Article Text

Abstract
Objective The CIRCE trial (NCT 01973101) investigated the efficacy, safety, and quality of life of the addition of neoadjuvant chemotherapy with cisplatin and gemcitabine to standard chemoradiation for locally advanced cervical cancer (stages IIB–IVA). The impact of both treatment arms on quality of life is reported in the present study.
Methods Patients completed the European Organization of Research and Treatment of Cancer questionnaire QLQ-C30 and CX24 before treatment and at 3, 6, 9, and 12 months after treatment. Linear mixed models were fitted to analyze differences in quality of life over time and between groups. Differences in mean quality of life scales >10 points and p<0.05 were considered clinically relevant and statistically significant, respectively. Inclusion criteria were: (1) histological diagnosis of locally advanced invasive carcinoma of the uterine cervix, International Federation of Gynecology and Obstetrics stages IIB–IVA; (2) signed informed consent to participate in the CIRCE trial; and (3) answered at least one quality of life questionnaire. Excluded were patients who did not complete any quality of life questionnaire. Relevant exclusion criteria for the CIRCE trial included Eastern Cooperative Oncology Group performance status >2 and peripheral neuropathy >2. Mann–Whitney U tests were performed to assess differences between groups in quality of life at baseline. To evaluate differences between treatment arms, linear mixed models were fitted using the transformed quality of life scores as a dependent variable and time of follow-up and study arm as factors.
Results A total of 107 patients were enrolled (n=55 neoadjuvant chemotherapy arm; n=52 chemoradiation arm). Quality of life compliance rates were higher for the chemoradiation group at every assessment time (ranging from 75–86.5% in the chemoradiation arm vs 55–81.8% in the neoadjuvant chemotherapy arm). For quality of life results at baseline, no statistically significant difference between the groups was seen. For both groups, most scales showed improvements over time, except for worsening of the summary score, sexual enjoyment, peripheral neuropathy, and menopausal symptoms. For chemoradiation, body image was lower (p<0.001) and patients presented more lymphedema (p<0.001) and sexual worry (p<0.001) at 12 months compared with baseline. Comparing study arms, neoadjuvant chemotherapy showed significantly lower scores in the menopausal symptoms scale (p=0.03) and higher scores for sexual/vaginal functioning (p=0.01). At 12 months, clinical differences were seen only for body image and menopausal symptoms scale, with neoadjuvant chemotherapy presenting better body image scores and a lower burden of menopausal symptoms.
Conclusion After treatment for locally advanced cervical cancer, patients improved in most quality of life aspects. However, worsening was observed in sexual enjoyment, peripheral neuropathy, and menopausal symptoms. To improve patients’ quality of life, efforts should be made to prevent and treat these long term effects of locally advanced cervical cancer treatment.
- quality of life (PRO)/palliative care
- uterine cervical neoplasms
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, an indication of whether changes were made, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
HIGHLIGHTS
Patients with locally advanced cervical cancer undergoing neoadjuvant chemotherapy with cisplatin and gemcitabine plus chemoradiation had a similar quality of life compared with those undergoing standard chemoradiation
For both groups, most scales showed improvements over time, except for worsening of the summary score, sexual enjoyment, peripheral neuropathy, and menopausal symptoms.
At 12 months, clinical differences were seen only for body image and menopausal symptoms scale,
Introduction
Cervical cancer is the third most common malignancy among women in Brazil1 ¹ and the fourth worldwide.2 Naga et al reported that more than two-thirds of patients have advanced disease at diagnosis and approximately 85% occur in developing countries.3 For locally advanced cervical cancer (International Federation of Gynecology and Obstetrics (FIGO) stages IIB–IVA), chemoradiation with platinum agents has been he standard treatment for almost two decades, with evidence of its superiority compared with radiotherapy alone.4–8 However, 25–40% of patients still experience disease recurrence after chemoradiation.9 In addition, early and late treatment toxicities of chemoradiation may also impair these patients’ quality of life.
