Article Text

Abstract
Background Villoglandular adenocarcinoma is a rare sub-type of cervical adenocarcinoma.
Objective To analyze the clinicopathological features and evaluate the prognosis of patients with villoglandular adenocarcinoma of the cervix.
Methods Patient characteristics, procedure, pathology, and surgical outcomes were retrospectively reviewed in patients with villoglandular adenocarcinoma between November 2006 and June 2019 from multiple centers in China. In order to explore the difference between villoglandular adenocarcinoma and routine adenocarcinoma, patients (FIGO 2009 stage IA1–IB2) who had complete data during the same time period were included.
Results A total of 60 patients with villoglandular adenocarcinoma and 104 with standard adenocarcinoma were included. The median age of the patients with villoglandular adenocarcinoma was 42 years (range 27–68). The most common 2009 FIGO stage was IB1 in 39 (65%) patients with villoglandular adenocarcinoma. A total of 23 patients underwent laparoscopic surgery (two total hysterectomies, 21 radical hysterectomies) and the other 37 patients underwent laparotomy (three total hysterectomies, 34 radical hysterectomies). A total of 56 patients underwent lymphadenectomy and three (5.4%) had positive lymph nodes. Fifteen (25%) patients had one or both ovaries preserved. Seven patients were lost to follow-up. The median follow-up time for the entire group was 50.2 months (range 5.1–154.6). No deaths or recurrences occurred. Excluding six patients with FIGO 2009 stage II, the 5-year disease-free survival of the 47 patients with villoglandular adenocarcinoma with FIGO 2009 stage I for whom there was follow-up, was significantly higher than that of the 104 patients with standard cervical adenocarcinoma (100% vs 92.2%, log-rank p=0.039). However, the 5-year overall survival of the two groups did not differ (100% vs 95.7%, log-rank p=0.11).
Conclusion Villoglandular adenocarcinoma has a favorable prognosis. Further studies are needed to provide more details of treatment strategies and prognosis.
- cervical cancer
- adenocarcinoma
- pathology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, an indication of whether changes were made, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
HIGHLIGHTS
Villoglandular adenocarcinomas rarely have lymph node involvement (5%) or lymphovascular invasion (3%).
No death or recurrence occurred in patients with villoglandular adenocarcinoma during the follow-up period of 50.2 months.
The 5-year disease-free survival of patients with villoglandular adenocarcinoma was significantly better than of patients with other types of cervical adenocarcinoma
INTRODUCTION
Cervical cancer is one of the most common malignant tumors in the female reproductive system in developing countries. A total of 13 240 new cases and 4170 deaths were estimated in the USA in 2019.1 In 2018, there were 570 000 new cases of cervical cancer, which represented 6.6% of all female carcinomas in the world.2 The incidence of squamous cell carcinoma has declined significantly and the incidence of cervical adenocarcinoma continuously increased from 5% to 25% in the past decades.3–5 Cervical adenocarcinoma is generally associated with lymph node metastasis and distant metastasis, which may lead to poor prognosis.6–9
Villoglandular adenocarcinoma is a rare sub-type of cervical adenocarcinoma and it was first described in 1989 by Young and Scully.10 The International Endocervical Adenocarcinoma Criteria and Classification (IECC) declared that villoglandular adenocarcinoma is an human papillomavirus (HPV)-associated adenocarcinoma.11 The incidence of villoglandular adenocarcinoma is between 4% and 8.8%,12 13 which is lower than for cervical adenocarcinoma.14–16 Villoglandular adenocarcinoma tumors have a lower risk of deep infiltration, lymphovascular invasion, and lymph node metastasis.15 17 The majority of studies suggest that the long-term prognosis of villoglandular adenocarcinoma is considered favorable.16–18
The standard surgery for patients with International Federation of Gynecology and Obstetrics (FIGO 2009) stage IA1 combined with lymphovascular invasion and stage IA2–IIA1 cervical adenocarcinoma is radical hysterectomy and pelvic lymph node assessment.7 19 In this study, the clinical and pathological characteristics of patients with villoglandular adenocarcinoma in multiple centers in China were reviewed and the risk factors were evaluated. We also compared the outcomes of patients with villoglandular carcinoma with those of patients with standard adenocarcinoma in the same period.
