Article Text

Statistics from Altmetric.com
CASE PRESENTATION
A 44-year-old G3P2 patient was transferred from a community hospital with severe abdominal pain, nausea, and hemoperitoneum requiring ongoing transfusions. She had a history of abnormal uterine bleeding for several weeks. The patient had not undergone a recent endometrial biopsy as part of the evaluation. Ulipristal acetate had been previously initiated for treatment of presumed benign degenerating leiomyomas. Past medical history was significant for two previous cesarian sections and hypothyroidism.
She was transferred to the gynecologic oncology service at our tertiary academic hospital. On physical examination, her blood pressure was 123/84, heart rate 97 beats/min, temperature 36.8°C, and oxygen saturation 98%. She had a large pelvic mass measuring approximately 22 cm, and was tender on abdominal examination due to hemoperitoneum. Pelvic examination revealed no evidence of parametrial involvement or cul-de-sac nodularity. An abdominal drain and nasogastric tube had been inserted prior to transfer for initial conservative management of hemoperitoneum and partial small bowel obstruction, respectively. On arrival, her hemoglobin was 93 g/L, prothrombin time was 13.4 s, partial thromboplastin time 26.6 s, and international normalized ratio 1.14.
Of note, for approximately 2 years prior to presentation to our service, the patient had been undergoing serial pelvic ultrasound examinations for monitoring of presumed benign leiomyomas. Ultrasound had revealed a partially calcified and necrotic fibroid uterus measuring 12 to 14 cm, with the largest fibroid measuring 5 cm. Two months prior to this presentation, an abdominal CT had revealed a multifibroid uterus measuring 15×11 x 9 cm. The presumed fibroids were described as homogeneous and solid, with cystic changes. A 13×13 x 9 cm complex cystic lesion with thick walls abutting the uterus was identified, separate from the ovaries. This had significantly increased in size compared with previous ultrasounds.
Dr Ghandehari
CT scan imaging (Figure 1A&B) performed prior to transfer to our institution showed enlargement of the uterus with multiple complex cystic areas due to necrosis and cystic degeneration, new free fluid, and dilatation of small bowel loops consistent with partial small bowel obstruction secondary to mass effect from the enlarged uterus. There was no evidence of metastatic spread. Five days prior to surgery, an MRI revealed a uterine size of 25×13 x 12 cm, and radiological features suspicious for leiomyosarcoma with evidence of rupture and large volume hemoperitoneum (Figure 2A–D). Chest X-ray examination did not show evidence of metastasis.
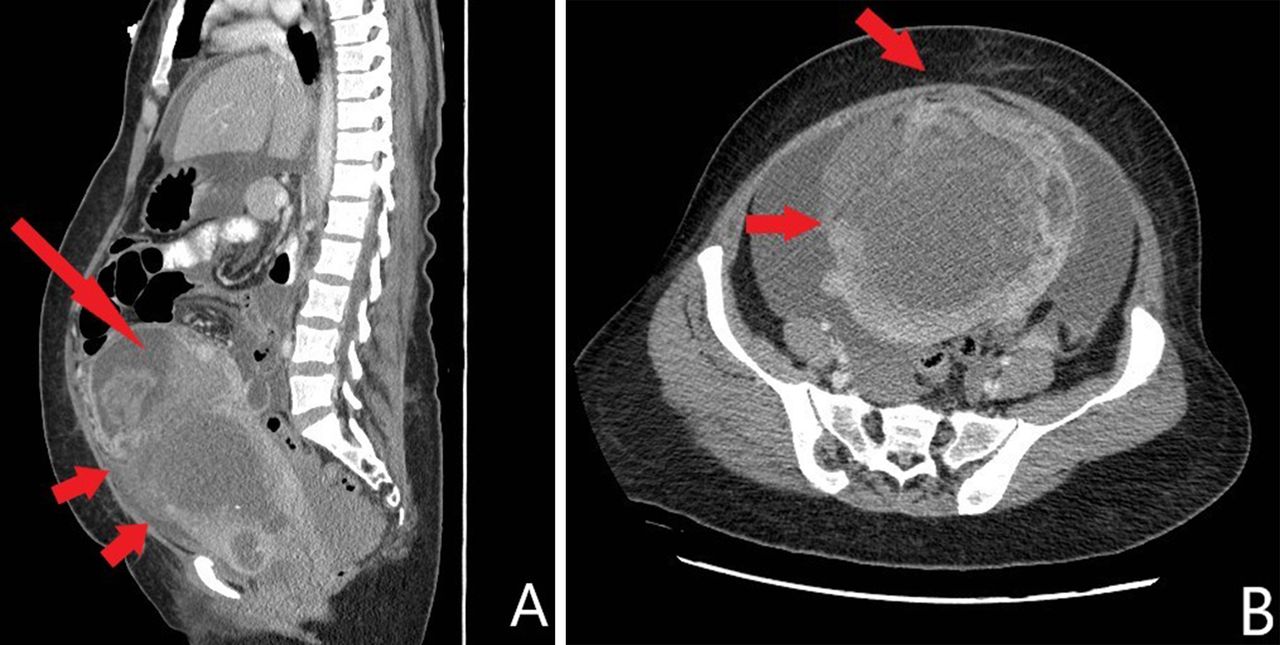
(A, B) CT abdomen pelvis 6 days prior to surgery: the fundal cystic/necrotic component appears partially collapsed and contains dense material (blood: long arrow). There is an apparent 'gap' in the anterior aspect (between two small arrows) with adjacent clot. Interval significant increase in free fluid which is dense in the dependent pelvis (hemoperitoneum).

