Article Text

Abstract
Clear cell carcinoma of the ovary has distinct biology and clinical behavior. There are significant geographical and racial differences in the incidence of clear cell carcinoma compared with other epithelial ovarian tumors. Patients with clear cell carcinoma are younger, tend to present at an early stage, and their tumors are commonly associated with endometriosis, which is widely accepted as a direct precursor of clear cell carcinoma and has been identified pathologically in approximately 50% of clear cell carcinoma cases. The most frequent and important specific gene alterations in clear cell carcinoma are mutations of AT-rich interaction domain 1A (ARID1A) (~50% of cases) and phosphatidylinositol-4,5-bisphosphate 3-kinase catalytic subunit alpha (PIK3CA) (~50% cases). More broadly, subgroups of clear cell carcinoma have been identified based on C-APOBEC (apolipoprotein B mRNA editing enzyme, catalytic polypeptide-like) and C-AGE (age-related) mutational signatures. Gene expression profiling shows upregulation of hepatocyte nuclear factor 1-beta (HNF1β) and oxidative stress-related genes, and has identified epithelial-like and mesenchymal-like tumor subgroups. Although the benefit of platinum-based chemotherapy is not clearly defined it remains the mainstay of first-line therapy. Patients with early-stage disease have a favorable clinical outcome but the prognosis of patients with advanced-stage or recurrent disease is poor. Alternative treatment strategies are required to improve patient outcome and the development of targeted therapies based on molecular characteristics is a promising approach. Improved specificity of the histological definition of this tumor type is helping these efforts but, due to the rarity of clear cell carcinoma, international collaboration will be essential to design appropriately powered, large-scale clinical trials.
- ovarian cancer
- medical oncology
- pathology
- surgery
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
Introduction
Ovarian cancer is a heterogeneous disease and at least five types of epithelial ovarian cancer – high-grade serous, low-grade serous, mucinous, endometrioid, and clear cell carcinomas – are defined at the morphological level, before considering molecular subtypes.1 Much of the historical evidence regarding therapeutic efficacy in ovarian carcinoma either identifies histological type based on poorly reproducible criteria or does not distinguish one type from another.2 Therefore, much of the evidence regarding ovarian cancer treatment reflects the predominant histological type, which is high-grade serous carcinoma.2 However, it is now evident that clear cell carcinoma is a discrete entity, both biologically and clinically, and treatment should be specific for this type. In this review we consider the pathology and clinical behavior of clear cell carcinoma and discuss the extent to which this impacts its management compared with other types of ovarian carcinoma. We also highlight areas where further research is required.
Epidemiology
In the general population, it is estimated that 1.3% of women will develop ovarian cancer in their lifetime.3 There are significant geographical and racial differences in the incidence of clear cell carcinoma, which is higher in Korea (10.3%), Taiwan (18.6%), and Japan (15%–25%)4–7 than in North America and Europe (1%–12%).8 9 The reasons for these differences in incidence are not clear, although molecular differences between tumors arising in different populations have been described; these are discussed in the section on molecular pathology. According to Surveillance, Epidemiology, and End Results (SEER) data, in women living in the United States, the proportion of clear cell carcinoma in whites, blacks, and Asians with epithelial ovarian cancer was 4.8%, 3.1%, and 11.1%, respectively.10 The median age of patients with clear cell carcinoma was significantly younger than that of serous carcinoma of the ovary (55 vs 64 years).10 Clear cell carcinoma is often associated with endometriosis,11 12 and the presence of endometriosis has been associated with a good prognosis.13 Although the molecular mechanisms underlying malignant transformation have not been elucidated fully, endometriosis, particularly ovarian endometriosis, is widely accepted as a direct precursor of endometrioid and clear cell carcinomas of the ovary.14 15 This is supported by data showing that women with histologically proven endometriosis have a significantly elevated age-adjusted incidence rate ratio of 2.29 (95% CI 1.24 to 4.20) for clear cell carcinoma16 and by the identification of endometriosis in the final pathology report in 51% of cases of clear cell carcinoma.17 The incidence of thromboembolic complications, such as deep venous thrombosis and pulmonary embolism, is reported to be higher (up to 40%) in patients with clear cell carcinoma than in those with other ovarian carcinoma types,18 and is considered an independent poor prognostic factor.19 20