Several options have been investigated to improve clinical outcomes of locally advanced cervical cancer.10–13 Gemcitabine, for example, is known to synergize with radiation and cisplatin.14 In a phase III trial, the use of cisplatin and gemcitabine concurrent with radiotherapy and after chemoradiation was associated with superior progression free and overall survival.10 However, grade 3 and 4 toxicities were significantly higher with the addition of gemcitabine to concurrent cisplatin chemoradiotherapy and adjuvant chemotherapy with cisplatin, compared with standard treatment (86.5% grade 3 and 4 toxicities, vs 46.3%), which limited the use of this strategy in clinical practice. The addition of gemcitabine to standard cisplatin regimens has been evaluated in the neoadjuvant setting. Neoadjuvant chemotherapy with gemcitabine and cisplatin was tested before surgical treatment in two phase II studies, with favorable outcome in response rate.11 12 Further analysis from non-randomized phase II trials suggested that neoadjuvant chemotherapy followed by surgery or chemoradiation was at least as effective as standard concurrent cisplatin based chemoradiation.13
The CIRCE trial is a phase II trial that aimed to evaluate the efficacy and safety of the addition of neoadjuvant chemotherapy with cisplatin and gemcitabine to standard chemoradiation for locally advanced cervical cancer (NCT 01973101).15 The neoadjuvant chemotherapy group was associated with decreased 3 year progression free survival, with 3 year progression free survival rates of 40.9% compared with 60.4% in the chemoradiation arm (hazard ratio (HR) 1.84 (95% confidence interval (CI) 1.04 to 3.26); p=0.03), lower overall survival (3 year overall survival 60.7% vs 86.8%; HR 2.79 (95% CI 1.29 to 6.01); p=0.006), and lower complete response rates (56.3% vs 80.3%; p=0.008).15 Toxicities were similar between arms, except for a higher frequency of hypomagnesemia and neuropathy in the neoadjuvant chemotherapy arm. The study concluded that the addition of neoadjuvant chemotherapy to chemoradiation is not superior and is possibly inferior to chemoradiation alone in the treatment of locally advanced cervical cancer.
A systematic review in patients with cervical cancer, post treatment, undergoing surgery, chemotherapy, radiotherapy, or a combination, reported that quality of life was compromised compared with the general population, mainly in terms of sexual functioning. Further, treatment with radiotherapy was reported to have a greater negative impact on quality of life.16 Additionally, previous studies that analyzed the addition of neoadjuvant chemotherapy to chemoradiation did not analyze quality of life, leading to a paucity of data in the literature on patient reported outcomes with this treatment modality.17 18 As quality of life has emerged as an important oncological endpoint in clinical trials, helping in decision making, the present study reports the quality of life results with the two treatment strategies, which was a secondary endpoint of the CIRCE trial. We hypothesized that quality of life would be similar in both groups at the 12 month follow-up.
Methods
Study Design
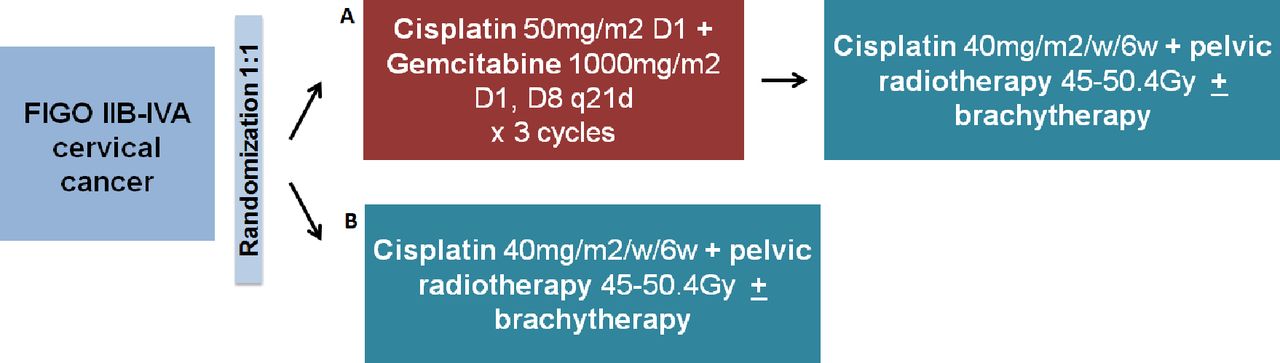
This study was conducted as a secondary analysis of the CIRCE trial to evaluate quality of life outcomes (NCT 01973101).15 The CIRCE trial is a randomized, phase II trial, assessing the efficacy and safety of neoadjuvant chemotherapy with cisplatin and gemcitabine followed by chemoradiation with cisplatin for patients with locally advanced cervical cancer. Patients were allocated, by a simple 1:1 randomization using a computer generated random list, to three cycles of neoadjuvant chemotherapy with cisplatin and gemcitabine followed by standard chemoradiation followed by brachytherapy or standard chemoradiation and brachytherapy alone (Figure 1). The primary endpoint was 3 year progression free survival and the secondary endpoints were complete response rate, overall survival, toxicity, and quality of life.15