(A-D) MRI pelvis 5 days prior to surgery: post-contrast fat saturation (A and B), axial T2 (C), axial T1 post-contrast fat saturation (D).
Dr Vicus
Based on this history and imaging evaluation, what should be the differential diagnosis and the proposed plan of management?
The differential diagnosis included degenerated benign leiomyoma versus uterine leiomyosarcoma. Her clinical presentation and imaging were reviewed at our multidisciplinary case conference. Although there are over 100 reported cases of hemoperitoneum secondary to spontaneous rupture of uterine leiomyomas and/or their overlying vessels,1 presumptive diagnosis of leiomyosarcoma was made in view of a notable increase in size in comparison with previous imaging studies, irregular and ill-defined margins, heterogeneous signal intensity on both T1- and T2-weighted images, and central hyperintensity on T2-weighted images suggestive of extensive necrosis. Surgery should be the cornerstone of management for diagnosis and treatment, as there was no evidence of metastatic disease, and the patient was very symptomatic. As such, decision was made to recommend surgery with total abdominal hysterectomy, bilateral salpingo-oophorectomy, and possible cytoreduction if metastatic spread was found at the time of surgery. It was proposed to proceed with uterine artery embolization prior to surgery to decrease risk of severe intra-operative bleeding in the setting of the large uterine tumor.
She continued to be treated conservatively for partial small bowel obstruction. She underwent surgery 24 hours after embolization. A midline laparotomy was performed the day after transfer to our institution. On entry into the abdominal cavity, an area of full-thickness uterine rupture was identified, and approximately 1500 mL of blood was evacuated. The proximal ileum and omentum were adherent to the anterior wall of the 20-week size uterus. We performed a total abdominal hysterectomy, bilateral salpingo-oophorectomy, small bowel resection (approximately 20 cm of ileum removed) with re-anastomosis, and omentectomy. The specimen was not sent for frozen section, as frozen section analysis is not routinely performed in our institution for uterine tumors. The abdominal cavity was examined thoroughly and there were no sites of metastasis. Surgical duration was 164 min, and intra-operative blood loss was 300 mL. The patient did not require any intra-operative transfusions. Post-operatively her hemoglobin was 74 g/L and she received 1 unit of packed red blood cells for symptomatic anemia. Her post-operative course was otherwise unremarkable. She was discharged home in stable condition on post-operative day 3. She was seen at her post-operative appointment 4 weeks later and had recuperated well.
