Article Text

Statistics from Altmetric.com
Case presentation
Dr Marchocki
A 39-year-old, G0P0 woman was referred to the gynecologic oncology clinic following a diagnosis of ovarian serous low malignant potential tumor on a biopsy specimen taken during work-up for primary infertility. She had been seen by the infertility specialist 4 months prior to the current presentation with a 2-year history of primary infertility. The patient had no significant medical history and no prior surgeries at that time. Family history was significant for a maternal aunt who had breast cancer in her 40s and maternal grandfather who had prostate cancer. Pelvic ultrasound performed as part of the initial infertility work-up 4 months prior to the oncologic referral showed echogenic solid area in the right adnexa measuring 3.2×2.0 x 2.4 cm adjacent to the right ovary, a normal left ovary, a 2.5×2.4 x 1.9 cm submucosal uterine fibroid, and possible uterine septum. The patient was referred by the fertility specialist to a general gynecologist for surgical management and underwent a diagnostic laparoscopy, biopsy of a right ovarian lesion, excision of a paratubal cyst, and hysteroscopic uterine myomectomy. Significant pelvic and peri-hepatic adhesions were noted on laparoscopic assessment.
Dr Rouzbahman
Microscopic examination of the right ovarian biopsy showed papillary proliferation with hierarchical branching architecture lined by cuboidal to columnar epithelium with minimal nuclear atypia, in keeping with a serous low malignant potential tumor. No micropapillary architecture or evidence of stromal invasion were identified. The endometrial curetting contained proliferative endometrium and fragments of submucosal leiomyoma. Cytological examination of the pelvic washings showed serous neoplasm.
Dr Marchocki
In view of these findings, the patient was referred to the gynecologic oncology service where she was seen in consultation.
Given the findings on pathology, what would be your recommendation as it pertains to additional evaluation? Is there a role for re-operation if no evidence of disease is found on imaging and, if not, is there any patient for whom one should consider re-operation?
Dr May
This patient has a tissue diagnosis of serous low malignant potential tumor that was incompletely excised. The initial work-up included epithelial tumor markers and computed tomography (CT) of the chest, abdomen, and pelvis. Although radiologic staging is helpful to evaluate the extent of disease, it does not substitute for a surgical assessment. In young patients with disease that appears localized to the adnexa on imaging, ovarian cystectomy or unilateral salpingo-oophorectomy might be appropriate if fertility preservation is desired. In women with bilateral ovarian involvement, either bilateral ovarian cystectomies or unilateral salpingo-oophorectomy with contralateral ovarian cystectomy might be considered, when feasible. Patients should be counseled that cystectomy for apparent clinical stage I disease is associated with a higher risk of ipsilateral or contralateral adnexal recurrence compared with oophorectomy.1 In a meta-analysis examining the risk of recurrence associated with different surgical procedures, Vasconcelos and de Sousa Mendes demonstrated that patients treated with unilateral cystectomy, bilateral cystectomies, unilateral salpingo-oophorectomy, or unilateral salpingo-oophorectomy with contralateral cystectomy for serous low malignant potential tumors had pooled recurrence rates of 25.3%, 25.6%, 12.5% and 26.1%, respectively.1 In cases where bilateral salpingo-oophorectomy is necessary, the conservation of the uterus might allow for future pregnancy with previously frozen embryos or donor eggs. It is prudent to advise patients that conserving ovarian tissue may be associated with a 10%–20% risk of recurrence, with the majority of the recurrences occurring within the residual ovarian tissue and 2% in extra-ovarian locations within the peritoneal cavity.2 3 In comparison, patients treated with radical non-fertility preserving surgery have lower relapse rates of approximately 5%, largely within the peritoneal cavity.2
Significantly, the majority of recurrences in women with a history of serous low malignant potential tumors are in the form of recurrent low malignant potential tumors and few are in the form of invasive carcinoma.2 Factors associated with increased risk of recurrence include tumor microinvasion, presence of invasive or non-invasive implants, advanced International Federation of Gynceology and Obstetrics (FIGO) stage, residual disease, and incomplete surgical staging.2 4 5 Traditional comprehensive surgical staging consists of hysterectomy, bilateral salpingo-oophorectomy, omentectomy, peritoneal washing, and peritoneal biopsies.2 Although the likelihood of identifying positive lymph nodes is between 21% and 29% in low-grade tumors, the clinical benefit of systematic pelvic and para-aortic lymphadenectomy is questionable since patients with positive or negative lymph nodes have similar recurrence and survival rates.5 Complete surgical staging in clinically early stage disease and comprehensive surgical cytoreduction in clinically advanced stage disease allow thorough histo-pathological assessment, exclusion of invasive cancer, and post-operative risk stratification. As the prognosis of patients with low malignant potential tumors is good, the laparoscopic approach has been suggested especially in fertility sparing settings. However, concerns remain regarding inadequate staging, cyst rupture, dissemination of tumor cells, and port site metastases, particularly in patients with invasive disease.
