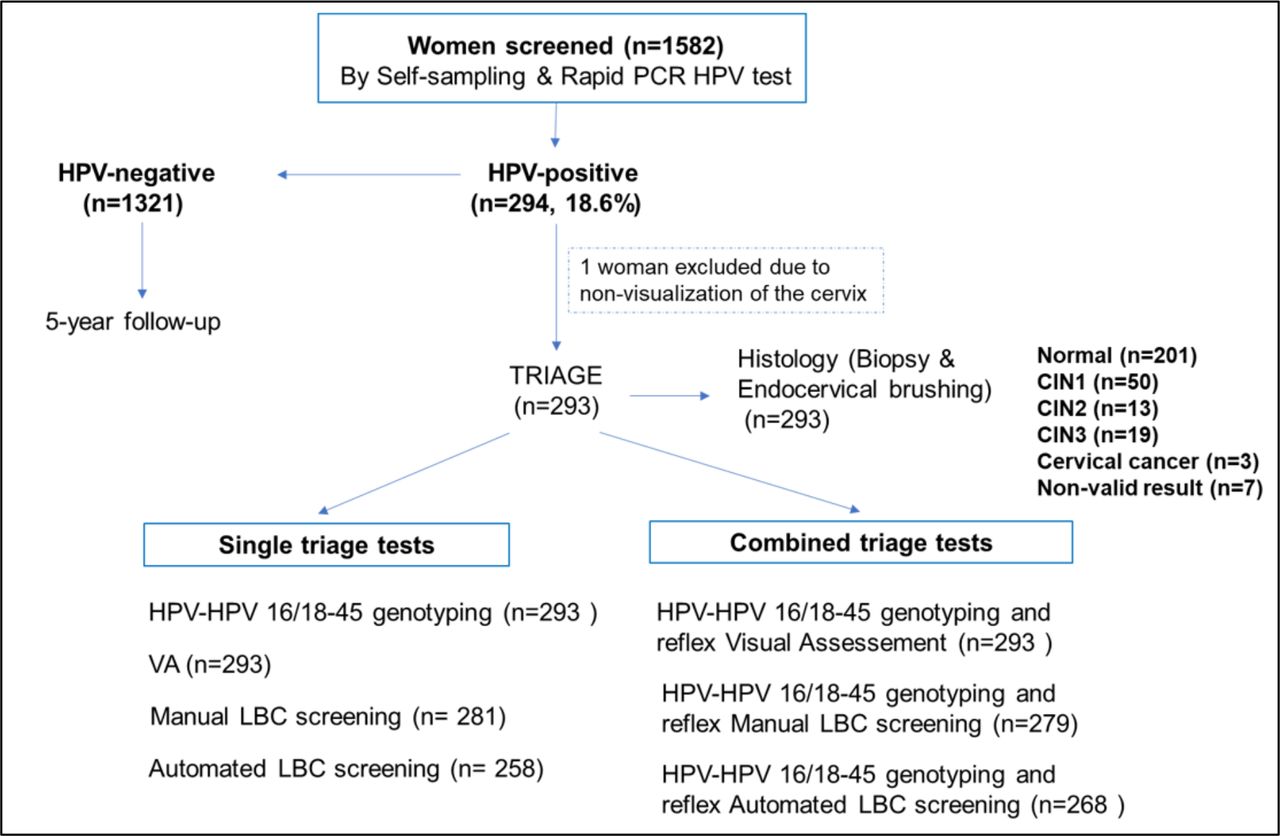
Study flowchart showing study population, histology results, and triage tests evaluated. CIN1, cervical intraepithelial neoplasia grade 1; CIN2, cervical intraepithelial neoplasia grade 2; CIN3, cervical intraepithelial neoplasia grade 3; HPV, human papillomavirus; LBC, liquid-based cytology; n, number; VA, visual assessment.
Epidemiological Characteristics
The median age of screened women was 40 (IQR 35–45) years. Compared with HPV-negative women, HPV-positive participants were more frequently single (10.3% vs 7.8%) or divorced/widowed (11.3% vs 5.2%). The mean number of sexual partners was higher in HPV-positive women (4.2±3.8 vs 3.8±3.3). A majority (69.4%) did not use contraception. A significantly higher proportion of women reported being HIV-positive in the HPV-positive group (6.6%) than in the HPV-negative group (2.5%) (Table 1).