Clear cell carcinoma tends to be diagnosed at an earlier stage than serous carcinoma, with 57%–81% and 19%–22%, respectively, presenting at stage I or II.8 10 21 In early stage, especially stage IA and IC1 (rupture alone) disease, the prognosis of clear cell carcinoma patients is good; 5-year disease-free survival rates of patients with stage IA and IC1 clear cell carcinoma were 84%–100% and 86%–89%, respectively.10 21–25 Stage IB clear cell carcinoma is uncommon and data on the prognosis of stage IB clear cell carcinoma are limited. Chan et al reported a 5year disease-specific survival of 56.3% for patients with stage IB clear cell carcinoma, which was significantly lower than other histological types.10 A longitudinal analysis reported a median disease-specific survival of only 10.2 months for advanced-stage (International Federation of Gynecology and Oncology (FIGO) III/IV) clear cell carcinoma cases, compared with over 4 years for the overall clear cell carcinoma population.26 The prognosis of patients with early-stage clear cell carcinoma is similar to or better than that of patients with serous carcinoma.10 27–29 In a review of patients who participated in 12 prospective randomized Gynecologic Oncology Group (GOG) studies, progression-free survival was significantly better in clear cell carcinoma than in serous carcinoma, with a trend towards improved overall survival in stage I and II patients (progression-free survival hazard ratio (HR) 0.69, 95% CI 0.50 to 0.96; overall survival HR 0.76, 95% CI 0.53 to 1.09)29 . In a meta-analysis, there was no significant difference in the HR of overall survival between clear cell carcinoma and serous carcinoma in stage I and II patients (HR 0.87, 95% CI 0.75 to 1.02).30 However, in advanced stage, the prognosis of patients with clear cell carcinoma was remarkably poorer than that of patients with serous carcinoma.21 29–31 In the same review of data from 12 prospective randomized GOG trials, advanced-stage clear cell carcinoma had worse progression-free survival and overall survival compared with advanced-stage serous carcinoma (overall survival HR 1.66, 95% CI 1.43 to 1.91).29 Furthermore, in the meta-analysis, advanced-stage clear cell carcinoma showed a higher HR for death than serous carcinoma (HR 1.71, 95% CI 1.57 to 1.86).30 This poorer outcome for patients with advanced-stage clear cell carcinoma has been confirmed in a study based on SEER data.32
Recurrence of clear cell carcinoma tends to occur at multiple sites, and Hogan et al reported that 38 of 61 patients with recurrent clear cell carcinoma (62%) had multiple-site recurrence involving pelvic, extrapelvic, intrathoracic, lymph node and cerebral/meningeal sites.33 The prognosis of patients with recurrent clear cell carcinoma is poorer than that of patients with recurrent serous carcinoma.34 . When recurrence occurs at a single site, or is restricted to lymph nodes, survival is longer and disease-free interval can be prolonged by surgery; however, this is based on retrospective data.33 This is consistent with the better outcome of patients with isolated lymph node relapse of ovarian carcinoma of all histotypes.35 A retrospective study compared 113 patients with recurrent clear cell carcinoma to 365 patients with recurrent serous carcinoma (type not specified) to estimate long-term clinical outcome. The rate of 5-year post-recurrence survival was significantly lower in recurrent clear cell carcinoma than in recurrent serous carcinoma (13.2% and 18.2%, p<0.0001). On multivariable analysis, there was a significant difference in overall survival between patients with recurrent clear cell carcinoma and recurrent serous carcinoma (HR 2.30, 95% CI 1.72 to 3.07, p<0.0001). In deceased patients with clear cell carcinoma, 67.8% and 93.1% died within 12 and 24 months of recurrence, respectively. In contrast, in deceased patients with serous carcinoma, 40.7% and 73.0% died within 12 and 24 months of recurrence, respectively.34
Definition and Molecular Pathology
Histopathological Diagnosis
The diagnostic criteria for clear cell carcinoma have been refined, enabling more robust and reproducible diagnosis of this tumor type.36–38 Typical cases have characteristic morphological features, including a combination of papillary, tubulocystic, and solid patterns, combined with clear and eosinophilic cells, and stromal hyalinization. The presence of background endometriosis or clear cell adenofibroma is also helpful in supporting the diagnosis. The recognition that other types of ovarian carcinoma, including high-grade serous carcinoma and endometrioid carcinoma, can contain areas with clear cell change has improved the specificity of a clear cell carcinoma diagnosis, which can now be made using a combination of morphological and immunohistochemical features (Figure 1). In particular, clear cell carcinoma is typically positive for napsin A and hepatocyte nuclear factor 1-beta (HNF1β), and negative for Wilms tumor 1 (WT1) and estrogen receptor (ER); high-grade serous carcinoma shows the inverse immunoprofile, and endometrioid carcinoma is negative for napsin A and WT1, and positive for ER.36–38

Histopathological features of clear cell carcinoma. Hematoxylin and eosin (H&E) staining shows (A) papillary and (B) tubulocystic patterns formed by malignant cells with variably clear and eosinophilic cytoplasm. Immunohistochemistry shows a (C) Wilms tumor 1 (WT1)-negative, (D) p53 wild-type, (E) estrogen receptor (ER)-negative, and (F) napsin A-positive immunoprofile.