Dr Marchocki
Given the patient’s desire for fertility preservation, she underwent pre-operative oocyte retrieval and in vitro fertilization with successful embryo freezing prior to the definitive completion surgery. She developed ovarian hyperstimulation syndrome and required multiple paracenteses. Peritoneal cytology showed serous neoplastic cells not otherwise specified.
Is there a concern for increased risk of tumor spread or cancer recurrence in patients undergoing oocyte retrieval and in vitro fertilization in the setting of low malignant potential tumors or in the setting of documented invasive cancer?
Dr May
The association between fertility therapies and gynecologic malignancies has been extensively studied with variable results. Two large case–control studies reported no significant increased risk of ovarian cancer among most women treated with fertility drugs when controlling for known confounders.6 7 In contrast, a recently published Cochrane review showed a slight increase in ovarian cancer risk in sub-fertile women treated with infertility drugs when compared with either the general population or with sub-fertile women who did not receive fertility treatments.8 The risk appears to be related to ovarian stimulating medications and the subsequent hormonal changes they cause. Given that up to 96% of serous low malignant potential tumors express estrogen and progesterone receptors, they are susceptible to these hormonal fluctuations.9 Some women appear to be at higher risk of developing ovarian neoplasms following fertility treatments including long-term fertility drug users, women who remain nulligravid after fertility treatment, women with Breast Cancer Antigen (BRCA) 1 or BRCA2 mutations, and patients with a history of low malignant potential tumors.6 7 Moreover, follicle aspiration may cause cystic tumor rupture and spill as well as iatrogenic seeding of cancer cells. This is particularly relevant for patients with known or suspected malignancy where the abnormal ovary should not be targeted for oocyte retrieval to avoid tumor spill or iatrogenic seeding. Lastly, if malignancy is suspected, the delay in definitive cancer treatment should be considered when discussing possible fertility treatments. These delays are unlikely to impact long-term survival outcomes in patients with low-grade neoplasms and are more relevant to high-grade histologies.
Please provide a detailed and comprehensive description and provide images of the findings noted on CT scans.