Dr Parra-Herran
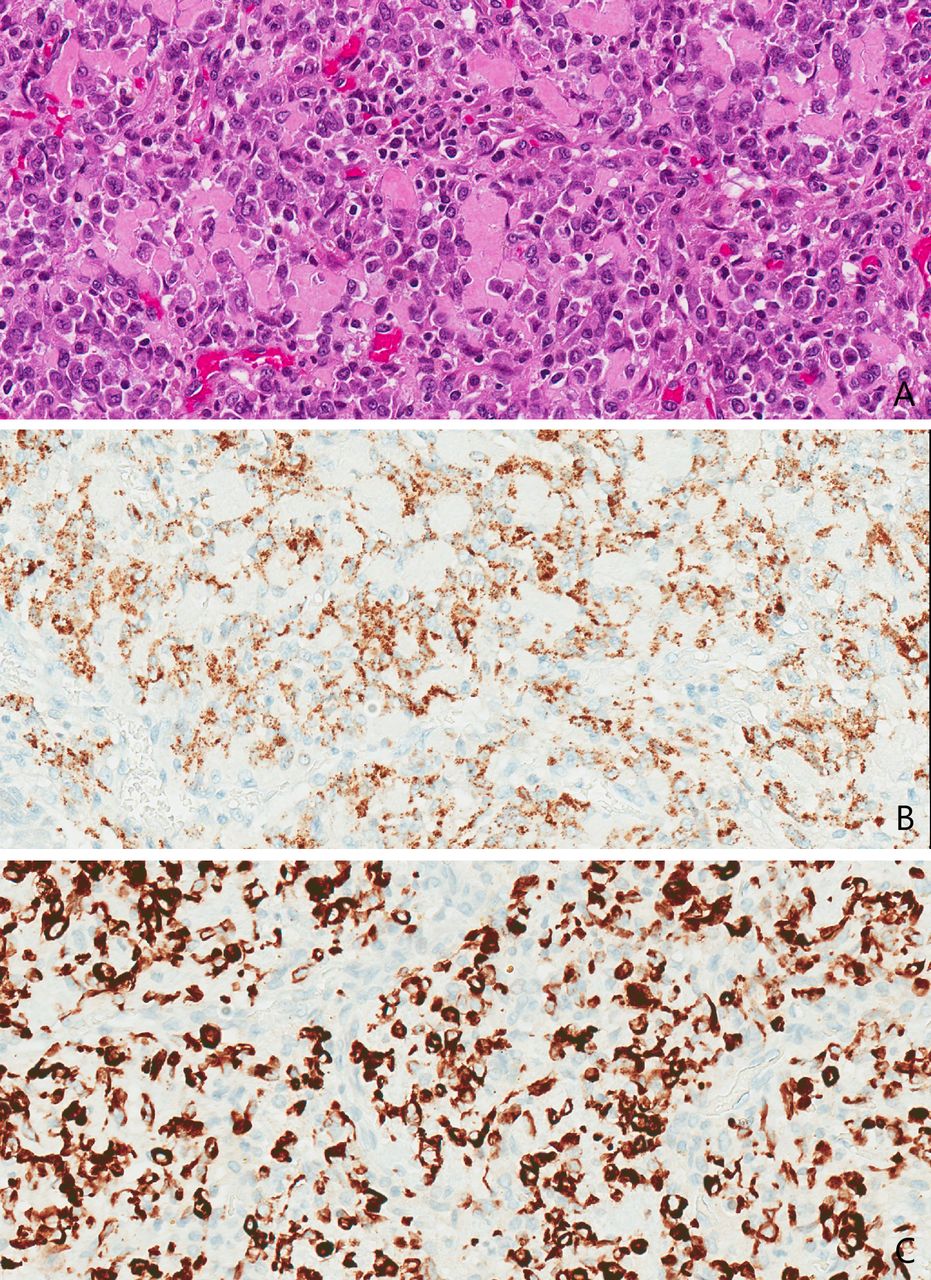
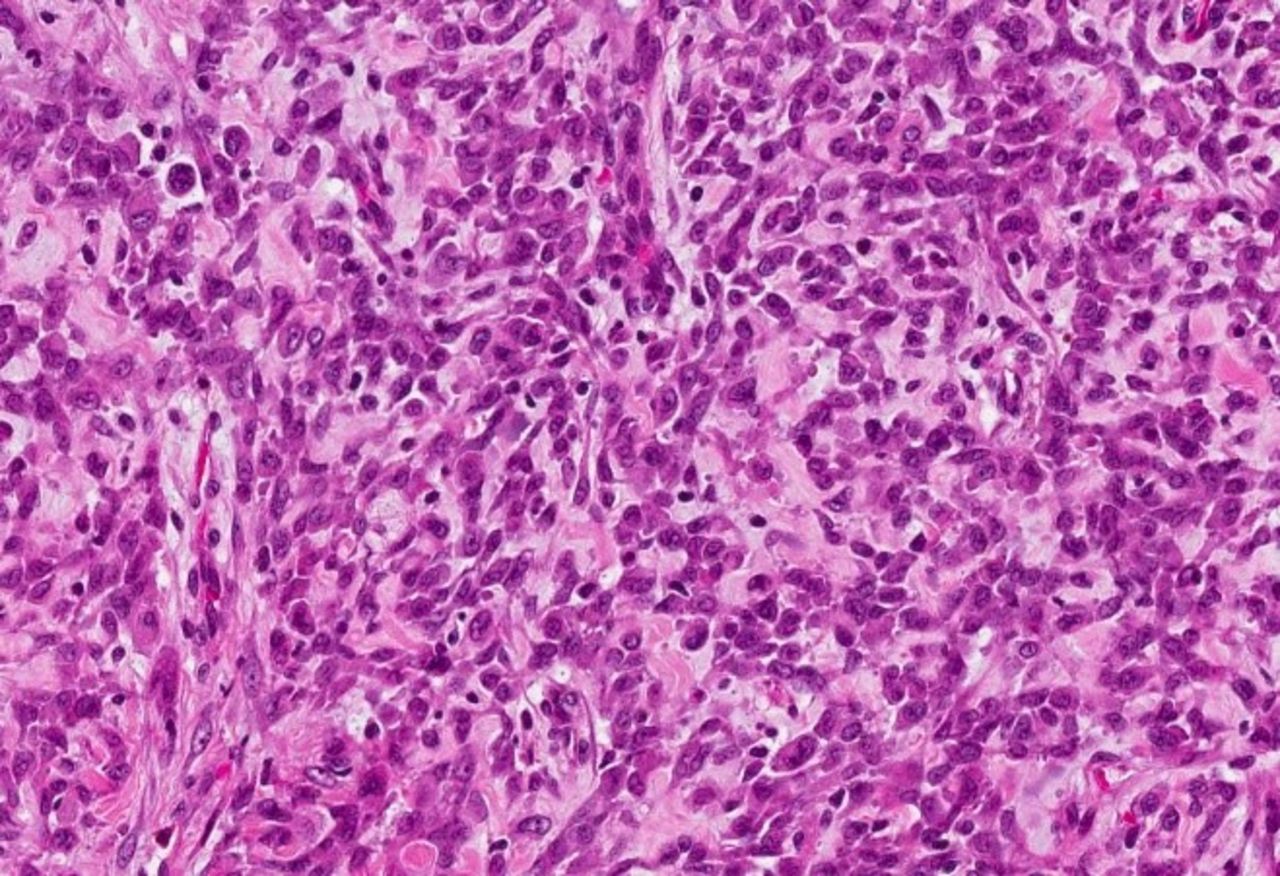
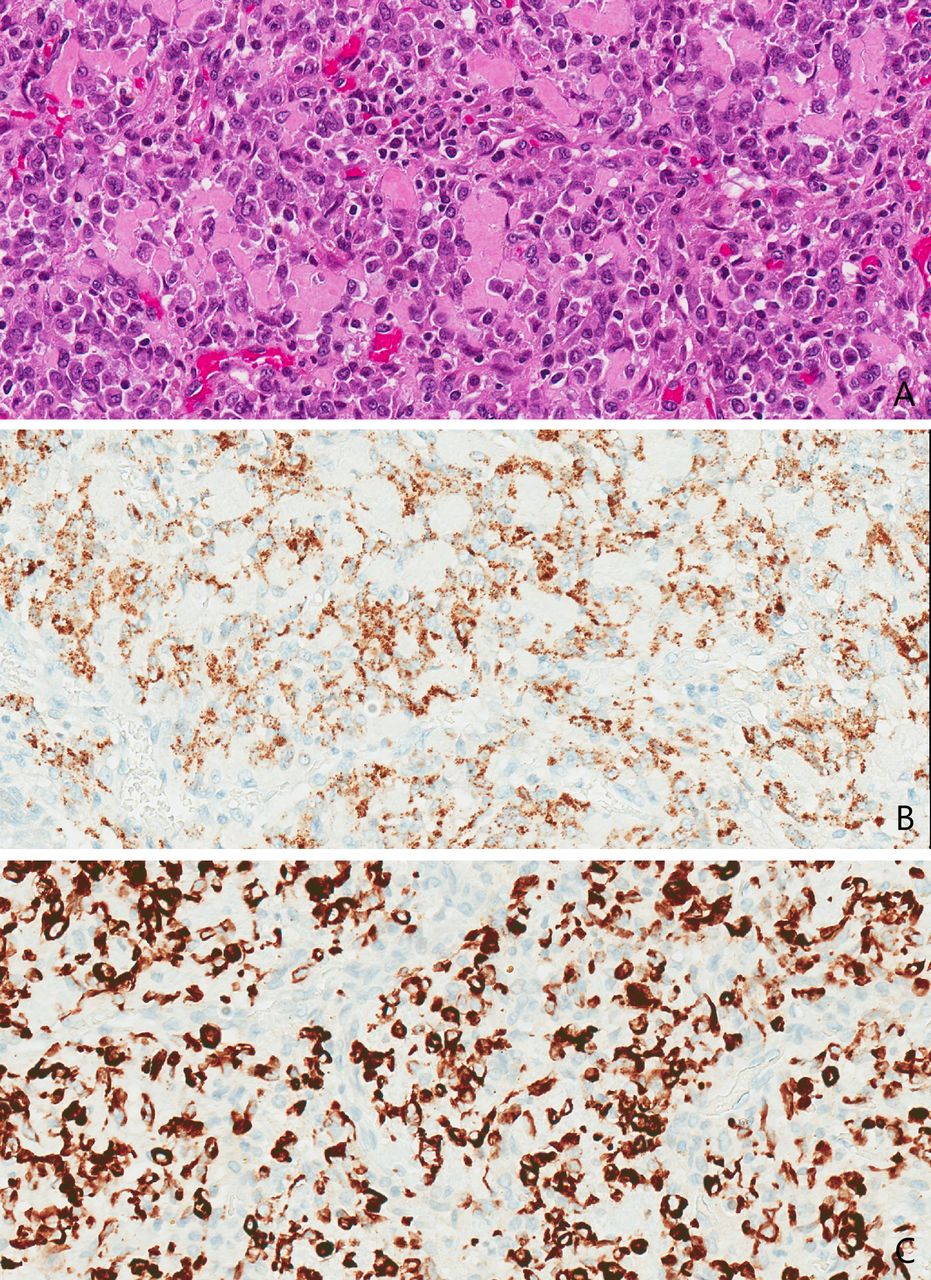
The tumor cells had an epithelioid and spindled morphology, with low-grade nuclear atypia and dense eosinophilic cytoplasm (Figures 3 and 4). The mitotic activity was less than 1 per 50 high power fields and there was no lymphovascular space invasion. However, the tumor was large (18 cm) and associated with vast infiltration into the myometrium. Tumor nodules were present on the uterine serosal surface with direct invasion into the muscularis propria of the small bowel. Tumor necrosis was present. All resection margins were negative for malignancy. By immunohistochemistry (Figure 5A–C), the cells stained strong and diffuse for desmin, smooth muscle actin and HMB-45, with 50% estrogen receptor positivity. There was focal patchy staining for caldesmon, CK7, and CD10. Stains for pankeratin, epithelial membrane antigen, myogenin, S100, S0×10, melan-A, and cyclin-D1 were negative. Given the above characteristics, the final pathology diagnosis was uterine perivascular epithelioid cell tumor (PEComa). It was classified as malignant based on the large tumor size, presence of necrosis, and extra-uterine spread.