Baseline sociodemographic, reproductive health and clinical characteristics
Triage Results Distribution by Histology Classification
Among all HPV-positive participants with valid histopathological results, 58.7% had a positive visual assessment, 18.5% were diagnosed ≥ASC US by manual cytological screening, 36.0% were classified as positive by automated cytology, and 22.4% were positive for HPV-16 and/or HPV-18/45. Concerning positivity of combined testing with HPV-genotyping, 67.1% of women were positive with reflex visual assessment screening, 34.4% were positive with reflex manual cytology, and 50.6% were positive with reflex automated cytology screening (Figure 1 and Online supplemental table S1).
Supplemental material
Performance of Triage Tests
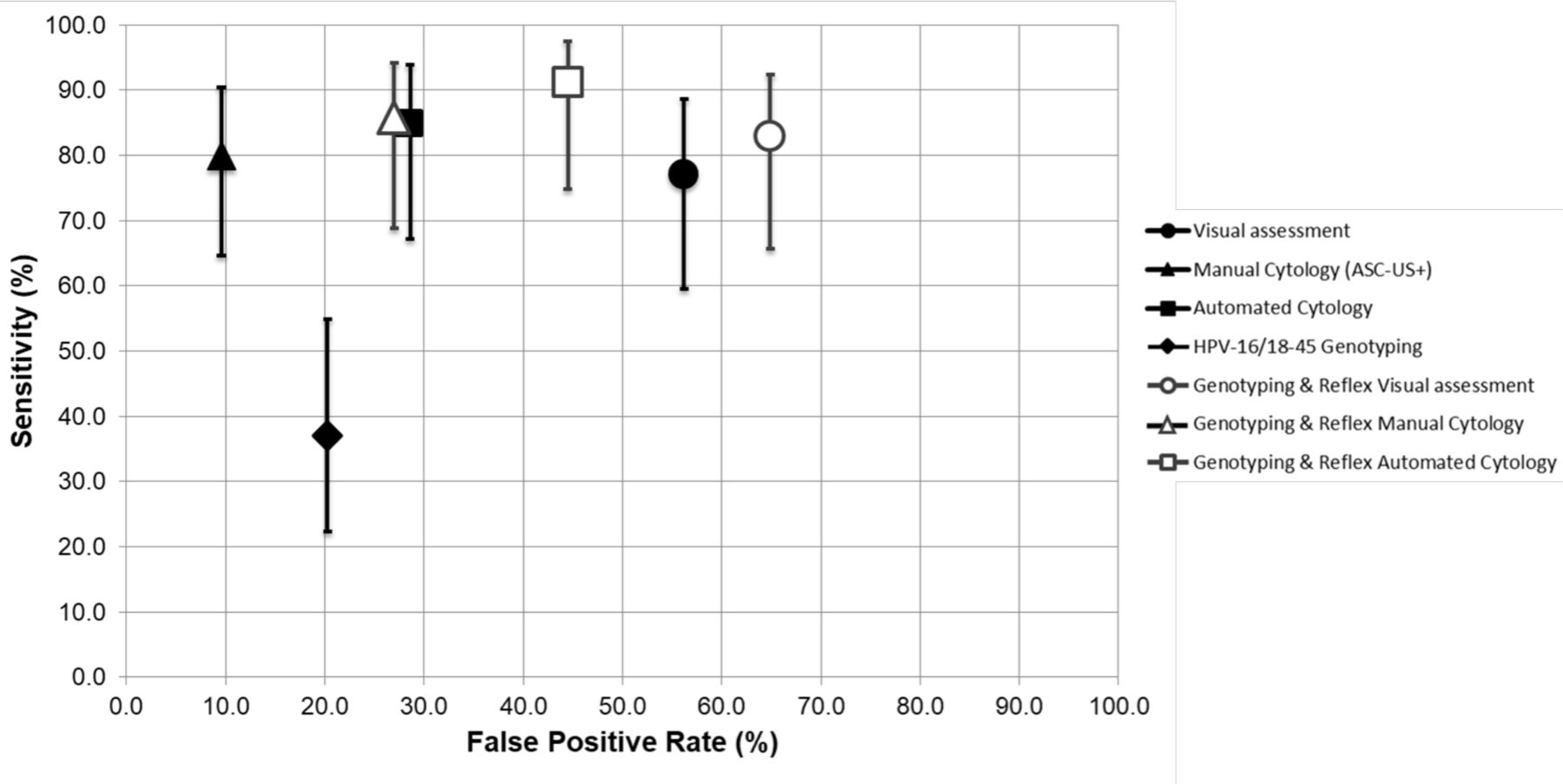
The sensitivities of individual tests for the detection of CIN2+ were 77.1% (95% CI 59.5% to 88.6%) for visual assessment, 80.0% (95% CI 62.6% to 90.5%) for manual cytology, and 84.8% (95% CI 67.2% to 93.9%) for automated cytology (Table 2).