Dr Chawla
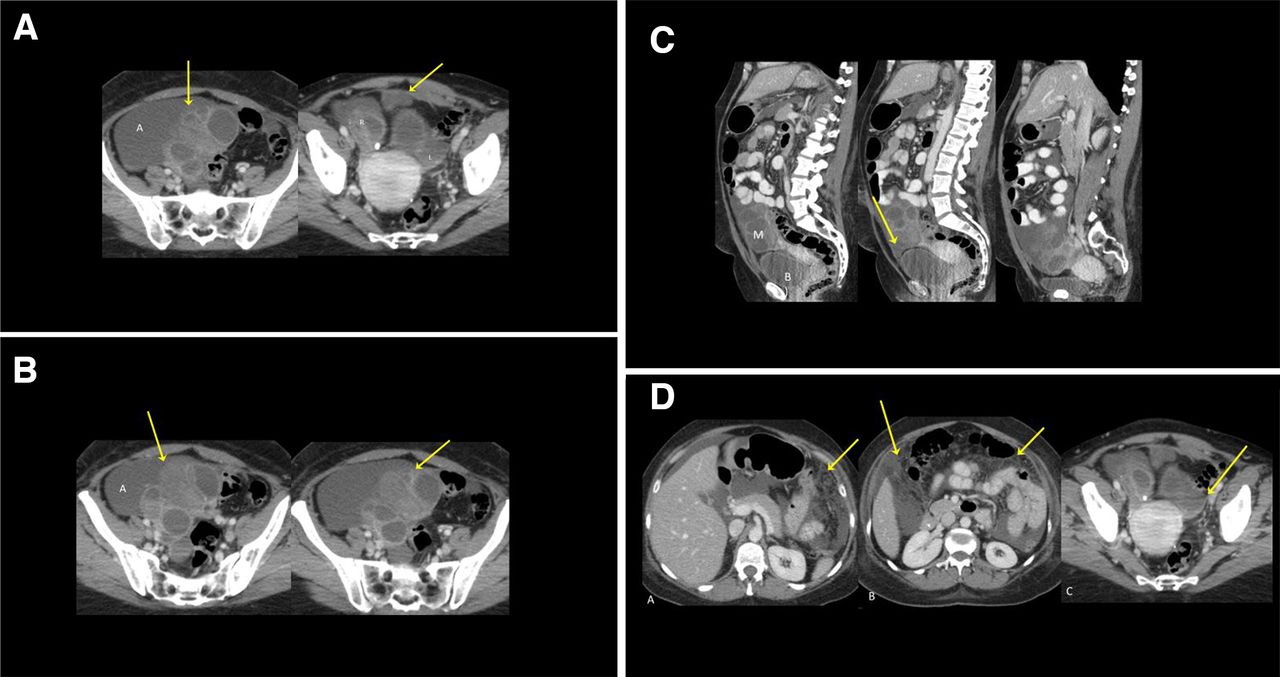
Pre-operative portal venous phase CT of the abdomen and pelvis performed after the patient completed fertility treatment showed the presence of bilateral adnexal masses (Figure 1). These lesions were multi-loculated and had cystic and solid components bilaterally. The right-sided adnexal lesion measured up to 8.9×7.2 x 6.6 cm and the left-sided adnexal mass measured up to 8×7.2 x 6.6 cm. Within the limitations of CT, the uterus, endometrium and cervix appeared unremarkable. There was a moderate volume of ascites with generalized peritoneal stranding in the omentum and mesentery (Figure 1). Specifically, nodularity was seen in locations such as superficial to the bladder dome, within the sigmoid mesentery, and within the ileocolic mesentery. There was no evidence of any large size adenopathy in the abdomen or pelvis. The solid organs were unremarkable and there was no evidence of any hydronephrosis. CT chest demonstrated some borderline nodes in the right internal mammary and left supraclavicular chains; there was no other measurable disease within the thorax.

(A) Axial view of the pelvis showing the presence of moderate ascites. There are bilateral (R and L) adnexal masses present. There is a cystic implant in the space of Retzius close to the dome of the urinary bladder (arrow). (B) Portal venous phase (PVP) scan through the pelvis shows the right-sided adnexal mass. It is multi-loculated. Note the locules are of differential attenuation reflecting cystic and solid components (arrows). Note ascites surrounding the mass (A). (C) Sagittal images showing the adnexal mass (M) and its relationship to the urinary bladder (B) as well as a cystic implant cranial to the urinary bladder (arrow). Note small to moderate quantities of ascites and the generalized peritoneal thickening. (D) Arrows (in images A and B) indicate the presence of peritoneal stranding in the gastrocolic and infracolic omentum in keeping with disease. Image C shows a loculated implant in the posterior cul de sac (arrow). Note the overlying enhancement in this location.