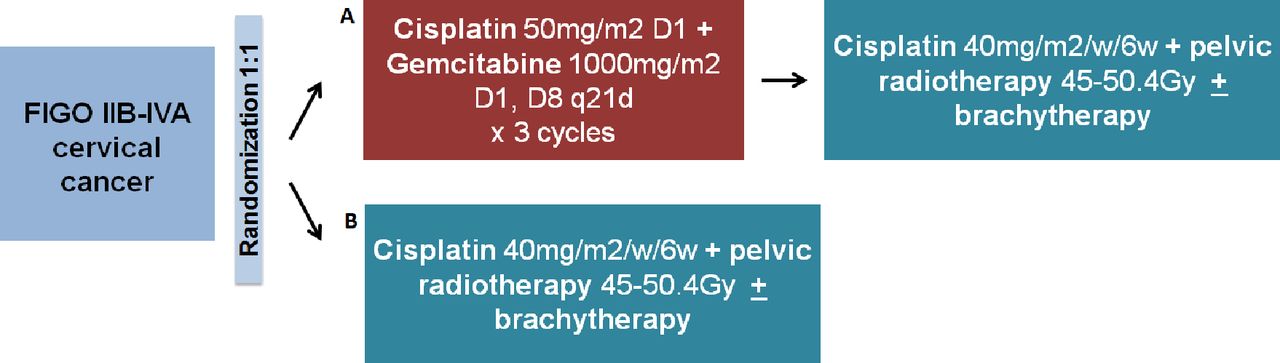
Study design and treatment modalities for each study arm.
Quality of life questionnaires were applied at baseline and after completion of treatment at 3, 6, 9, and 12 months. The baseline assessment was performed following diagnosis but prior to treatment initiation and prior to the medical consultation. The ethics committee of the participating institution approved the study.
Patients
Eligibility was assessed for patients admitted to the Instituto do Cancer do Estado de Sao Paulo and participating in the CIRCE trial. Inclusion criteria were: (1) histological diagnosis of locally advanced invasive carcinoma of the uterine cervix, FIGO stages IIB–IVA; (2) signed informed consent to participate in the CIRCE trial; and (3) answered at least one quality of life questionnaire. Excluded were patients who did not complete any quality of life questionnaire. Relevant exclusion criteria for the CIRCE trial included Eastern Cooperative Oncology Group performance status >2 and peripheral neuropathy >2. Additional eligibility criteria for the CIRCE trial are described elsewhere.15 All patients provided written informed consent before randomization.
Quality of Life Assessment
The quality of life assessment was performed using the European Organization of Research and Treatment of Cancer (EORTC) questionnaire core module, QLQ-C30,19 and its cervical cancer module, QLQ-CX24, both validated tools.20 The general cancer module includes one global health status, five functional scales, three symptom scales, and six single items, generating a total of 15 scales. Additionally, a summary score was introduced by the EORTC in 2016.21 The summary score is calculated from the mean of 13 of 15 QLQ-C30 scales (global health status and financial difficulties are excluded).22 The QLQ-CX24 includes four functional scales and five symptom scales. From the functional scales, two scales are intended only for a subset of patients who are sexually active. Higher scores in the functional scales and global health status indicate better functioning whereas higher scores in the symptom scales indicate higher symptoms burden.23 Patients received the questionnaire prior to the medical consultation and were instructed by a health professional to answer it according to what they felt, and that there were no right or wrong answers. The professionals, all nurses, were trained in the institution for this purpose. For illiterate patients, the patient’s companion read the questionnaire. If this was not possible, the health professional present was advised to do it. The questionnaires were translated into Portuguese and culturally validated in our population.20 24 25
Statistical Analysis
Descriptive statistics were used to describe patients’ clinical characteristics as well as quality of life data. Sample size was calculated based on the primary outcome of the CIRCE trial (progression free survival) and is described elsewhere.15 Questionnaire completion rates were calculated for all patients per assessment time and per treatment arm. The completion rate was derived from the number of responders for a time point by the number of expected responders (intention to treat population). All EORTC scales were linearly transformed to a continuous scale (0–100). For this analysis, differences in the mean quality of life scales >10 points were considered clinically relevant, as proposed by Osoba et al.26 Missing items were handled following the EORTC scoring manual.23 For missing scales, imputation was performed using the mean of the nearby observation only when both nearby observations were available. Baseline scores were not imputed, and neither were scores of patients who dropped out of the study or who were lost to follow-up. As all quality of life scales had a skewed distribution, the scores were transformed using a logarithmic transformation.
