Article Text

Statistics from Altmetric.com
Cervical cancer caused by persistent human papillomavirus (HPV) infection is still a major public health concern in sub-Saharan Africa. In Cameroon it represents the second most common cancer in women and the leading cause of cancer-related deaths. As in many other parts of sub-Saharan Africa, facilities for the prevention and treatment of this cancer are still very limited in this country.
Launched in September 2018 in partnership with the Cameroon Ministry of Public Health, the Dschang District Hospital and University Hospitals of Geneva, we designed a 5-year community-based cervical cancer screening program in West Cameroon1 (Figure 1). Historically, since 1980, a partnership has existed between the University of Geneva and the Cameroonian Ministry of Health with the aim of developing knowledge and promoting its exchange. In the domain of cervical cancer prevention, the partnership was established in 1999 and has led to the development of a highly productive research platform for medical students and young doctors.2–5

District Hospital of Dschang, Cameroon.
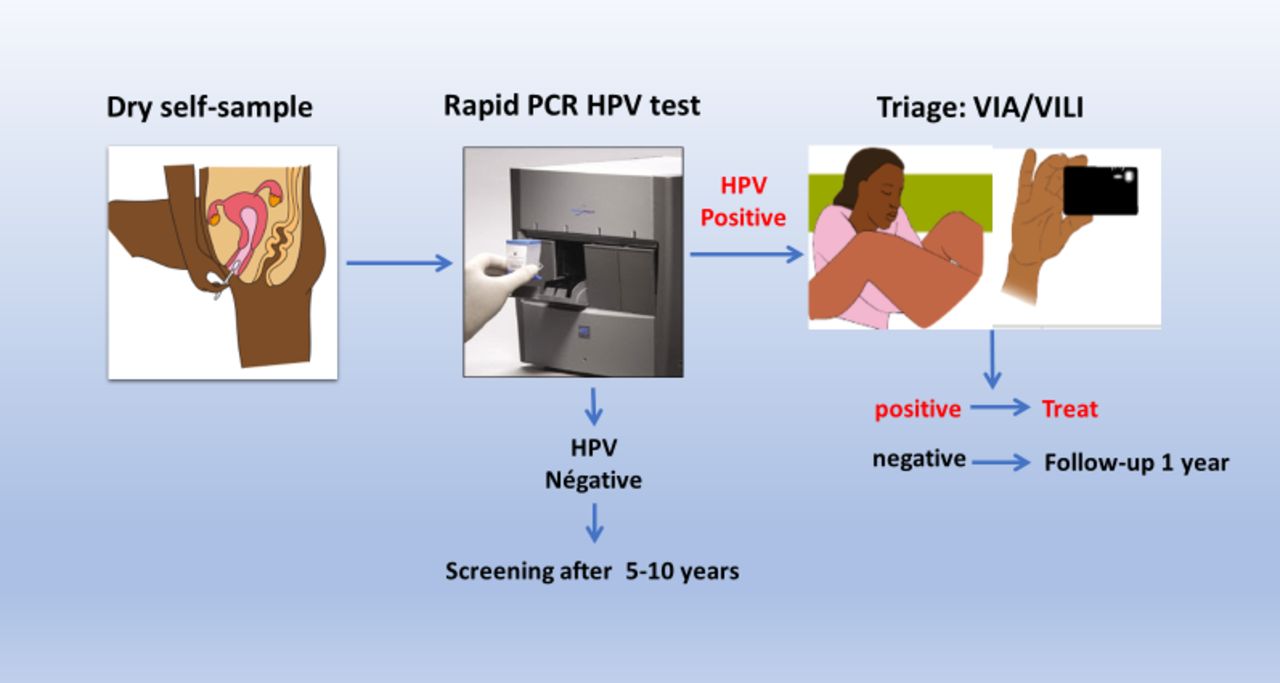
Our screening program, based on the WHO recommendation, entitled the '3T-Approach' (Test, Triage and Treat), is done in a single visit (Figure 2). Briefly, after counselling, a point-of-care rapid HPV self-test is performed followed by visual triage for HPV-positive women and treatment with thermal ablation if needed Figure 3. Smartphone digital photographs after visual inspection with acetic acid (VIA) and visual inspection with Lugol's iodine (VILI) (D-VIA/VILI) are also obtained for quality control as well as cytology, biopsies, and endocervical brushing for program evaluation (Figure 4). We decided to organize and sustain our program in a well-defined geographical area of West Cameroon (Dschang Health District) before expanding to cover the region. In this brief contribution we report our 18-month experiences and achievements in an ongoing community-based cervical cancer screening program.