Dr Marchocki
Pre-operative tumor markers indicated elevated Cancer Antigen 125 (CA125) of 279 U/mL, normal Carcinoembryonic Antigen (CEA) of 1.8 µg/L, and normal Carbohydrate Antigen 19–9 (CA19-9) of 19 kU/L. The patient was counseled regarding treatment options and elected to proceed with surgical management. She was consented for a midline laparotomy, cytoreductive surgery with possible unilateral or bilateral salpingo-oopherectomy, possible hysterectomy, omentectomy, peritonectomy, and possible bowel resection.
Given the patient’s desire for future fertility, what would be the frame of the discussion regarding what will be done at the time of surgery? How would you use intra-operative frozen section in this setting?
Dr May
Surgical cytoreduction in patients with a pre-operative diagnosis of advanced low-grade serous ovarian neoplasms serves a diagnostic and therapeutic purpose. It is imperative to remove all the visible disease so it can undergo pathologic assessment to define whether the lesions are pre-invasive or invasive. Frozen section has intra-operative limitations as it may not accurately distinguish between low malignant potential tumors and low-grade serous ovarian carcinoma.10 In fact, the intra-operative frozen section diagnosis is amended in up to one-third of low-grade neoplasms.10 If an invasive component cannot be identified by the pathologist intra-operatively, then conservative surgery is recommended in the setting of desired fertility preservation. We advocate resecting all visible disease to obtain complete cytoreduction which is associated with highest survival advantage and lowest risk of recurrence.2 11 This may include unilateral or bilateral salpingo-oopherectomy if both adnexa are involved, hysterectomy if the uterus is directly involved by tumor, omentectomy, peritonectomy, excision of enlarged lymph nodes, and bowel resection. Importantly, if the contra-lateral ovary appears clinically uninvolved and is left in situ, the patient should be aware of the limitations of frozen sections in these neoplasms and of the possibility of requiring additional surgery should the final pathology indicate a malignancy. In cases where the final pathology diagnosis is low-grade serous ovarian carcinoma, the patient would benefit from bilateral salpingo-oopherectomy for surgical completion and to eliminate the hormonal secretion by the residual ovary.
Dr Marchocki
The patient was taken to the operating room for surgical cytoreduction. An exploratory laparotomy revealed an 8 cm papillary right adnexal mass invading the mesentery of the distal ileum, the right pelvic sidewall peritoneum, the cul de sac peritoneum, and the rectosigmoid mesentery. A 10 cm left papillary adnexal mass was present on the superior aspect of the uterine fundus without direct uterine serosal invasion. There was an additional 8 cm wide and 4 mm thick peritoneal plaque overlying the anterior bladder peritoneum. Borderline enlarged, mobile retroperitoneal nodes were palpated. A 4 cm right paracolic gutter lesion was identified lateral to the cecum. Omental thickness was noted without clinically evident omental deposits. Two liters of ascites were identified and aspirated. Frozen section examination of the left adnexal mass, the right adnexal mass and the cul de sac lesion showed low-grade serous ovarian neoplasm not otherwise specified. Final diagnosis was deferred to permanent pathology. Complete cytoreduction to no evidence of residual disease was achieved by performing bilateral salpingo-oophorectomy, small bowel resection of the distal ileum with primary side-to-side re-anastomosis, excision of enlarged pelvic and para-aortic lymph nodes, excision of sigmoid mesenteric tumor, excision of anterior bladder peritoneum tumor, pelvic peritonectomy and omentectomy. As there was no evidence of uterine serosal invasion, the uterus was left in situ. The patient had an uneventful post-operative recovery course and was discharged home on post-operative day 6 in a stable medical condition.