METHODS
Patients with adenocarcinoma between November 2006 and June 2019 were retrospectively reviewed. Clinical characteristics, HPV testing, pathological features, treatment, and prognosis were analyzed. Inclusion criteria of patients with villoglandular adenocarcinoma were as follows: villoglandular adenocarcinoma confirmed by pre-operative biopsies and/or post-operative pathological examination. Pathological diagnostic criteria for villoglandular adenocarcinoma were as follows: exophytic pattern of growth with long and slender papillary structures, mild to moderate cellular atypia, and scattered mitotic figures. All specimens were reviewed by at least two pathologists and audited by a senior pathologist. Exclusion criteria were the presence of other malignancy from either villoglandular carcinoma or standard adenocarcinoma and incomplete medical records.
In order to explore the difference between villoglandular adenocarcinoma and standard adenocarcinoma with FIGO 2009 stage I, a total of 104 patients with standard cervical adenocarcinoma (FIGO 2009 stage I) were screened in the same period. The establishment of the cervical cancer database was reviewed by the ethics committee of Nanfang Hospital, Southern Medical University (ethics number NFEC-2017–135).
Statistical Product and Service Solutions (SPSS) 25.0 statistical software was used to analyze the data. A t-test was adopted for measurement of data. Enumeration data were evaluated using the chi-square test and Fisher exact test. The survival patterns of patients with villoglandular adenocarcinoma and patients with standard adenocarcinoma were shown graphically using Kaplan-Maier survival curves. Groups were compared by the log-rank test.
RESULTS
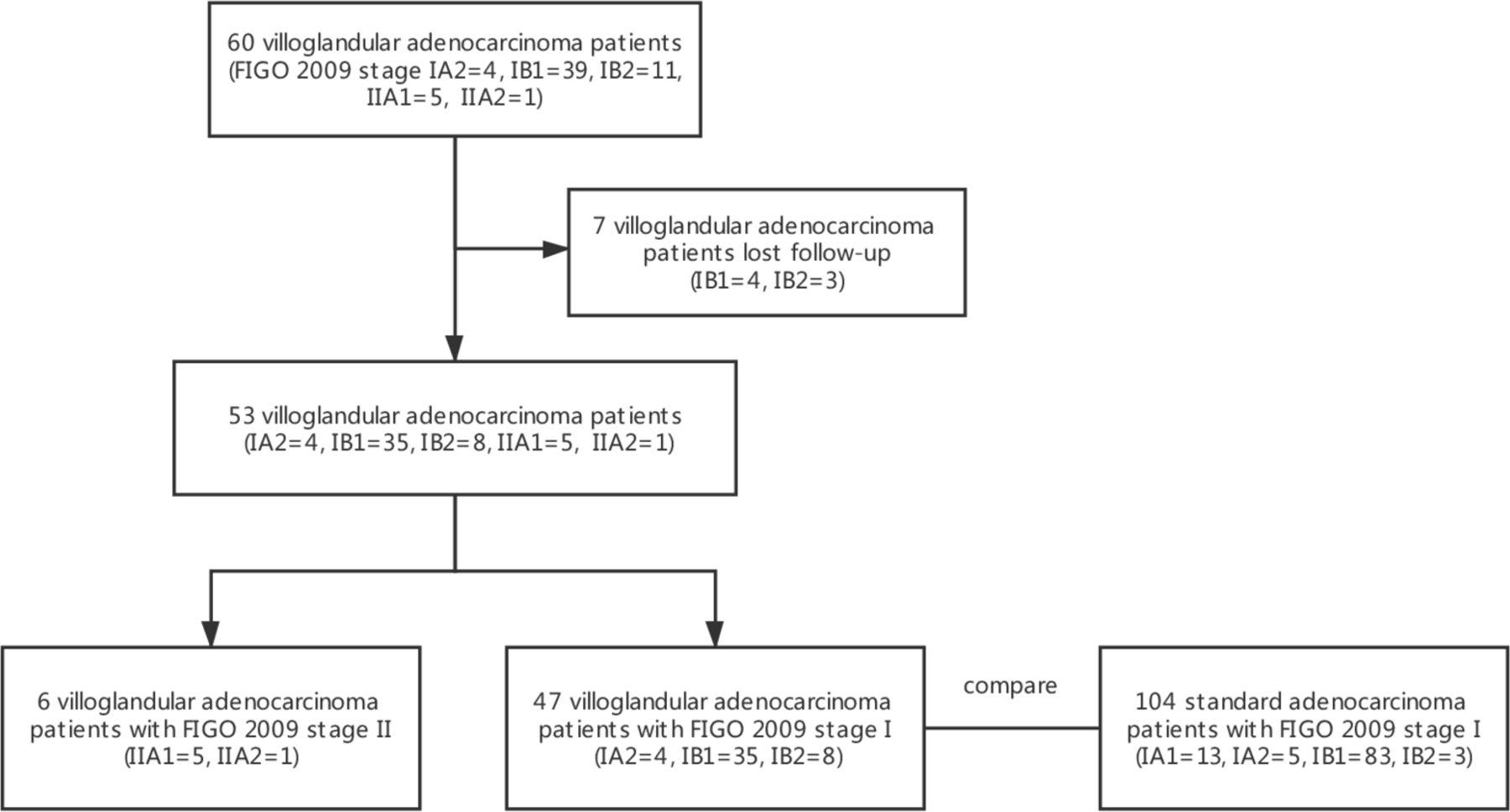
A total of 1515 patients with adenocarcinoma were screened and 60 patients with villoglandular adenocarcinoma (4%) were included in our analysis (Online supplemental table 1). The median age was 42 years (range 27–68). The most common symptoms were irregular vaginal bleeding or post-coital bleeding (41.9%). The most common tumor growth pattern was exophytic type (67.9%). The 2009 FIGO stage distribution was 4 patients stage IA2, 39 patients stage IB1, 11 patients stage IB2, 5 patients stage IIA1, and 1 patient stage IIA2. A total of seven patients were lost follow-up (Figure 1). The mean maximum diameter of the tumor was 2.12±1.78 cm and tumors ≥2 cm accounted for 71.7% (Table 1).