Molecular Analyses
A number of sequencing analyses have been performed in clear cell carcinoma (Table 1). These results and gene alterations previously reported are summarized in Table 2. The most frequent gene alterations in clear cell carcinoma are in the AT-rich interaction domain 1A (ARID1A)39–44 and phosphatidylinositol-4,5-bisphosphate 3-kinase catalytic subunit α (PIK3CA)39 41–46 genes (both occurring in about 50% of cases).
Next-generation sequencing studies
Summary of critical genetic changes in ovarian clear cell carcinoma
SWI/SNF Chromatin Remodeling Complex
ARID1A encodes ARID1A/BAF250A, which is a key component of the switch/sucrose nonfermentable ATP-dependent (SWI/SNF) chromatin remodeling complex that regulates gene expression targeting multiple tumorigenesis pathways47 . In addition to ARID1A mutation, mutations of ARID1B (6%–18%)41 42 48 and SWI/SNF related, matrix associated, actin dependent regulator of chromatin, subfamily a member 4 (SMARCA4) (5%–18%)41 49 affect the SWI/SNF chromatin remodeling complex.
PI3K/AKT/mTOR Pathway
PIK3CA encodes the catalytic subunit p110α of phosphatidylinositol 3-kinase (PI3K). Somatic mutation of PIK3CA increases PI3K activity and activates the downstream AK strain transforming (AKT) pathway50 . In addition to PIK3CA mutation, mutations of phosphoinositide-3-kinase regulatory subunit 1 (PIK3R1) (7%–10%),41–43 48 51 mutations of phosphatase and tensin homolog (PTEN) (2%–13%),41–44 49 and amplification of AKT serine/threonine kinase 2 (AKT2) (8%–26.6%)41 44 have been reported as genetic changes that affect the PI3K/AKT pathway.50
Combined SWI/SNF and PI3K/AKT/mTOR Alterations
An association between loss of ARID1A expression and activation of the PI3K/AKT pathway in clear cell carcinoma has been reported.52 53 Among 17 clear cell carcinoma cases with PIK3CA mutation, 71% were found in those with loss of ARID1A protein expression.52 Another study showed that the loss of ARID1A expression was more frequent in clear cell carcinoma cases with an activated PI3K/AKT pathway (PIK3CA mutations or loss of PTEN expression) (54%) than those without activation of the PI3K/AKT pathway (30%) (p=0.046).53 According to studies using next-generation sequencing, ARID1A and PIK3CA variants co-occurred in 20%–56% clear cell carcinoma cases,41 44 54 55 and 82% of tumors with activation of the PI3K/AKT pathway were observed in tumors with mutations of the SWI/SNF subunit genes.41 ARID1A and PIK3CA mutations are likely to occur at an early stage in the development of clear cell carcinoma, as they are also detected in endometriosis, which is considered to be a precursor lesion of clear cell carcinoma.14 In a genetically engineered mouse model, loss of ARID1A and activating mutations of PIK3CA were sufficient to generate tumors that phenotypically and molecularly resembled human clear cell carcinoma.56
Mitogen-Activated Protein Kinase (MAPK) Pathway
Genetic changes in the mitogen-activated protein kinases (MAPK) pathway, such as mutation of protein phosphatase 2 scaffold subunit alpha (PPP2R1A) (4.1%–20%)39 42–44 57 and the KRAS proto-oncogene, GTPase (KRAS) (4.7%–20%);39 41–45 54 55 mutation and amplification of erb-b2 receptor tyrosine kinase 2 (ERBB2) (4%–13%);41 44 49 54 55 and amplification of the MET proto-oncogene (MET) (24%–37%)58 59 have been reported.