Dr Rouzbahman
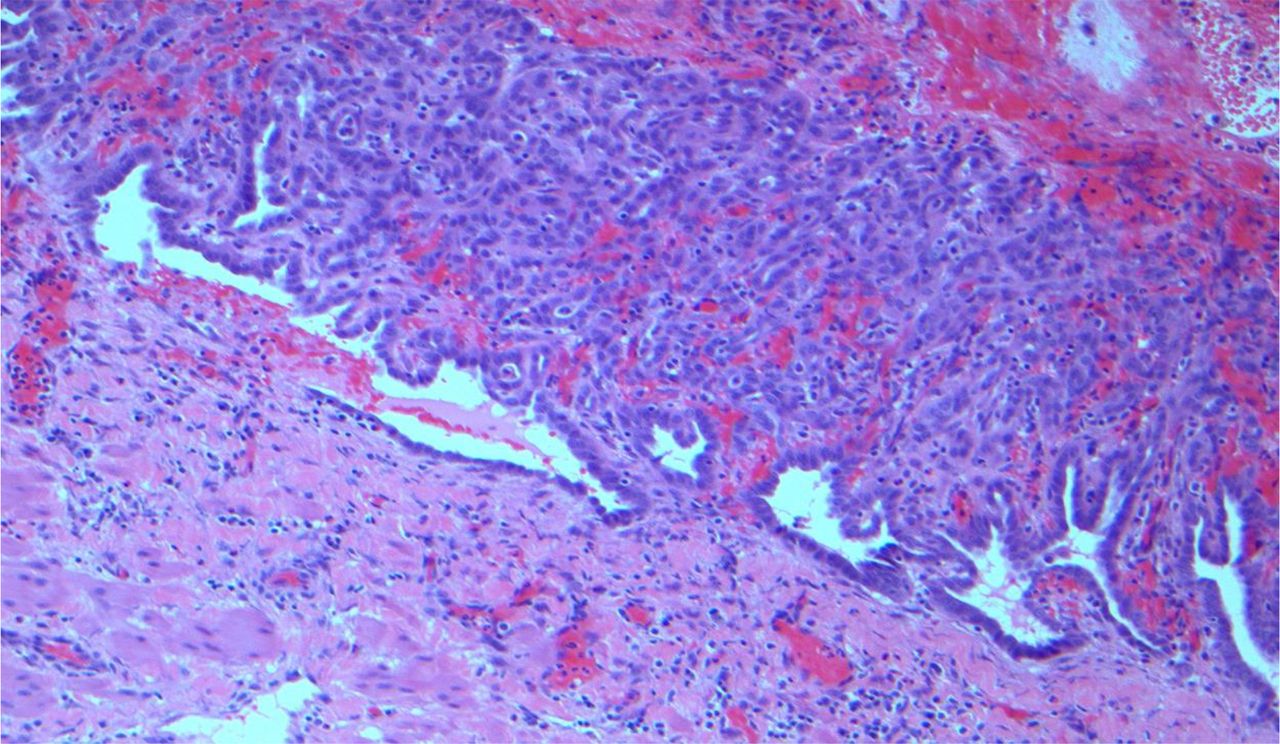
Pathologic examination of the bilateral salpingo-oophorectomy specimen revealed a left ovarian mass measuring 10.8×7.2 x 3.1 cm and a right ovarian mass measuring 7.8×6.0 x 2.1 cm. On gross examination, both masses were solid-cystic with a predominant solid component (80%–90%). The cystic portion was multi-loculated and there were multiple papillary excrescences on the external surface as well as internal lining. The cystic portion contained clear serous to hemorrhagic fluid. Gross examination of the small bowel specimen showed mesenteric implants, bowel serosal deposits without evidence of mucosal or intra-luminal deposits, and negative resection margins (Figure 2). Multiple biopsies from the cul de sac, pelvic sidewall, bladder, sigmoid lesion, peri-cecal lesion as well as a portion of small bowel were examined. Microscopic examination of the ovarian masses showed features in keeping with serous borderline tumor. No micropapillary architecture or stromal invasion were noted (Figure 3). Histological changes in keeping with non-invasive implants were identified in the cul de sac, pelvic sidewall, bladder dome lesion, sigmoid mesentery lesion, and serosal surface of both fallopian tubes (Figure 4). In addition, there was endometriosis in the bladder dome lesion and right pelvic sidewall lesion. Florid reactive mesothelial hyperplasia was present in the sections of the omentum, sigmoid colon mesentery, and serosal surface of the small bowel. In some foci, extensive tissue reaction and mesothelial hyperplasia made histological assessment challenging; however, no diagnostic evidence of low-grade serous carcinoma was identified (Figure 5). Ascitic fluid cytology indicated serous low-grade neoplasm.