Supplemental material

Flow diagram of patient selection.
Clinicopathological features and prognosis of 60 patients with villoglandular adenocarcinoma*
In the laparoscopic surgery group (n=23), two patients underwent laparoscopic total hysterectomy without pelvic lymphadenectomy and 21 patients underwent laparoscopic radical hysterectomy with pelvic lymphadenectomy. In the laparotomy surgery group (n=37), three patients underwent total hysterectomy and only one underwent pelvic lymphadenectomy. The other 34 patients underwent laparotomy radical hysterectomy group with pelvic lymphadenectomy. The median follow-up was 38.8 months (range 13–85.2) for patients who had laparoscopic surgeries and 56.5 months (range 5.1–154.6) for those who underwent open surgeries (Table 1). A total of 56 patients underwent lymphadenectomy and three (5.4%) had positive lymph nodes. A total of 27 (45%) patients received adjuvant therapy (Online supplemental table 1).
Eighteen of 20 patients had positive-HPV results and nine of 13 patients had abnormal cervical cytology screening (Table 1). In a total of 38.3% of patients the preoperative diagnosis of villoglandular adenocarcinoma was consistent with the post-operative result. Villoglandular adenocarcinomas were found to be primarily well differentiated (grade I/II,97.1%), rarely to have lymphovascular space invasion (3.3%), and mainly having superficial cervical interstitial infiltration (≤1/2, 71.7%). A total of 6.7% of patients had uterine infiltration and 5.4% of patients had lymph node metastasis (Table 1). In this study, 75% patients were found to be p16 positive and the Ki67 index was increased in 75% of patients (Online supplemental table 2).
A total of 15 patients preserved unilateral/bilateral ovaries. These patients were younger (39.6 vs 45.2 years, p=0.024) and more underwent simple hysterectomy (26.7% vs 2.2%, p=0.015)in comparison with those who had oophorectomy. No tumor recurrence or metastasis occurred in these patients. Moreover, there was no statistical difference in pathological factors such as tumor differentiation, lymphatic vessel infiltration, interstitial infiltration depth, uterine infiltration, lymph node metastasis, parametrium, and vaginal resection margin infiltration (p>0.05).