Mann–Whitney U tests were performed to assess differences between groups in quality of life at baseline. To evaluate differences between treatment arms, linear mixed models were fitted using the transformed quality of life scores as a dependent variable and time of follow-up and study arm as factors. Time of follow-up was entered as a repeated measure and study arm as a fixed effect. Further, to analyze differences within each group over time, the study arms were analyzed separately, fitting a linear model for each group with transformed quality of life scores as dependent variables and time of follow-up as an effect. In addition, graphs were constructed in which the mean values over time on the subscales of the quality of life questionnaire were presented. As the distribution of the data was skewed, no confidence intervals were constructed.
Results
Population Characteristics
Between July 2012 and July 2017, 107 patients were enrolled and randomized. All patients in the clinical trial were included in this analysis. Clinical characteristics are described in Table 1. In the neoadjuvant chemotherapy group, median age was 48 years (interquartile range (IQR) 40–58), 87.2% had squamous cell carcinoma, and most patients had stage IIIB disease (47.2%). For the chemoradiation group, median age was 45 years (IQR 38–54), 88.4% had squamous cell histology, and 42.3% had stage IIIB disease. Patient compliance with radiotherapy was similar in the two groups. However, more patients discontinued concurrent chemotherapy in the neoadjuvant chemotherapy arm (80%) than in the chemoradiation arm (94.2%). The main reasons for discontinuing chemotherapy were toxicities (n=9) and withdrawal of consent (n=5).
Population clinical characteristics
Quality of Life Compliance
Quality of life compliance was reported by each study arm at every time point in the study (Figure 2). Quality of life compliance rates were higher for the chemoradiation arm in every assessment. Considering the intention to treat population, at 12 months, 69.2% (36/52) of patients in the chemoradiation group answered the questionnaires, while in the neoadjuvant chemotherapy group, only 40% (22/55) had responded. Recurrence was higher for the neoadjuvant chemotherapy group during follow-up time (11 patients in the neoadjuvant chemotherapy group and 7 in the chemoradiation group), and patients who had recurrence were discontinued from the quality of life assessment. Among patients who continued in the trial at 12 months (no recurrence, death, or withdrawal of consent), compliance was 55.5% (22/40) in the neoadjuvant chemotherapy arm and 81.8% (36/44) in the chemoradiation arm.

Flowchart of compliance with quality of life questionnaires. The number of responders at each time assessment is presented as well as compliance rates, in parentheses.
Quality of Life Measures
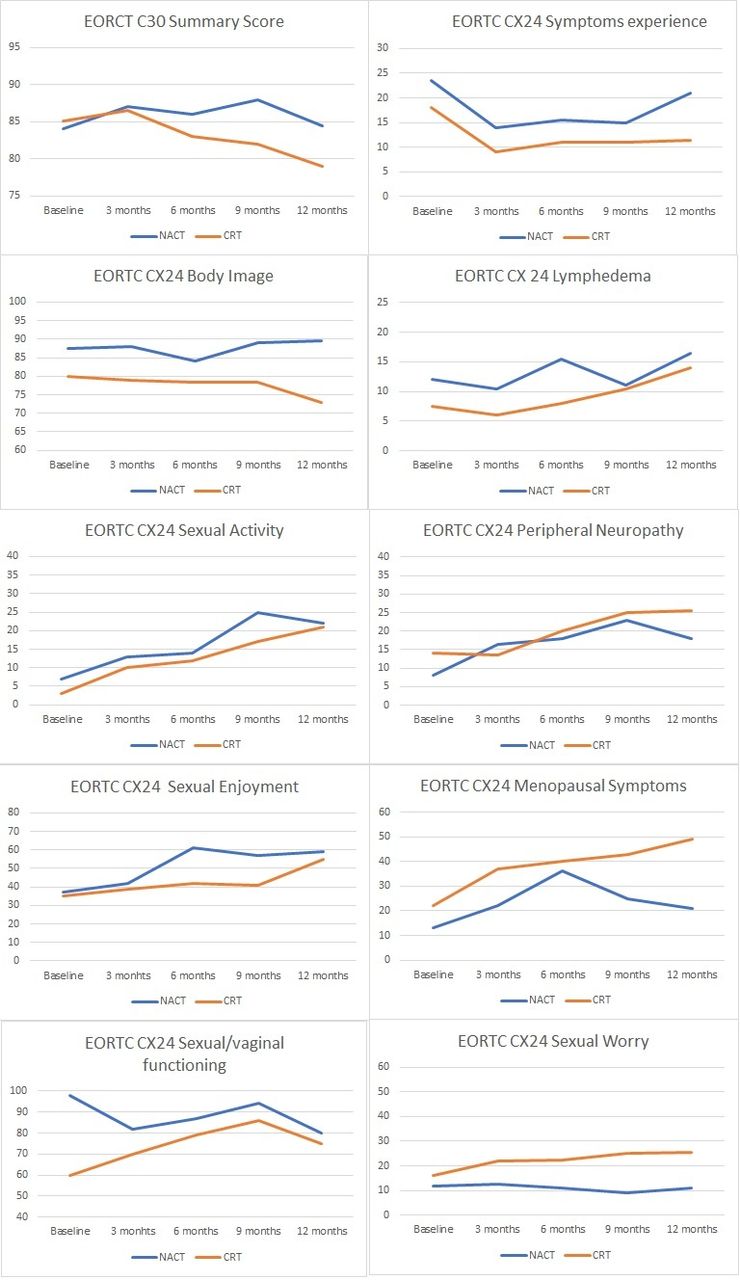