Gross involvement of the small bowel mesentery and bowel serosa by low malignant potential tumor.

(A) Serous borderline tumor: hierarchical, branching papillary architecture. (B) Papillary proliferation lined by cuboidal to columnar epithelium with minimal nuclear atypia.

Non-invasive implants of serous borderline tumor: glands lined by mildly atypical epithelium with no mitotic activity.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Florid reactive mesothelial hyperplasia and adhesions.
Dr Marchocki
The final pathology confirmed FIGO stage IIIC low-grade serous ovarian neoplasm consistent with low malignant potential tumor without micropapillary features arising from the right and left ovaries with non-invasive implants involving the right fallopian tubes, small bowel serosa and mesentery, sigmoid mesenteric lesion, cul de sac lesion, pelvic sidewall lesion, and bladder peritoneum lesion.
Please discuss your treatment recommendations at this point based on the final pathology. Please provide details regarding the role of chemotherapy versus hormonal therapy and the data for maintenance therapy in this setting.
Dr May
Advanced stage pre-malignant serous ovarian neoplasms that have been completely surgically resected do not require adjuvant systemic chemotherapy or radiotherapy.12 Similarly, there is no clear evidence in support of using aromatase inhibitors or other anti-hormonal therapies in the setting of non-invasive disease. Tang et al recently presented the results of a phase II study investigating the activity of anastrozole in patients with metastatic or recurrent serous low malignant potential tumors or low-grade serous carcinoma.13 While over 60% of patients experienced clinical benefit at 3 and 6 months, the results may not be applicable to most patients with advanced low malignant potential tumors as only two patients in the study cohort had a history of low malignant potential tumors, and they experienced recurrences in the form of low-grade serous carcinoma.
The overall recurrence rate for ovarian serous low malignant potential tumors quoted in the literature ranges between 3% and 10%.4 14 In patients treated with fertility sparing surgery for apparent stage I disease, the remaining ovary is the most common site of recurrence. In patients treated with radical surgery without ovarian preservation, relapses occur in peritoneal sites and present either as recurrent low malignant potential tumors or invasive carcinomas. Notably, 37% of recurrences are diagnosed within 2 years, 31% between 2 and 5 years, 22% between 5 and 10 years, and 10% after 10 years from the initial diagnosis.3 It is recognized that the longer the duration of follow-up, the higher the relapse rate.15 Silva et al found a 44% recurrence rate after a median follow-up of 15 years in 80 patients with serous low malignant neoplasms with non-invasive implants.15 In the same study, out of 33 patients with histologically proven relapse, 6 patients had serous low malignant potential tumors and 27 patients had invasive low-grade carcinoma. In a large Danish cohort of patients with serous low malignant potential tumors with a median follow-up of 10 years, 4% of patients developed malignancy of which 93% were low-grade and 7% were high-grade carcinoma.16 At our center, patients with a history of advanced serous low malignant potential tumors are seen in follow-up every 3 months in the first 2 years, every 6 months between 2 and 5 years, and annually thereafter. Clinical examination can be supplemented with CA125 levels if those were initially elevated and imaging assessment such as ultrasound.