'3T-Approach' strategy procedure – 1 day visit. Self-sampling with a dry swab is followed by rapid human papillomavirus (HPV) testing (Xpert™ HPV). HPV-negative women are reassured and advised to do the next screening 5 years later. HPV-positive women will undergo visual inspection with acetic acid and visual inspection with iodine (VIA/VILI) and treatment (if indicated) or follow-up. Smartphone digital photographs (cervicograms) are obtained for quality control. Source: Vassilakos et al, Rev Med Suisse (March 2019).

District Hospital of Dschang: women receive counselling service (community education, counselling on sexual health and cervical cancer screening) before testing.
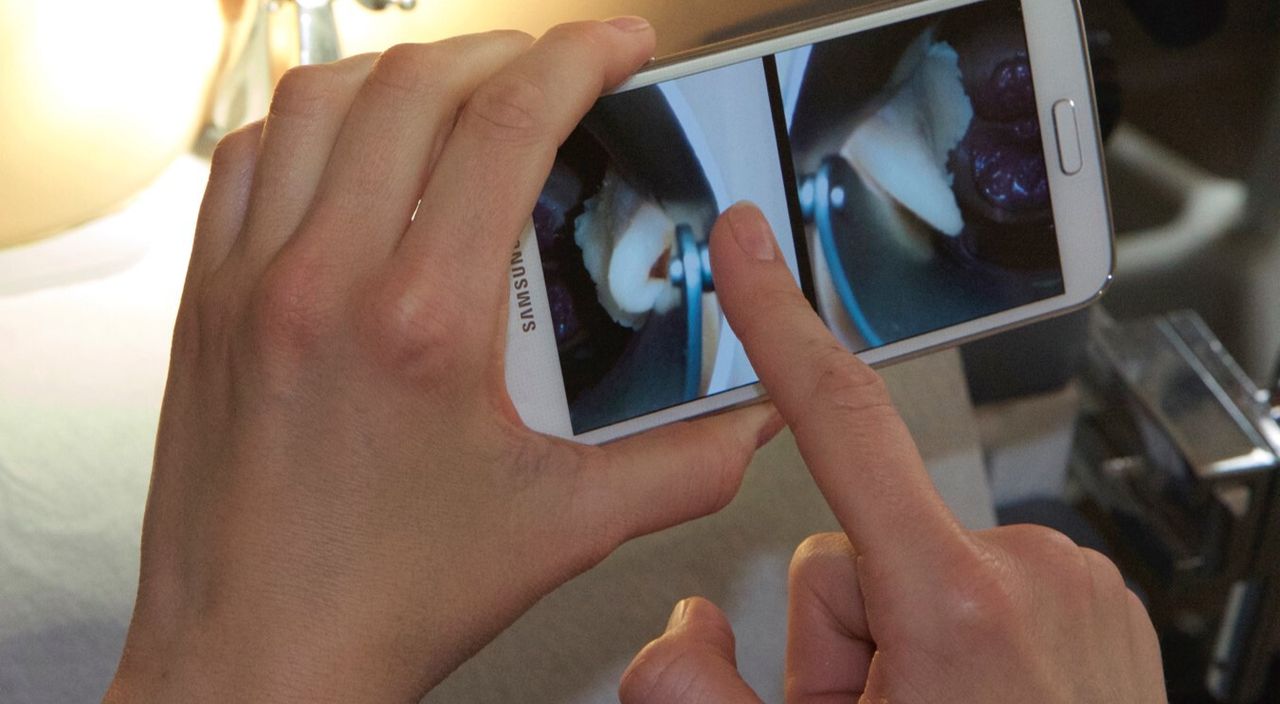
Smartphone digital images acquisition after VIA (D-VIA) and VILI (D-VILI) procedures. This allow to slide between pictures on the Smartphone for diagnosis. It is a simple and reproducible procedure that facilitates the identification of lesion.