Median (IQR) quality of life scales are presented by treatment arm and assessment time in Table 2. At baseline, there were no statistically significant differences regarding quality of life between the groups. Both groups demonstrated statistically significant differences in quality of life scales over time, except for global health scale. In the neoadjuvant chemotherapy group, the sexual worry scale did not significantly change over time. For both groups, most scales showed improvements over time, except for worsening in the summary score, peripheral neuropathy, and menopausal symptoms scales (Figure 3). Additionally, in the chemoradiation arm, body image was lower compared with baseline, and patients presented more lymphedema and sexual worry at the 12 month follow-up compared with baseline. Comparing study arms, patients in the neoadjuvant chemotherapy group had statistically significant lower scores in the menopausal symptoms scale, indicating lower burden of menopausal symptoms, and higher scores in sexual/vaginal functioning, demonstrating better sexual functioning. For the other scales, no statistically significant differences between the study arms were seen after 1 year. At 12 months, clinical differences were seen only for body image, sexual activity, and menopausal symptoms scale, with patients undergoing neoadjuvant chemotherapy demonstrating better body image and sexual activity scores and lower burden of menopausal symptoms. To further understand why these differences between the groups occurred, exploratory analyses were performed to access the factors that could be associated. Among patients who completed the 12 month follow-up, patients in the neoadjuvant chemotherapy group were significantly younger than those in the chemoradiation group (median age in the neoadjuvant chemotherapy group 52.3 years vs 53.7 years in the chemoradiation group; p<0.001).
{kind=link}
{kind=link}
{kind=link}
Quality of life scales over time of follow-up. Mean scores are represented by group at each time point. CRT, chemoradiation; EORTC European Organization for Research and Treatment of Cancer; NACT, neoadjuvant chemotherapy.
Quality of life outcome over time; scores for functional scales, in which higher scores represent better functioning, and symptoms scales, with higher scores representing higher burden of symptoms. As all quality of life scales had a skewed distribution, the scores were transformed using logarithmic transformation
Discussion
The CIRCE trial showed that women with locally advanced cervical cancer treated with neoadjuvant chemotherapy with cisplatin and gemcitabine followed by standard chemoradiation had a similar quality of life compared with patients treated with standard chemoradiation. Both groups demonstrated improvements over time in most quality of life aspects, except for worsening in peripheral neuropathy and menopausal symptoms, observed in both groups. Comparing our baseline quality of life data, both groups had similar results to other studies using the same measurement tools and with similar populations, indicating that our cervical cancer population is representative regarding their quality of life.20 27 28 Sexual quality of life was the main impairment, especially for the chemoradiation group.