Summary
Dr May
Serous ovarian malignancies are classified in a two-tier grading system based on their degree of nuclear atypia. Low-grade serous carcinoma corresponds to Silverberg grade 1 tumors and high-grade serous ovarian carcinoma corresponds to Silverberg grade 2–3 tumors.17 Our group compared the gene expression profiles of serous Mullerian tumors, including ovarian and fallopian tube serous carcinomas, and identified significant differential gene expression between low-grade serous carcinoma and high-grade serous carcinoma.18 Low-grade neoplasms often exhibit mutations in the mitogen-activated protein kinase (MAPK) pathway including KRAS, BRAF, and NRAS.19 Pre-invasive low-grade neoplasms–serous borderline or low malignant potential tumours–are characterized by nuclear atypia, increased cellular proliferation, and the lack of stromal invasion.20 In 2014 the WHO segregated these pre-invasive tumors into borderline serous tumors of usual variant, also known as atypical proliferative serous tumors, and borderline serous tumors of micropapillary variant, also known as non-invasive low-grade serous carcinoma.21 Invasive implants were defined as extra-ovarian low-grade serous carcinoma. We have previously studied the genomic expression of low malignant potential tumors with micropapillary features and found that they were distinct from the usual variant low malignant potential tumors and were similar to invasive low-grade serous carcinoma.22 Therefore, any low malignant potential tumor with invasive implants and any low malignant potential tumor with micropapillary features should be managed similarly to invasive low-grade serous carcinoma.
The role of systemic chemotherapy in low-grade serous carcinoma is not well established.23 The international cooperative group phase III randomized controlled trial comparing systemic chemotherapy followed by maintenance letrozole versus letrozole alone after cytoreductive surgery for stage II–IV low-grade serous carcinoma (NRG protocol GY019) will be critical to understand the role of adjuvant therapy in this disease.24 Importantly, surgery remains the cornerstone in the management of women with advanced low malignant potential tumors as well as low-grade serous carcinoma and complete cytoreduction has the highest impact on improved survival in these patients.11 Given the low response rates to chemotherapy in recurrent low-grade serous carcinoma of 2%–4%, alternative targets such as anti-hormone therapies and MEK inhibitors were studied.25 Aromatase inhibitors have been shown to be effective in the management of recurrent low-grade serous carcinoma and play an important role in the recurrent setting.13 GOG 239 examined the role of the MEK 1/2 inhibitor selumetinib in a single-arm phase II protocol in patients with recurrent low-grade serous carcinoma.26 The results showed that selumetinib was well tolerated and had a 15% response rate and 63% disease control rate in recurrent low-grade serous carcinoma. In contrast, the MILO phase III randomized trial was designed to investigate the role of the potent MEK inhibitor binimetinib compared with physician choice chemotherapy in patients with recurrent or persistent low-grade serous carcinoma.27 The study was prematurely terminated after a planned interim analysis showed that the HR for progression-free survival crossed the pre-defined futility boundary. Median progression-free survival was 9.1 months in the binimetinib arm and 10.6 months in the physician choice chemotherapy arm (HR 1.21, 95% CI 0.79 to 1.86, closed early for futility).28 The median overall survival was 25.3 months for binimetinib versus 20.8 months for physician choice chemotherapy. Interestingly, a post hoc analysis suggested a potential correlation between KRAS mutations and tumor response to binimetinib. Recently, the results of a phase II/III randomized trial were presented examining the MEK inhibitor trametinib versus physician choice standard of care systemic therapy for recurrent low-grade serous carcinoma.29 Trametinib was associated with improved progression-free survival (13.0 vs 7.2 months, HR 0.48; p<0.0001) and overall survival (37 vs 29.2 months, HR 0.75; p=0.054). Therefore, MEK-based therapy should be considered in women with recurrent low-grade serous carcinoma. Long-term studies are warranted to further stratify low-grade neoplasms by their specific MAPK mutation status to assess differential response rates within those sub-groups. Lastly, direct comparison of MEK inhibitors with aromatase inhibitors would be prudent to determine the treatment algorithm for women with recurrent disease.
References
Footnotes
Contributors Presenter: ZM. Pathologist: MR. Radiologist: TC. Discussant: TM.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Commissioned; internally peer reviewed.