Diagnostic performance of single and combined triage tests for CIN2+ and CIN3+ detection among HPV-positive women
HPV-16/HPV-18/45 genotyping alone had a sensitivity of 37.1% (95% CI 22.3 to 54.9). The highest sensitivity for CIN2+ detection was obtained by combining HPV-16/HPV-18/45 genotyping and automated cytology (91.2%, 95% CI 74.8% to 97.3%). Although sensitivities of visual assessment and manual and automatic cytology were statistically indistinguishable, we noticed a gain in sensitivity of combined tests compared with single tests, at the cost of an increased false positive rate (decreased specificity) (Figure 2).
{kind=link}
{kind=link}
Sensitivity (with 95% CI) versus the false positive rate (FPR=1−specificity) for CIN2+ detection among HR-HPV positive women for various triage tests (single and combined). ASC-US, atypical squamous cells of undetermined significance; CIN2+, cervical intraepithelial neoplasia grade 2 or worse; HPV, human papillomavirus; HR-HPV, high risk HPV.
Performance of Screening Scenarios for Treatment and Colposcopy Referrals
In the one-visit scenario, the proportion of HPV-positive women that would be referred for treatment under single and combined visual assessment triage was 58.7% and 67.1% respectively, with no noticeable difference concerning over-treatment rates (83.9% and 84.8%, respectively) nor ratios of treated women per CIN2+ (6.2 and 6.6, respectively). In the whole population screened, 8.9% of the screened women (141 of 1582) would therefore be over-treated. In the two-visit scenario, the lowest proportion of women referred to colposcopy would be obtained under manual cytology (18.5%), while the largest referral would be under combined genotyping and reflex automated cytology (50.6%), with an over-referral of 76.7% (Table 3).
Performance of screening scenarios according to triage strategies stratified by referral rates to treatment or colposcopy, histology results, over-treatment or over-referral rates to colposcopy, and number of treatments or colposcopies per CIN2+
Discussion
Summary of Main Results
This cross-sectional study found that a combined triage strategy of HPV-16/HPV-18/45 genotyping with visual assessment and manual cytology increases sensitivity to detect CIN2+ among HPV-positive women. Similarly, sensitivity was increased with the combined use of genotyping and automated cytology. The simulation of two screening scenarios demonstrated that combined tests offer a reliable triage strategy for immediate treatment or referral to colposcopy.
Results in the Context of Published Literature
Performance of Triage Tests
The sensitivity of visual assessment found for detection of CIN2+ and CIN3+ are among the highest reported in general populations where visual inspection was used,14–16 especially when combined with HPV-16/HPV-18/45 genotyping, and might be related to the introduction of D-VIA/VILI and the adoption of ABCD positivity criteria. It has been demonstrated that digital cervicography implemented as quality assurance may increase the sensitivity of visual inspection.17 In a previous study in Cameroon, we found that visual assessment triage without D-VIA/VILI and ABCD criteria performed poorly by reducing the original sensitivity of the HPV test by 66% for CIN2+ detection.18 Similarly, other studies found lower sensitivity with visual assessment triage of HPV-positive women.19 20 To our knowledge, this is the first study showing that the use of HPV-16/HPV-18/45 genotyping and reflex D-VIA/VILI offers a substantial improvement in detection of CIN2+ and CIN3+ lesions for triage of HPV-positive women.
Manual cytology is the currently recommended triage test for HPV-positive women with referral of ASC-US+ cases to colposcopy. In our study, manual cytology (single or combined) demonstrated the best balance of sensitivity, specificity, and predictive values for CIN2+ and CIN3+ detection. Like other studies,8 21 22 we found that a combination of cytology and HPV-16/18 genotyping for triage of HPV-positive women further increases sensitivity.