Regarding changes in quality of life scales over time, both groups showed improvements in sexual activity, sexual enjoyment, and symptoms experience scales. These findings are in line with prospective studies analyzing post treatment quality of life.27–29 Further, for both groups, results were worse at 12 months compared with baseline for the summary score, peripheral neuropathy, and menopausal symptoms. Additionally, similar to a prospective, longitudinal study evaluating quality of life and distress in early and locally advanced cervical cancer, menopausal symptoms were one of the most disabling treatment related sequelae.28 Further, in a population based survey investigating quality of life in cervical cancer survivors, women treated with radiotherapy reported more peripheral neuropathy than others.30
Menopausal symptoms were found to have considerable impact on post treatment cervical cancer patients. These bothersome symptoms may be managed with hormone replacement therapy. There are few data on the safety of hormone replacement therapy following cervical cancer treatment, but the available data suggest that hormone replacement therapy does not increase the risk of recurrence31 32 and significantly decreases menopausal symptoms, with a favorable impact on quality of life.31 Ploch prospectively compared 80 women receiving hormone replacement therapy and 40 controls after surgery or radiotherapy with stage I or II cervical cancer over a period of 5 years.31 They found no difference in disease recurrence or overall survival between the two groups, with optimal menopausal symptom control in the hormone replacement therapy group. Further research investigating the use of hormone replacement therapy in a broader cervical cancer population is needed to support the use of this therapy in the management of treatment related sequelae.
The present study has some limitations. First, the efficacy analysis of the CIRCE trial showed that the experimental treatment (neoadjuvant chemotherapy in addition to chemoradiation) was inferior to standard treatment (chemoradiation alone). Thus comparisons of quality of life between the groups may have limited practical relevance as chemoradiation alone is more effective and remains the standard treatment. The main focus of this quality of life analysis was to understand quality of life aspects of patients with cervical cancer in general, treated with chemoradiation. The intention was to collect quality of life data during treatment. Because of irregular data collection during treatment, these data were not included in the analysis. Another major concern was compliance with the quality of life questionnaires. Considering patients that were still on the trial at 12 months, only 55% of patients in the neoadjuvant chemotherapy arm and 81.8% in the chemoradiation arm answered the questionnaires. Differences in compliance rates could be due to higher toxicities in the neoadjuvant chemotherapy group. Higher absolute numbers of toxicities were observed in the neoadjuvant chemotherapy arm, although the difference was statistically significant only for hypomagnesemia and neuropathy in the neoadjuvant chemotherapy group. Patients with more toxicities, and consequently more prolonged side effects, might be more likely to be non-responders of the quality of life questionnaires. The small final sample size that answered the questionnaires limits the power to compare the two study arms. In addition, the low compliance rates could be a source of bias and this may be a possible explanation for the between groups differences observed in quality of life.
Another limitation is that the study population included only Brazilian women treated in a public cancer center. Nevertheless, we believe that this group is representative of the major population of cervical cancer patients, which is constituted largely by patients from developing countries. We can also highlight the strengths of the study. First, data were obtained from a prospective randomized trial and addressed an important issue that should be discussed by physicians and patients. Recognizing the relevance of the measure, the quality of life analysis was predefined as a secondary endpoint of this prospective randomized trial. The data provided will inform areas of concern that should receive attention for prevention and treatment strategies. Other prospective studies evaluating new treatment strategies for cervical cancer should also investigate quality of life aspects, especially studies in larger populations. Moreover, future studies should also address possible strategies to improve quality of life after cervical cancer treatment.
In conclusion, the present study showed that most quality of life aspects improved after treatment for locally advanced cervical cancer, irrespective of the treatment modality. However, worsening was observed in menopausal symptoms and peripheral neuropathy. Importantly, patients with cervical cancer are mostly diagnosed at a young age and will live for many years with their treatment sequelae.33 This highlights the importance of medical awareness, early recognition, and intervention for these treatment related impairments. As quality of life is a relevant oncological endpoint, careful thought should be directed to these results.
References
Footnotes
Correction notice Since the online publication of this article, the authors have noticed that the initial H was missing from Geertruida H. de Bock's name. This has now been corrected.
Contributors Each author has substantially contributed to conducting the underlying research and drafting the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The ethics committee of the participating institution approved the study.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available. Data are not available due to confidential patient information.