TP53, Homologous Recombination Deficiency, and Telomerase
Unlike high-grade serous carcinoma, clear cell carcinomas usually express wild-type p53 protein and have a lower frequency of BRCA1 and BRCA2 mutations;41 44 BRCA mutations have been identified in approximately 6% (1% germline, 5% somatic) of cases, and mutations in homologous recombination pathway genes in up to 28% overall.60 The frequency of TP53 mutations in clear cell carcinoma has been reported to be approximately 8.5%–21.6%.43–45 49 55 It is possible, however, that some of the TP53 and BRCA1-mutated carcinomas categorized as clear cell carcinoma in these cohorts are high-grade serous carcinomas with areas of clear cell change. Clear cell carcinoma has a higher frequency of telomerase reverse transcriptase (TERT) promoter mutation (5.7%–16.0%) than other histological types of epithelial ovarian cancer.61 62 TERT promoter mutation does not appear to be an early event in the carcinogenesis of clear cell carcinoma, as it was not observed in endometriosis progressing to clear cell carcinoma.61
Mutational Signatures
Two major subgroups of clear cell carcinoma have been identified based on mutational signatures: C-APOBEC, characterized by an apolipoprotein B mRNA editing enzyme, catalytic polypeptide-like (APOBEC) mutation signature (26%), and C-AGE, characterized by an age-related (AGE) mutation signature (40%).43 Consistent with this, another study reported an APOBEC signature in 18% of clear cell carcinoma.48 The APOBEC mutational process has been proposed as a therapeutic target to prevent ongoing clonal evolution in disease progression.63 A multi-region sequencing study showed APOBEC-mediated kataegis to be an early event in clear cell carcinoma development, with APOBEC3B expression associated with infiltration by cytotoxic T cells and favorable outcome. Moreover, in another study, APOBEC3B overexpression was shown to associate with improved clinical outcome in clear cell carcinoma and to have a potential role in predicting response to platinum-based chemotherapy.64
Copy-Number Alterations
The total number of copy-number alterations in clear cell carcinoma is similar to that in low-grade serous carcinoma,65 and much lower than in high-grade serous carcinoma.65 66 Conversely, the ratio of whole-arm copy-number alterations in clear cell carcinoma was significantly higher than in serous carcinoma.66 Whole-arm copy-number alterations at 8q in clear cell carcinoma were also reported in other studies.42 67 The most remarkable region with copy-number gain in clear cell carcinoma is at chr20q13.2, which includes a potential oncogene, zinc finger protein 217 (ZNF217), at a frequency of 20%–36%.65 68 69 ZNF217 was amplified significantly more frequently in Japanese (62%) than in Korean (7%) or German (25%) clear cell carcinoma,67 and high-level amplification of ZNF217 was identified in C-APOBEC (33%) and C-AGE (57%) tumors.43 Moreover, ZNF217 amplification in clear cell carcinoma correlated significantly with shorter progression-free survival (HR 2.6, 95% CI 1.1 to 6.1, p=0.339) and overall survival (HR 3.5, 95% CI 1.1 to 10.6, p=0.031).68 The association between ZNF217 and SWI/SNF is controversial. Loss of ARID1A expression has been reported to be coincident with PI3K-AKT pathway activation and/or ZNF217 amplification.53 Conversely, in another study, the cases positive for all SWI/SNF subunits demonstrated significantly greater DNA copy-number alterations, such as amplification of chromosomes 20q.13.2-20q13.33 (including ZNF217) and 8q.24.3, and deletion of chromosomes 13q12.11-13q14.3 (including RB1), 17p13.2–17 p13.1 (including TP53), and 19p13.2–19 p13.12.70
Transcriptomic Analyses
Previous microarray analyses have identified a clear cell carcinoma expression profile that is distinct from other histological types of ovarian carcinoma.66 71 72 HNF1β and oxidative stress-related genes are upregulated in clear cell carcinoma.73 74 Microarray analysis classified clear cell carcinoma into three clusters, and co-existent alterations of PIK3CA and ARID1A were commonly observed in two of these (7/11, 64%) but not in the third (0/10, 0%; p<0.01). Being in the cluster without co-existent PIKCA and ARID1A alteration was an independent favorable prognostic factor.66 Unsupervised gene expression analysis of clear cell carcinoma has identified two gene transcriptomic subtypes associated with differential outcome, termed epithelial- and mesenchymal-like.75 The epithelial-like subgroup, which had a high frequency of SWI/SNF complex mutations, was associated with early stage at diagnosis and favorable outcome, while the mesenchymal-like group was enriched for advanced-stage disease at diagnosis and overall poor prognosis.
Clinical Aspects
Diagnosis
As described above, the morphological features of clear cell carcinoma are often typical and diagnostic; and the addition of immunohistochemistry for WT1, p53, napsin A, and HNF1β helps to ensure diagnostic specificity by allowing the exclusion of, in particular, high-grade serous carcinoma with clear cells.36–38 70 It is important that clear cell carcinoma is defined robustly both in clinical practice and in molecular and clinical studies to ensure that patients are managed appropriately, and therapeutic responses and outcomes are accurately determined.