Cervical cancer screening program (3T-Approach)
Setting
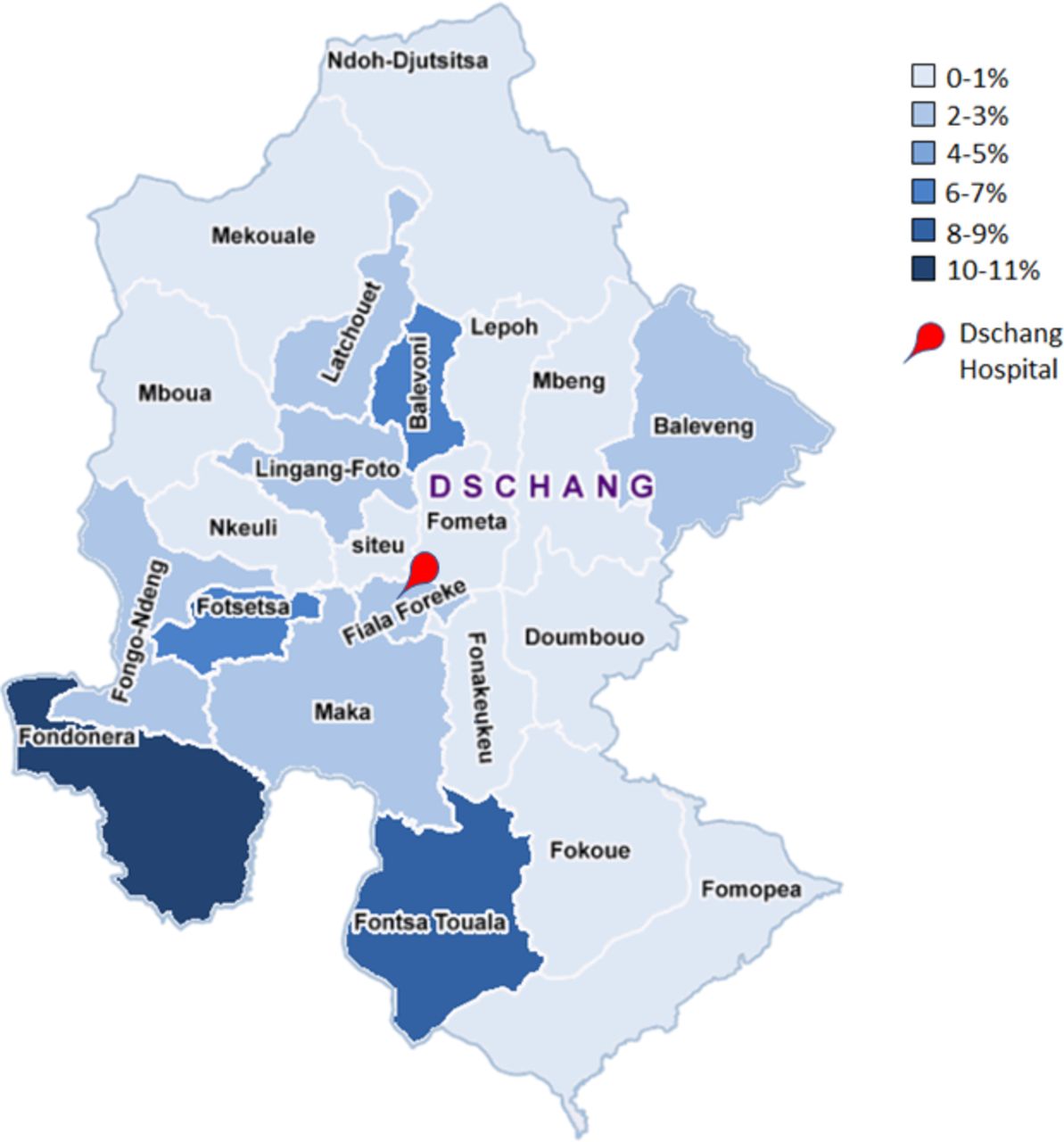
The program started in the city of Dschang and surrounding villages in September 2018. We estimated that about 10 000 women in this zone aged 30–49 years were eligible for a cervical cancer screening test. Screening coverage is regularly monitored for communication and intervention planning with community health workers in order to enhance participation of women in the program (Figure 5). Social educators trained to provide information about cervical cancer and its screening play a major role. They provide information in villages, churches, markets, and women's associations and encourage women to participate. They educate people on positive health-seeking behaviors, about the importance of HPV infection and timely screening and treatment of pre-cancerous lesions. A free consultation is emphasized.