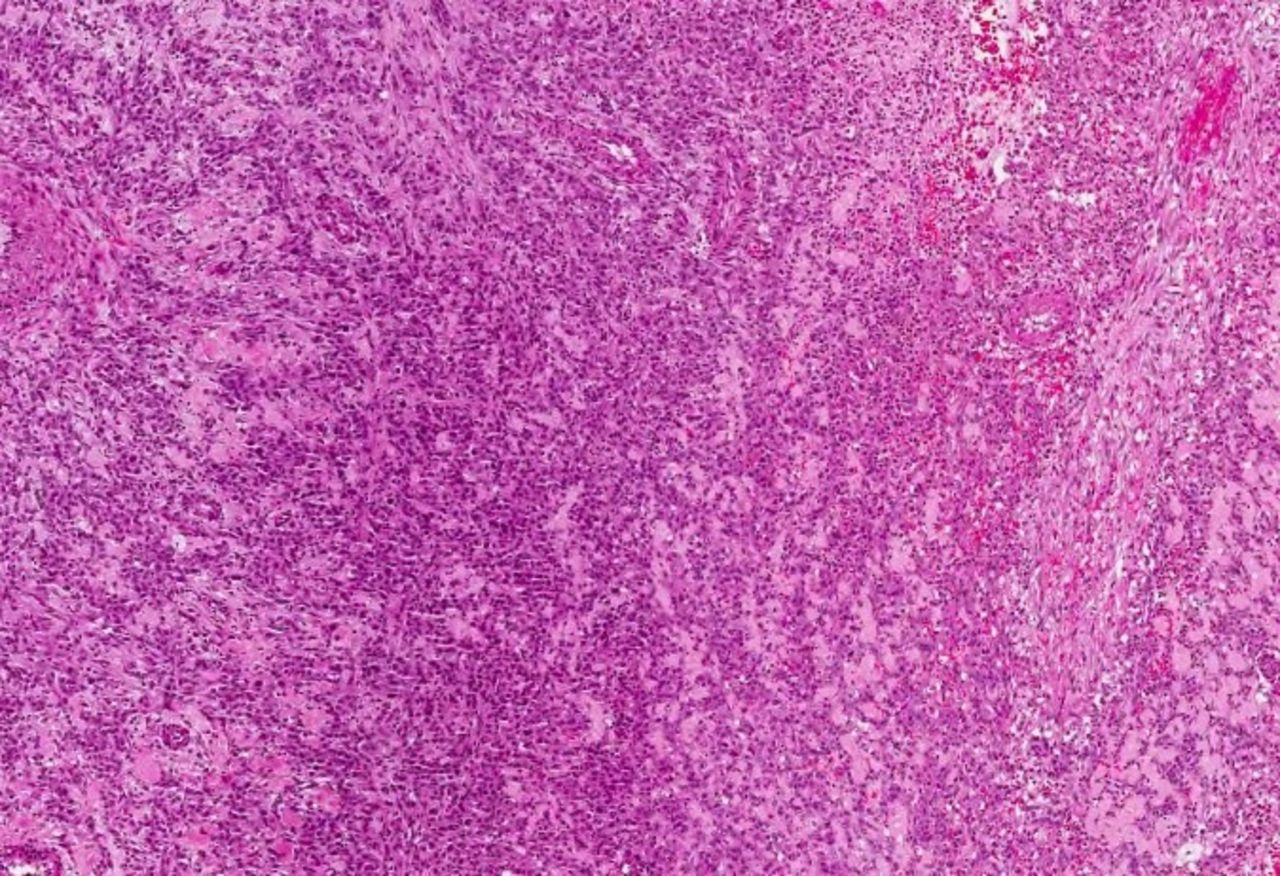
Perivascular epithelioid tumor. The neoplasm has solid growth (left aspect) with areas of hemorrhage and necrosis (right aspect).