Surgery
Tumor stage is an important determinant of outcome and is crucial for clinical management. Lymphadenectomy is necessary to determine the precise stage because the rate of lymph node metastasis has been reported to be 4.5%–14.4% in pT1 (tumor limited to ovaries (one or both)) or pT2 (tumor involving one or both ovaries with pelvic extension) clear cell carcinoma.22 76–78 In the Multicentre Italian Trials in Ovarian Cancer (MITO-9) retrospective study, disease-free survival was longer in patients undergoing lymphadenectomy at surgery, both in early-stage (p=0.026) and in advanced-stage (p=0.004) disease. Lymphadenectomy was independently associated with longer overall survival (HR 0.15, 95% CI 0.04 to 0.54) in multivariate analysis,79 although stage shift is clearly a possible confounding factor in this study. Other studies have failed to show the therapeutic benefit of lymphadenectomy for early-stage clear cell carcinoma23 76 78 and further studies are required to determine the impact of lymphadenectomy in this context.
Although it has been reported that residual disease after cytoreductive surgery is a strong predictor of survival in advanced-stage epithelial ovarian cancer, the proportion of clear cell carcinomas in these reports is low (3.3%–4.8%).31 80–82 There are, however, a few reports that examine an association between residual tumor and prognosis in clear cell carcinoma. Takano et al performed a retrospective analysis to evaluate the clinical characteristics and prognostic factors in the 254 patients with clear cell carcinoma of the ovary. There was no significant prognostic difference between patients with residual tumor diameter <1 cm and those with residual tumor diameter >1 cm (p=0.40). Patients with no residual tumor had significantly better progression-free survival than those with residual tumor <1 cm (p=0.04) or those with residual tumor diameter >1 cm (p<0.01), and only residual tumor diameter was an independent prognostic factor in advanced-stage clear cell carcinoma (p=0.02).22 Furthermore, Melamed et al conducted a retrospective cohort study to quantify the magnitude of associations between residual disease status and all-cause mortality by histological type using data from the National Cancer Database of America. Overall survival differed significantly according to residual disease status not only in patients with high-grade serous carcinoma but also in those with clear cell carcinoma and, while not statistically significantly different, the survival benefit associated with cytoreduction to no residual disease was greater in clear cell carcinoma (HR 0.39, 95% CI 0.22 to 0.69) than in high-grade serous carcinoma (HR 0.58, 95% CI 0.49 to 0.68).83 Surgery to achieve no residual tumor may be necessary to improve the prognosis in advanced-stage clear cell carcinoma.
As clear cell carcinoma is found at early stage and at a younger age, fertility sparing is an important consideration in clinical practice. According to a summary of studies on fertility-sparing surgery in stage I clear cell carcinoma, there was no difference in the recurrence rate between patients with clear cell carcinoma and non-clear cell carcinoma (7/53, 13.2% and 41/377, 10.9%; p=0.61).84 However, in another report, the recurrence rate of stage IC clear cell carcinoma patients who underwent fertility-sparing surgery was 22.5% (7/31).85 The role for fertility-sparing surgery in stage 1B is unclear from existing data. Therefore, fertility-sparing surgery may be an option at least for patients with stage IA clear cell carcinoma when adequate staging is conducted. A recent systematic review supports this conclusion, identifying that fertility sparing surgery is not associated with worse survival in patients with stage I disease.86