Our study demonstrates that a complete automated strategy using genotyping and reflex automated cytology might be a useful tool offering high sensitivity for the detection of CIN2+ and CIN3+ lesions and confirms our previous results that automated cytology is a promising triage approach.5 6 23 Yu et al have developed a risk score algorithm using the same system as in our study (Focal Point) and found that 91.7% of HPV-positive CIN3 and adenocarcinoma-in-situ cases were referred for immediate colposcopy.23
Performance of Screening Scenarios
The one-visit scenario is very convenient for low-resource settings because it reduces cost and risk of loss to follow-up. In this context, high sensitivity tests for primary screening and triage are crucial because they reduce missed opportunities for diagnosis and treatment of CIN2+ disease. Low- and middle-income countries adopting a screen-and-treat approach should weigh the risk of unnecessary treatment and harm against the benefits of early detection and treatment. A high false positive rate of visual inspection is a well-known limitation in primary screening.24 In our study, the use of ABCD criteria may have potentially increased false positive results because any whitening induced by benign conditions was considered positive. Although we are aware that the low specificity for CIN2+ means significantly more women will receive treatment than necessary, we consider this over-treatment rate acceptable for underserved rural communities where high loss to follow-up could be a serious issue for screening programs.25
It should be noted that ablative therapy is an affordable option for low resource settings, with a good cure performance and adherence (>90%) and with a vast majority associated with well-tolerated and temporary side effects, which are accepted by women after preventive patient counseling.26 27
The two-visit screening scenario is suitable for middle- and high-income countries. The study demonstrated that quality-assured cytology would be an accurate triage test for CIN2+ and CIN3+ lesions with an acceptable rate of referral to colposcopy. The number of colposcopies required to detect one case of CIN2+ after single and combined manual cytology triage was lower in our study than in studies in Mexico and China, which showed a ratio of 5.9 and 3.7 respectively after single cytology triage, and a ratio of 7.2 and 5.0 respectively after combined triage with HPV-16 and/or 18 genotyping and reflex cytology.21 22 By comparison, automated cytology combined with genotyping showed in our study a ratio of 4.3.
Strengths and Weaknesses
The major advantage of this study is that it was conducted in a real-world setting and all HPV-positive women underwent biopsy and endocervical brushing to minimize disease misclassification. A limitation of our study is that our results cannot be generalizable to populations with different disease prevalence and screening costs. Further validation is needed to verify whether our results are comparable across other low- and middle-income countries’ contexts. The number of CIN2+/CIN3+ lesions was relatively small, therefore the difference in accuracy of combined tests compared with single tests failed to reach statistical significance. Finally, performance of VIA/VILI compared with D-VIA/VILI was not assessed in this study and should be considered for further research.
Implications for Practice and Future Research
Our results raise a difficult question, namely, how to determine an acceptable sensitivity-to-specificity balance of triage tests. In low-income countries where women are screened once or twice in a lifetime, a triage test such as visual assessment with high sensitivity and low specificity may be convenient. The use of artificial intelligence as a diagnostic aid for visual assessment of the cervix is a growing trend in low- and middle-income countries. A promising triage approach to improve accuracy of visual assessment is the automatic detection of CIN2+ using digital image-based machine learning models.28 29
In middle- and high-income countries, manual cytology is considered an acceptable triage test offering a higher specificity. Triage by genotyping combined with reflex cytology increases sensitivity but leads to a higher number of colposcopies. Cost-effectiveness analyses would be useful, as it was found previously that despite its relatively high referral rate to colposcopy, HPV primary screening with reflex genotyping and cytology remain a cost-effective strategy.30
Additional studies are required to evaluate the performance and cost of automated cytology as a triage tool and determine whether its introduction would be feasible in some middle-income countries, or even in high-income countries where the prevalence of the disease is decreasing. Alternative technologies applying artificial intelligence for object detection using machine-learning algorithms are emerging in the field of computational cytology31 32 and might be more cost-effective.
Conclusions
Our study demonstrates a high sensitivity of visual assessment of the cervix, and manual and computer-interpreted cytology, used as triage tests to detect CIN2+ among HPV-positive women. Sensitivity was further improved when single tests were combined with HPV-16/HPV-18/45 genotyping. The benefit provided by a high sensitivity conducive to early detection and prompt treatment of the disease in low- and middle-income countries may counterbalance cost and harm of over-treatment or over-referral to colposcopy.
Data availability statement
Data are available upon reasonable request. In accordance with the journal’s guidelines, we will provide our data for the reproducibility of this study in other centers if such is requested.
Acknowledgments
We would like to thank all the women who participated in the study and the doctors and nurses who examined the women in Cameroon. We would also like to thank all our funders for the economic support. Finally, we thank the Cytopath laboratories (Unilabs, Geneva) for their help in cytopathological analyses.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors All authors contributed substantially to the study and preparation of the manuscript.
Funding This study was funded by ESTHER, Solidarité Internationale Genève, the Private Foundation of Geneva University Hospitals (HUG), the Groupement Romand de la Société Suisse de Gynécologie et Obstétrique, the University Hospital of Geneva (Switzerland) and the University of Dschang (Cameroon).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.