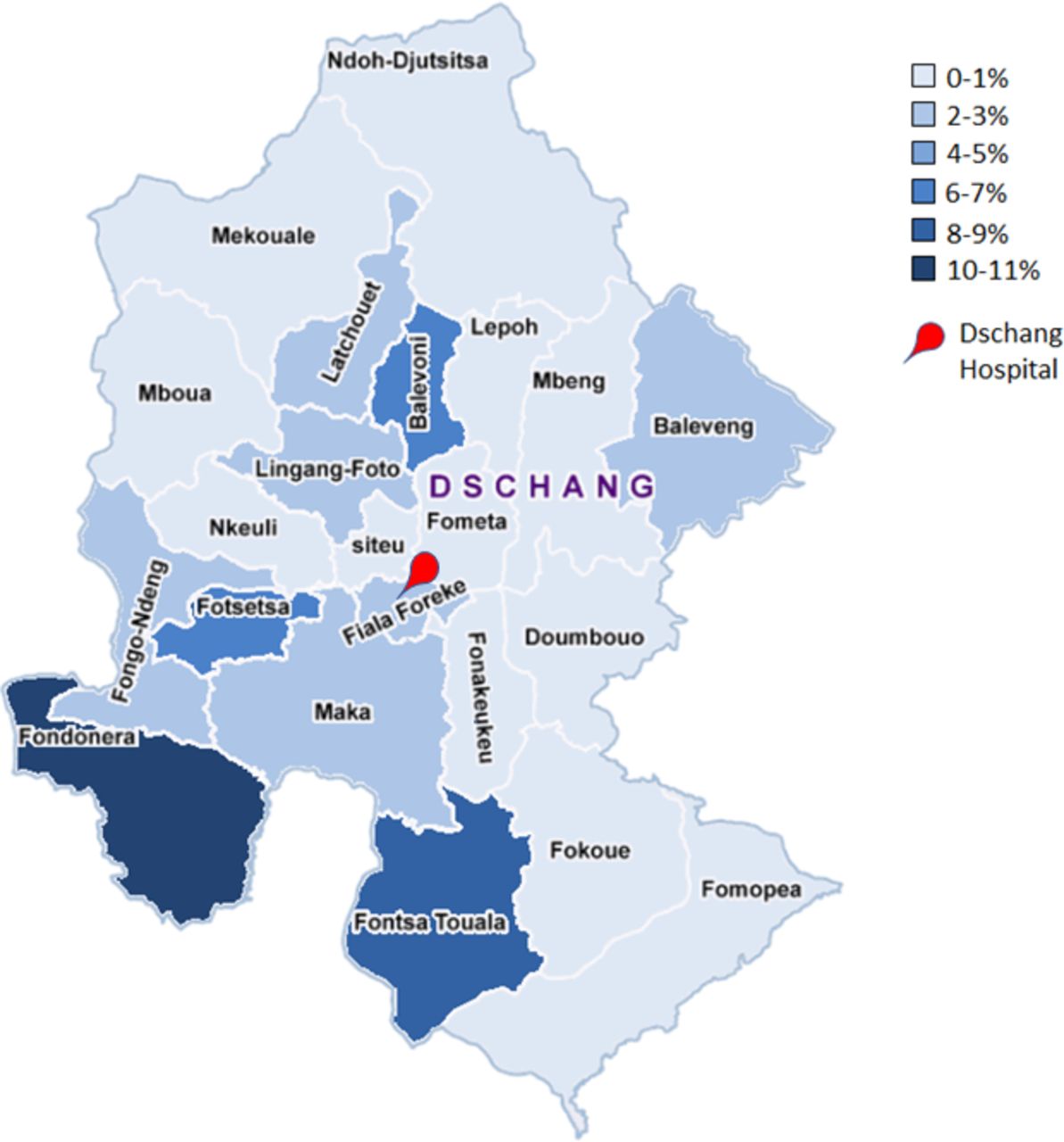
District of Dschang, West Cameroon. A detailed map allows monitoring and evaluation of screening coverage rates (women 30–49 years). This is an example of a map showing rates of coverage during the second half of 2019.