Chemotherapy
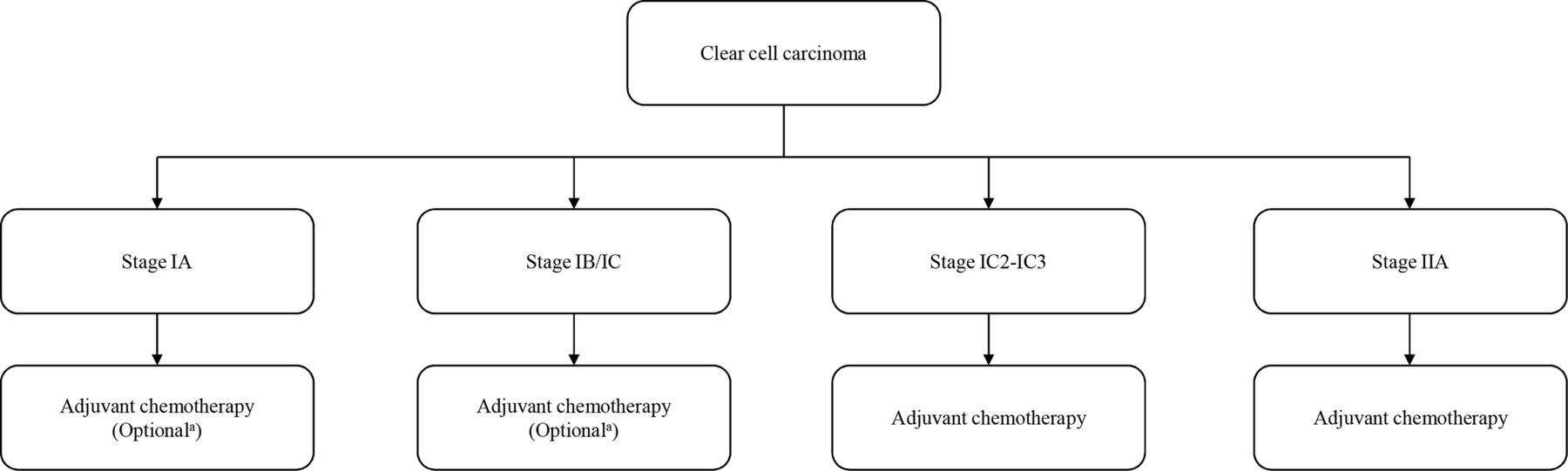
Current National Comprehensive Cancer Network (NCCN) guidelines for the management of clear cell carcinoma are summarized in Figure 2.87 Although previous NCCN guidelines recommended adjuvant chemotherapy for clear cell carcinoma regardless of disease stage,88 current European Society for Medical Oncology-European Society of Gynaecological Oncology (ESMO-ESGO) consensus conference recommendations on ovarian cancer indicate that the benefit of adjuvant chemotherapy is uncertain for patients with stage IA, IB, and IC1 clear cell carcinoma, and no adjuvant chemotherapy is recommended for patients with stage IA, IB, and IC1 clear cell carcinoma with complete surgical staging (Figure 3).89 The current NCCN ovarian cancer guidelines also state that observation is an option for patients with IA clear cell carcinoma who have undergone complete surgical staging (Figure 2).87 The subset analysis in the ACTION study showed similar progression-free survival for patients with stage I-IIA clear cell carcinoma with or without adjuvant chemotherapy,90 and two retrospective analyses reported no benefit for adjuvant chemotherapy after complete surgical staging for stage IA-B clear cell carcinoma.91 92 Furthermore, a large-scale study based on SEER data revealed that there was no significant difference in 5-year overall survival between the patients with stage I clear cell carcinoma who received adjuvant chemotherapy (85%) and those who did not (83%) (p=0.43). This was also true for substage IC clear cell carcinoma, where there was no significant difference in 5-year overall survival between the patients who received adjuvant chemotherapy (83%) and those who did not (80%) (p=0.62).93 However, a systematic review and meta-analysis identified that adjuvant chemotherapy correlated with improved overall survival in patients with stage IC (odds ratio (OR) 0.70, 95% CI 0.52 to 0.93) but not stage IA or IB disease.94

National Comprehensive Cancer Network (NCCN) guidelines version 1.2020 for clear cell carcinoma of the ovary.87 IP, intraperitoneal; IV, intravenous.

{kind=link}
{kind=link}
{kind=link}
Adjuvant chemotherapy for patients with early-stage clear cell ovarian cancer (stage I-IIA). From European Society for Medical Oncology-European Society of Gynaecological Oncology (ESMO-ESGO) consensus conference recommendations on ovarian cancer.89 aNo adjuvant chemotherapy should be considered only for patients with complete surgical staging.
A study of 210 patients showed that there was no impact of three versus six cycles of chemotherapy on overall survival in early-stage clear cell carcinoma.95 Further studies of early-stage disease are required to determine which stages of disease benefit from chemotherapy and how many cycles of adjuvant chemotherapy are appropriate. At present, the Japanese Gynecologic Oncology Group (JGOG) is performing a randomized phase III trial to evaluate the necessity of adjuvant chemotherapy in stage I epithelial ovarian cancer (stage IA/IB clear cell carcinoma or grade 2/3 other histological type and stage IC1 with all grades and histological types) after comprehensive staging surgery (JGOG3020, UMIN000008481). It is hoped that this trial will shed more light on the role of chemotherapy in stage IA/IC1 clear cell carcinoma.