The clinicopathological features of 47 patients with villoglandular adenocarcinoma were compared with those of 104 patients with common adenocarcinoma (FIGO 2009 stage I). No significant difference was found in the rate of HPV infection between the two groups (p=0.99). However, patients with villoglandular adenocarcinoma were more likely to have HPV16 sub-types (70.6% vs 33.3%, p=0.004), whereas patients with cervical adenocarcinoma were more likely to have HPV18 sub-types (17.6% vs 47.6%, p=0.023). In addition, patients with villoglandular adenocarcinoma were younger (43.8 vs 47.1 years, p=0.029) than patients with standard adenocarcinoma. Comparison of the villoglandular adenocarcinoma group with the group with standard adenocarcinoma showed that the proportion of pre-menopausal women was higher in the former (81.8% vs 66.4%, p<0.001), rates of grade I were higher (46.4% vs 17.6%, p=0.003), and there was more superficial cervical infiltration (70.0% vs 66.7%, p=0.004). Although more FIGO stage IB2 patients were included in the villoglandular adenocarcinoma group (17.0% vs 2.9%, p=0.001), no recurrence or death occurred in the villoglandular adenocarcinoma group. In the standard adenocarcinoma group, six patients relapsed and three patients died of disease (Table 2). The 5-year disease-free survival of patients with villoglandular adenocarcinoma was significantly better (100% vs 92.2%, log-rank p=0.039) than that of patients with standard adenocarcinoma, but no significant differences in 5-year overall survival was noted between the two groups (100% vs 95.7%, log-rank p=0.11) (Figure 2). Analysis of disease-free survival and overall survival between the two groups with or without ovarian preservation showed no difference (p>0.05). None of the patients who underwent simple hysterectomy relapsed (Figure 3).

Comparison of survival outcomes between villoglandular adenocarcinoma and cervical adenocarcinoma. AC, adenocarcinoma; VGA, villoglandular adenocarcinoma.

{kind=link}
{kind=link}
{kind=link}
Comparison of survival outcomes between ovarian-reserving villoglandular adenocarcinoma and cervical adenocarcinoma. AC, adenocarcinoma; RO, reserved ovarian-function; VGA, villoglandular adenocarcinoma.
Comparison of clinicopathological features between patients with villoglandular adenocarcinoma and those with standard cervical adenocarcinoma*
DISCUSSION
Summary of Main Results
Our results demonstrate that patients with villoglandular adenocarcinoma have more favorable clinicopathologic features and prognosis than patients with standard cervical adenocarcinoma. No deaths or recurrence occurred even in patients who underwent laparoscopic surgery or more conservative surgery, such as simple hysterectomy or ovarian preservation, during the follow-up period of 50.2 months.
Results in the Context of Published Literature
The literature has reported that the age range of patients with villoglandular adenocarcinoma is between 33 and 52 years.5 7 10 12 13 20–23 Our study reported that patients with villoglandular adenocarcinoma were younger than those with standard cervical adenocarcinoma and 81% were pre-menopausal women.
Villoglandular adenocarcinoma is associated with superficial invasion, well-differentiated tumor, uncommon lymphovascular invasion, and rare lymph node metastasis. Prior work reported the depth of stromal invasion of 64.3% patients to be less than 1/2.12 The lymph node metastasis rate of villoglandular adenocarcinoma is reported as between 2.7% and 11.7%.13 24 Lower lymph node metastasis (2.6% vs 14.2%, p=0.001) in villoglandular adenocarcinoma was reported than in standard adenocarcinoma.13
So far, at least 203 cases of villoglandular adenocarcinoma have been reported, with 12 recurrences and eight deaths.12 13 Most had more than one risk factor, such as lymph node metastasis, lymphovascular invasion, parametrial invasion. Guo et al compared villoglandular adenocarcinoma with adenocarcinoma in patients with FIGO 2009 stage I and found lower recurrence rates in those with villoglandular adenocarcinoma (2.6% vs 14.6%, p=0.038).13 The 5-year disease-free survival of patients with villoglandular adenocarcinoma in our study was also significantly better than for patients with standard cervical adenocarcinoma.