The tumor is composed of round to polygonal ('epithelioid') cells with eosinophilic cytoplasm.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A-C) Immunohistochemistry: epithelioid cells with granular cytoplasm (A), show strong expression of HMB-45 (B) and desmin (C).
Dr Vicus
Given the findings on final pathology, what would be your recommended approach for ongoing management of this patient?
The final pathology, imaging, and clinical case were again presented at our multidisciplinary case conference, and decision was made for observation with serial imaging and physical examination. Due to the extreme rarity of uterine PEComas, there are no published guidelines or consensus to guide management. Complete surgical resection with the goal of obtaining negative margins is the cornerstone of treatment—namely, total hysterectomy, with or without bilateral salpingo-oophorectomy. There are no data to support the use of adjuvant treatment. This patient had complete resection with no residual tumor at the end of surgery. She will require long term follow-up for more than 5 years, as there are reports of late recurrence. Indeed, PEComas can recur both locally and distantly, commonly with pulmonary metastases. Late pulmonary, renal, and cardiac recurrences have been reported over 5 years after initial diagnosis.2
A baseline postoperative CT scan was ordered 4 weeks after surgery to rule out metastatic disease. This revealed a 1.2×1.7 cm retroperitoneal lymph node, and decision was made to follow up conservatively with repeat imaging, which would help to determine whether this was reactive following surgery, or metastatic disease. A CT scan was repeated 2 months later and showed decrease in adenopathy to 0.9×1.3 cm. Four months later, the adenopathy had decreased to 0.8 cm on repeat CT scan. There were no lesions on CT chest imaging. The patient was recently re-assessed 13 months after surgery and was well and without evidence of recurrence. She will be re-assessed at 4-month intervals with repeat imaging.
CLOSING SUMMARY
Uterine perivascular epithelioid cell tumors (PEComas) are very rare mesenchymal neoplasms with fewer than 100 cases reported in small case series and case reports in the literature.3 4 They are composed of clear to eosinophilic epithelioid cells with a perivascular growth pattern, which exhibit distinctive immunohistochemical expression of both melanocytic (HMB-45, melan-A, MiTF) and smooth muscle markers (smooth muscle actin, desmin, caldesmon).
The World Health Organization defines PEComa as a “mesenchymal tumor composed of histologically and immunohistochemically distinctive perivascular epithelioid cells”. PEComas include renal angiomyolipomas, lymphangioleiomyomatosis, clear cell sugar tumor of the lung, and PEComas of the retroperitoneum, liver, kidney, pancreas, and uterus.5 PEComas of gynecological origin account for approximately a quarter of PEComas reported in the literature. Most gynecologic PEComas arise in the uterine corpus, with the cervix less commonly involved.4 The largest systematic review of uterine PEComas comprises 65 patients between the ages of 9 and 79 years.4 Most patients are diagnosed in their 40s and present with abnormal uterine bleeding, abdominal pain, and/or abdominal mass. Approximately a tenth of cases are associated with tuberous sclerosis,3 an autosomal dominant syndrome characterized by renal angiomyolipomas, lymphangioleiomyomatosis, cardiac rhabdomyomas, and subependymal giant cell astrocytomas.