In first-line chemotherapy for clear cell carcinoma, the response rate to a combination of paclitaxel plus platinum, which is standard therapy for ovarian carcinoma, is thought to be higher (22%–56%) than that of other platinum-based chemotherapy (11%–27%).21 22 96–99 However, the addition of taxane was not an independent prognostic factor in the MITO-9 study,79 and there was no survival benefit in advanced-stage clear cell carcinoma between patients treated with paclitaxel plus platinum compared with those treated with platinum monotherapy in a large Japanese study.22 A randomized phase III study of paclitaxel and carboplatin versus dose-dense paclitaxel and carboplatin as a first-line treatment for stage II-IV epithelial ovarian cancer showed that dose-dense paclitaxel and carboplatin offers better survival than paclitaxel and carboplatin in ovarian cancers unselected for histological type.100 However, in subgroup analysis of this study, there was no significant survival benefit in patients with clear cell or mucinous tumors between treatment groups.100 Conversely, combination therapy with irinotecan hydrochloride and cisplatin has been reported to be effective as first-line and second-line chemotherapy for clear cell carcinoma.101 102
A randomized phase II study (JGOG3014) to compare combination therapy with irinotecan hydrochloride and cisplatin and paclitaxel/carboplatin revealed that completion rates of six cycles and 5-year progression-free survival were similar in both arms.103 A subsequent randomized phase III study of combination therapy with irinotecan hydrochloride and cisplatin versus paclitaxel/carboplatin as first-line treatment for clear cell carcinoma was conducted by the JGOG in collaboration with the Gynecologic Cancer Intergroup (GCIG; JGOG3017/GCIG Trial). However, there was no significant survival benefit with combination therapy with irinotecan hydrochloride and cisplatin; 2-year progression-free survival rates were 73.0% in the combination therapy with irinotecan hydrochloride and cisplatin group and 77.6% in the paclitaxel/carboplatin group (HR 1.17, 95% CI 0.87 to 1.58).104
In second-line or salvage chemotherapy, the response rate for recurrent or refractory clear cell carcinoma is extremely low.96 97 105–108 In a large-scale study of platinum-sensitive relapsed ovarian carcinoma, including all histological types, the response rates of patients treated with paclitaxel plus platinum chemotherapy and those with other platinum-based chemotherapy were 66% and 54%, respectively.109 However, even in patients with ‘platinum-sensitive’ relapsed clear cell carcinoma, the response rate was lower than 10%.105 106 In a retrospective study of 75 patients with recurrent or refractory clear cell carcinoma, the median overall survival of patients after platinum-sensitive or platinum-resistant relapse were 16 months and 7 months, respectively (p=0.04).106 Chemotherapy for recurrent or refractory clear cell carcinoma therefore has only small benefit, especially in platinum-resistant relapse.
Radiotherapy
Adjuvant radiotherapy may improve the prognosis of early-stage clear cell carcinoma. In a retrospective analysis of stage IC, II, and III clear cell carcinoma to compare chemotherapy (cyclophosphamide, adriamycin, and cisplatin) and whole abdominal radiotherapy, overall survival and disease-free survival were significantly superior in the whole abdominal radiotherapy group to those in the chemotherapy group.110 Furthermore, a large-scale retrospective analysis of 241 patients with stage I and II clear cell carcinoma to compare adjuvant chemotherapy (three-cycle paclitaxel/carboplatin) followed by radiation (22.5 Gy to pelvis followed by 22.5 Gy to the whole abdomen) and chemotherapy (six-cycle paclitaxel/carboplatin) only, there was a significant improvement in disease-free survival by 20% at 5 years within stage IC (all IC patients except those who were IC by virtue of rupture alone) and stage II.25 Conversely, in a more recent retrospective study of 163 patients with stage I and II clear cell carcinoma, adjuvant radiotherapy was not significantly associated with increased progression-free or overall survival either in the whole group or even in the high-risk group (stage IC2, IC3, and II).111 The latter study was more likely to be subject to selection bias than the former as, in the former study, the decision to treat with chemo-radiotherapy or chemotherapy alone was based on service factors rather than patient factors. Further research is needed to determine the benefit of radiotherapy in early-stage clear cell carcinoma.
Radiotherapy may have a role in the treatment of patients with locoregionally recurrent clear cell carcinoma.112 113 One retrospective study of involved-field radiation therapy found higher 5-year overall survival (88% vs 37%, p=0.05) and disease-free survival (75% vs 20%, p=0.01) in eight patients with clear cell carcinoma compared with other histological types.114
Targeted Therapy
Some agents targeting angiogenesis (bevacizumab, sunitinib, nintendanib), the PI3K/AKT/mTOR pathway (temusirolimus), immune checkpoints (nivolumab, durvalumab), loss of BAF250a (dasatinib), Aurora A (ENMD-2076), and MET (cabozantanib) are currently being evaluated in clinical trials, either as monotherapy or in combination with other targeted/cytotoxic agents (Table 3).