However, the less radical management approaches are still controversial. Data on conservative approaches, such as conization, simple hysterectomy, radical vaginal trachelectomy, and ovarian preservation, are limited.13 16 25 Kim et al reported on three patients with villoglandular adenocarcinoma who underwent cervical conization only, and none relapsed (IA1=2, IB1=1).12 Guo et al reported on two patients who underwent radical vaginal trachelectomy and pelvic lymphadenectomy, and there was no recurrence.13 Five patients in our study, including one with deep cervical stromal invasion, underwent simple hysterectomy, and none had recurrence. No consensus has been reached on ovarian preservation in young women with villoglandular adenocarcinoma. A study in Korea suggested that retaining ovarian tissue for stage IB–IIA patients with villoglandular adenocarcinoma24 might not be safe. Two patients with no risk factors developed recurrence in the adnexa and then underwent bilateral oophorectomy.24 However, none of the 15 patients (FIGO 2009 stage IA2=2, IB1=7, IB2=3, IIA1=2, IIA2=1) who retained their ovaries in our study had a recurrence.
As we know, the Laparoscopic Approach to Cervical Cancer (LACC) trial and other recent studies have shown that minimally invasive surgery in patients with cervical cancer has a worse oncologic outcome than open surgery.26–29 Dietl et al reviewed the literature and identified 23 patients with villoglandular adenocarcinoma who were treated by minimally invasive surgery. Four experienced recurrence and one patient died.30 Despite no recurrence being seen in our laparoscopic surgery group, the follow-up period was shorter than for open surgery group (38.8 vs 56.5 months, p<0.001).
Strengths and Weaknesses
The strengths of our study include our large sample size from multiple centers. In addition, we included patients with ovarian preservation and non-radical surgery. However, there were several limitations and these include the following. First, no central pathology review was carried out and therefore some of these tumors might have been reclassified on secondary evaluation. Second, we had no information about the criteria used for the surgical approach and post-operative management strategy. Third, during the study period, modalities of imaging and therapies might have changed within the institutions and we had no ability to control such change. Fourth, the median follow-up time of the laparoscopic surgery group was shorter than that of the open surgery group and therefore, we do not have information as to whether the laparoscopic approach affected oncologic outcomes. Lastly, as this was a multicenter study, we have no information on the auditing of data in the respective databases used in these institutions.
Implications for Practice and Future Research
The results of our study provide evidence of the indolent course of the disease in patients with cervical villoglandular adenocarcinoma. Therefore, we consider that future studies should aim to evaluate this cervical histologic sub-type as possible candidates for fertility preservation or more conservative management. Similarly, given the low rates of lymph node involvement, patients with villoglandular adenocarcinoma might need only sentinel lymph node mapping in order to assess for nodal disease.
CONCLUSION
In conclusion, villoglandular adenocarcinoma had more favorable features and better prognosis than standard adenocarcinoma. Less radical surgery or ovarian preservation might be safe for patients with early stage disease. Further investigation of the safety of these approaches is needed
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
J-HC, HD, X-BY and H-WZ contributed equally.
Contributors J-HC, HD, X-BY, HW-Z: protocol/project development, data analysis, and manuscript writing; XC: data collection or management, data analysis; BX-L, PL, Z-QL, L-YP: data collection or management; CC, XY: protocol development, manuscript writing and editing.
Funding This work was supported by funds from the Natural Science Foundation of Zhejiang Province No. Y21H160267 (X-JY), Zhejiang Traditional Chinese Medicine Administration of China No.2020ZB144(X-JY), the Wenzhou Municipal Science and Technology Bureau of China No.Y20190014(X-JY), the National Science and Technology Support Program of China No.2014BAI05B03(C-LC), the National Natural Science Fund of Guangdong No.2015A030311024(C-LC), the Science and the Science and Technology Plan of Guangzhou No.158100075 (C-LC).
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.