Training of staff
Local staff were trained through an e-learning process (www.gfmer.ch) and with on-site training conducted by physicians from the University of Dschang and Geneva University Hospitals. One week of a theoretical course followed by 1 week of practical training on VIA, VILI, Smartphone images acquisition and thermal ablation using anatomical models was given to healthcare providers performing the screening (Figure 6). After 2 weeks of training, a review of photographs of normal and abnormal cervix as well as clinical sessions to observe and practice the techniques were organized. At the end of the training, a theoretical and practical examination was performed to ensure that all the necessary skills were acquired. Healthcare providers received certification after an examination from the University of Dschang and Geneva.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Smartphone training of health care providers for VIA and VILI digital image acquisition (D-VIA/D-VILI).
Program monitoring and evaluation
A set of benchmark indicators was developed to quantitatively evaluate how the screening and treatment program is progressing towards expected results. This permits early detection of potential problems. Results-at-a-Glance posters are given periodically to the staff in order to assess the screening performance. Based on our previous studies, we defined nine indicators including corresponding targets against which performance is assessed (Table 1).
Performance monitoring indicators and targets for the screening program
Ongoing training of providers
In order to enhance program performance, all providers met weekly with a supervising consultant gynecologist to review and discuss the digital images (D-VIA/VILI) of HPV-positive women and discuss treatment and referral decisions. Digital images of the cervix are also used for education (photos for review meetings and case studies).
Performance of the visual triage (VIA/VILI)
We use 'relaxed WHO criteria', meaning that any aceto-white lesion with faint whitening in the transformation zone is considered as VIA-positive. A VILI-positive test is defined as an iodo-negative area that takes a mustard or saffron yellow color. To examine the performance characteristics of VIA/VILI among HPV-positive women, standard test metrics (sensitivity, specificity, positive predictive value, and negative predictive value) are calculated. Results from histopathological examinations of cervical tissue obtained from biopsies and endocervical brushing are used as the gold standard to evaluate accuracy. Guided biopsies are performed on all visible lesions. If no lesion is seen, a random biopsy from 6 o’clock within the transformation zone and near the squamo-columnar junction are obtained accompanied by an endocervical brushing.
Cure rate and evaluation of overtreatment at 12 months
Cure rate was defined as the percentage of women with no evidence of disease at 12 months after a baseline diagnosis of cervical intra-epithelial neoplasia (CIN) 2 or CIN 3. Overtreatment was defined as treatment of women who either had no lesion or had CIN 1 lesions on baseline cervical biopsies and endocervical curettage and cytology was negative for a high grade squamous intra-epithelial lesion.
Cost analysis of the program
Cost analysis of the 5-year program will include staff time and salaries, clinical and laboratory supplies, laboratory and treatment equipment, start-up costs, training, and community mobilization costs. This also includes the cost for treatment of patients with invasive cancer diagnosed after screening. Additionally, we will analyze costs per woman and per pre-cancer and cancer diagnosed through a 5-year period modeling.
Conclusion
Considering the local specificities and available resources, we believe after 18 months of implementation and experience in Dschang that the program can be expanded to the region at large. Key pillars for the success of the program include providing adequate training and educational tools as well as developing a culture of quality among the healthcare workers. Future reports on clinical outcomes and cost analysis will contribute to optimizing a strategic plan for cervical cancer prevention in low- and middle-income countries.
Acknowledgments
The authors would like to thank Chloé Frund, Jessica Sormani, Jovanny Fougue, Alexia Chatillon, Christine Balli, Hélène Gaitsch, Karolin Tatrai, Rosa Catarino, Fritz Baumann, Beat Stoll, Atem Bethel Ajong.
Footnotes
Contributors All the authors made contributions to the design and participated in drafting and revising the manuscript. All authors gave final approval of the submitted version.
Funding This research is supported by the University Hospitals of Geneva (Commission des Affaires Humanitaires (CAH)), Solidarité Internationale Genève, ESTHER Switzerland Partnership Project Grant (17G1), District Hospital of Dschang. The authors have not declared a specific grant for this research from commercial sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Commissioned; internally peer reviewed.