Clinical trials of clear cell carcinoma using molecular targeted therapy
Bevacizumab was the first targeted therapy to receive the approval of the European Medicine Agency for the treatment of epithelial ovarian cancer. ICON7, a phase III randomized study, assessed bevacizumab combined with carboplatin and paclitaxel in the upfront setting compared with carboplatin and paclitaxel alone. This study included patients with stage I or IIA clear cell carcinoma and no benefit of bevacizumab was reported for clear cell carcinoma in a subgroup analysis,115 although this analysis was very underpowered and cannot be taken as evidence for absence of an effect of bevacizumab in clear cell ovarian carcinoma. The vascular endothelial growth factor receptor (VEGFR) inhibitor sunitinib demonstrated minimal activity in a phase II trial of patients with recurrent clear cell carcinoma as the second- or third-line treatment, with a response rate of 6.7%.116
Temsirolimus, an inhibitor of mammalian target of rapamycin (mTOR), was evaluated in a phase II trial in combination with carboplatin and paclitaxel as first-line therapy in the treatment of stage III-IV clear cell carcinoma of the ovary. This regimen did not statistically significantly increase progression-free survival compared with historical control.117 In a study of nivolumab, an immune checkpoint inhibitor that blocks programmed cell death 1 (PD-1), for platinum-resistant ovarian carcinoma, one of two patients with clear cell carcinoma exhibited complete response and, in a study of avelumab for recurrent/refractory ovarian carcinoma, both patients with clear cell carcinoma exhibited partial response.118 119 Immune checkpoint inhibitors may represent a new treatment option for clear cell carcinoma, and clinical trials using these are ongoing.
ENMD-2076, an oral multitarget kinase selective against Aurora A and VEGFR, was evaluated for its activity in patients with recurrent ovarian clear cell carcinoma in a phase II study. The overall 6-month progression-free survival rate was 22% and did not meet the preset threshold for efficacy.120 Besides these agents, it has been reported that a histone deacetylase (HDAC) inhibitor and an enhancer of zeste homologue 2 (EZH2) inhibitor selectively suppressed the growth of ARID1A-mutated cells in vitro and in vivo,121 122 and these drugs are expected to be introduced into clinical trials. In a small study, high HDAC6 expression correlated with poor prognosis in clear cell carcinoma with ARID1A loss, and also with programmed death-ligand 1 (PD-L1) expression.123 This is consistent with the demonstration that HDAC6 inhibition can synergize with anti-PD-L1 therapy in a mouse model, raising the possibility that this combination may represent a novel therapeutic strategy.124
In early work, prolyl hydroxylase domain-containing protein 2 (PHD2), encoded by EGLN1, has been identified as a potential hypoxia-inducible factor 1α (HIF1A)-dependent therapeutic target in clear cell carcinoma;125 and screening of ARID1A-deficient cells has suggested that gemcitabine may be an effective therapeutic option in ARID1A-deficient tumors.126
Post-Treatment Surveillance
Current NCCN guidelines do not recommend clear cell carcinoma-specific post-treatment surveillance;87 patients are followed up in the same way as patients with other histological tumor types. However, the ESMO-ESGO consensus conference recommendations on ovarian cancer indicate that CA125 is not a reliable marker in epithelial ovarian carcinoma types other than high-grade serous carcinoma.89
Future Directions
The improved definition of ovarian clear cell carcinoma, and greater understanding of its molecular characteristics, provide opportunities to develop alternative treatment strategies with the aim of improving survival, particularly of patients with advanced-stage or recurrent disease. Possible individualized investigational approaches based on tumor biology are suggested in Table 4. Due to the rarity of clear cell carcinoma, international collaboration will be essential to power large-scale clinical trials required to answer the many remaining questions regarding the optimal treatment of this disease. Accurate diagnosis, particularly the exclusion of clear cell carcinoma mimics such as high-grade serous carcinoma with clear cells, will be crucial for these trials to produce reliable findings. Specific areas that merit further investigation include the relationship between mismatch repair (MMR) deficiency and response to immune checkpoint inhibitors, the prevalence of BRCA mutation and its relationship to poly-ADP ribose polymerase (PARP) inhibitor response, and the development of novel therapies based on tumor biology.
Possible individualized investigational approaches to the treatment of metastatic or recurrent clear cell ovarian cancer.
Acknowledgments
The authors would like to extend their thanks to the Nicola Murray Foundation for their generous support of the authors' laboratory, and the NHS Lothian Department of Pathology.
References
Footnotes
Correction notice This article has been corrected since it was published Online First. The author name Robert L Hollis was incorrectly written as Robb Hollis. This has now been amended.
Contributors YI drafted the manuscript. CSH provided the figure. AO, RLH, CG, and CSH reviewed and edited the manuscript. All authors approved the submitted version.
Funding RLH is supported by Target Ovarian Cancer and the Medical Research Council (MRC). This work was also supported by a charitable donation from the Nicola Murray Foundation and by Cancer Research UK.
Competing interests CG discloses the following: research funding from AstraZeneca, Aprea, Nucana, Tesaro, and Novartis; honoraria/consultancy fees from Roche, AstraZeneca, Tesaro, Nucana, MSD, Clovis, Foundation One, Sierra Oncology, and Cor2Ed; named on issued/pending patents relating to predicting treatment response in ovarian cancer beyond the scope of this work.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.