Uterine PEComas represent a diagnostic challenge due to their non-specific clinical and radiological findings, often resulting in a delay in definitive treatment.6 In most cases reported in the literature, the diagnosis is only made post-operatively. Radiologically, findings in uterine PEComas are non-specific and variable, and they can mimic other benign or malignant entities: it is nearly impossible to make a pre-operative diagnosis based on imaging. They can appear homogeneous and resemble regular leiomyomas, or show heterogeneity and contour irregularity suspicious for degenerated leiomyomas or leiomyosarcomas. They are often well-circumscribed.5 Imaging features may not help discern benign from malignant PEComas. Enhancement on imaging is variable, with most PEComas showing significant intensity and enhancement on CT and MRI T2-weighted images,5 with calcification, necrosis, or hemorrhage described in a minority of cases. Ultrasound findings include heterogeneous echotexture without significant vascularity or cystic areas.
There is heterogeneity in malignant behavior and a wide morphologic spectrum: PEComas can be benign, of uncertain malignant potential, or malignant. Several criteria have been proposed to distinguish between benign and malignant PEComas; however, given the rarity of this disease, such proposals still require validation,7 8 A combination of the following features can indicate greater malignant potential: tumor size greater than 5 cm, necrosis, lymphovascular invasion, infiltrative growth pattern, high-grade atypia, and a mitotic rate greater than 1 per 50 high power fields.3 PEComas typically stain positive for HMB-45 and cathepsin-K; other markers frequently positive include smooth muscle actin, desmin, caldesmon melan-A and MiTF.7
The cornerstone of treatment is complete resection with negative margins. In a review of 65 cases,4 most patients were treated with total hysterectomy, with or without bilateral salpingo-oophorectomy, and only one patient was treated with fertility-sparing surgery, followed by adjuvant temsirolimus.9 Another case study of a young patient treated with fertility-sparing surgery reported no evidence of recurrence at 6 years of follow-up.10 As this entity is so rare, there are no prospective trials that elucidate the question of adjuvant management. Small case series describe the use of adjuvant therapy for high-risk disease, with heterogeneous treatment regimens including dacarbazine, ifosfamide, carpoblatin, epirubicin, doxorubicin, and vincristine. For patients who develop recurrences, the optimal strategy is debated. For patients with oligometastasis, surgery is an option. Recent reports also suggest activity of mammalian target of rapamycin (mTOR) inhibitors, including temsirolimus and everolimus, in certain types of PEComa (those with mutations in TSC1 or TSC2) with advanced and recurrent disease.2 11 12 Recent immunohistochemical analyses demonstrate TSC1 and TSC2 inactivation and up-regulation of the mTOR pathway in certain PEComas.4 The optimal treatment regimen is unknown. The role of radiation therapy is debated and its benefits on loco-regional relapse remain controversial.
In conclusion, uterine PEComas are an exceedingly rare entity with distinctive histologic and immunohistochemical features, although with non-specific clinical and radiologic presentation, making a pre-operative diagnosis challenging. There is a spectrum of pathobiological variation and clinical outcomes. Due to the paucity of cases, it is difficult to conduct randomized trials to elucidate the role of adjuvant treatment, and to establish the best strategies for advanced and recurrent disease. The addition of adjuvant treatment should be considered in patients presenting with advanced disease. mTOR inhibitors are a promising avenue that will require more investigation. Patients with uterine PEComas require close and prolonged follow-up due to reports of late recurrences.
Supplemental material
Footnotes
Contributors DV identified the patient, DV and JMVN managed treatment of the patient and drafted the manuscript, HG provided radiology images and reviewed the radiology component of the paper, CP-H provided pathology slides and reviewed the pathology component of the paper.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Commissioned; externally peer reviewed.