Article Text

Abstract
Objective Only few studies have focused on tumor markers used in the preoperative diagnosis of endometriosis-related ovarian neoplasms, and previous studies have only assessed serum CA125 levels. This study investigated the significance of preoperative tumor markers and clinical characteristics in distinguishing endometriosis-related ovarian neoplasms from ovarian endometrioma.
Methods A case-control study was conducted on 283 women who were diagnosed with confirmed pathology with endometriosis-related ovarian neoplasms (n=21) and ovarian endometrioma (n=262) at a single institution from April 2008 to April 2018. The serum CA125, CA19–9, carcinoembryogenic antigen (CEA), sialyl Lewis-x antigen (SLX), and lactate dehydrogenase (LDH) levels, age, tumor size, and the presence of mural nodule of the patients were analyzed.
Results Patients with endometriosis-related ovarian neoplasms were more likely to be older (48 (range, 26–81) vs 39 (range, 22–68) years, P<0.001), have higher levels of CA19–9 (42 vs 19 U/mL, P=0.013), CEA (1.3 vs 0.84 ng/mL, P=0.007), SLX (41 vs 33 U/mL, P=0.050), and LDH (189 vs 166 U/mL, P<0.001) and larger tumor size (79 vs 55 mm, P=0.001), and present with mural nodule (85.7 vs 4.5 %, P<0.001) than those with ovarian endometrioma. The CA125 levels did not significantly differ between the two groups. The area under the curve for each factor was as follows: CA19-9 level, 0.672 (95% CI 0.52 to 0.83; P=0.013); CEA level, 0.725 (95% CI 0.58 to 0.87; P=0.007); SLX level, 0.670 (95% CI 0.53 to 0.84; P=0.050); LDH level, 0.800 (95% CI 0.70 to 0.90; P<0.001); age, 0.775 (95% CI 0.65 to 0.90; P<0.001); and tumor size, 0.709 (95% CI 0.56 to 0.86; P=0.001). Age was a better marker than CA19-9, CEA, and SLX levels according to the receiver operating characteristic curve analysis. The optimal cut-off values for age and tumor size were 47 years and 80 mm, respectively.
Conclusions The assessment of serum CA19–9, CEA, SLX, and LDH levels may be a useful tool in the preoperative evaluation to differentiate between endometriosis-related ovarian neoplasms and ovarian endometrioma.
- ovarian neoplasms
- ovarian cysts
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, an indication of whether changes were made, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Highlights
Endometriosis-related ovarian neoplasms was more likely to have higher levels of CA19-9, CEA, SLX, and LDH when compared with CA125.
CA125 levels did not significantly differ between the two groups.
Age, tumor size, and the presence of mural nodule were important factors in the preoperative prediction of endometriosis-related ovarian neoplasms.
Introduction
Endometriosis may be associated with a subset of histologic subtypes of ovarian cancer.1–3 Both ovarian clear cell carcinoma and endometrioid carcinoma are often associated with endometriosis,4–6 sharing similar histogenesis and pathogenesis,7 and are known as endometriosis-associated ovarian cancer. Endometrioid ovarian carcinomas differ from high-grade serous ovarian cancers at the mutational level.8 Moreover, seromucinous borderline tumor, which is similar to endocervical-like mucinous borderline tumor or mixed-epithelial papillary cystadenoma of borderline malignancy of Mullerian type, is commonly found in an ovarian endometriotic cyst.9–11 Several immunohistochemical studies have shown that seromucinous borderline tumor is likely to originate from ovarian endometrioma.12 13 The inactivating mutations of the ARID1A tumor suppressor gene are uniquely correlated with ovarian clear cell carcinoma, ovarian endometrioid carcinoma, and seromucinous borderline tumor. Thus, these tumors are collectively called endometriosis-related ovarian neoplasms.14–16
The presence of mural nodule suggests malignancy, and solid masses and papillary projections in ovarian endometriomas were the most common forms mimicking ovarian cancer on sonographic morphology.17 Therefore, sonographic appearances are generally less objective. Meanwhile, according to the International Ovarian Tumor Analysis (IOTA) studies, transvaginal ultrasound characteristics could contribute to the improvement of the management of suspicious ovarian masses.18 19 However, only few reports have focused on tumor markers that can be used for the preoperative diagnosis of endometriosis-related ovarian neoplasms, and previous studies have only assessed serum CA125 levels.20 21 Human epididymis protein 4 (HE4) or the Risk of Malignancy Algorithm (ROMA) can possibly distinguish epithelial ovarian cancer from ovarian endometriosis,22–24 but HE4 is not frequently used in Japan. This study aimed to assess the significance of preoperative tumor markers and clinical characteristics in distinguishing endometriosis-related ovarian neoplasms from ovarian endometrioma.
Methods
From April 2008 to April 2018, 21 women with endometriosis-related ovarian neoplasms and 267 women with ovarian endometrioma were included in the study. All patients had been histologically diagnosed at a single institution according to the World Health Organization 2014 criteria, and those with borderline or malignant cells with endometriosis in the same ovary were diagnosed with endometriosis-related ovarian neoplasms. Clinical staging was determined in accordance with the International Federation of Gynecology and Obstetrics 2014 criteria.
Serum CA125, CA19-9, carcinoembryogenic antigen (CEA), sialyl Lewis-x antigen (SLX), and lactate dehydrogenase (LDH) levels were measured preoperatively. Doctors selected a combination of tumor makers to measure in each case. Thus, there was a lack of data for some tumor markers. Patients were excluded from a control group due to the absence of any information for tumor markers. The cut-off value for the serum CA125 level was set at 35 U/mL; CA19-9 level, 37 U/mL; CEA level, 5 ng/mL; SLX level, 38 U/mL; and LDH level, 211 U/mL. The maximum tumor diameter and the presence of mural nodule in the tumor were determined via MRI. No eligible patient declined to participate in this study.
The ethics committee of Nippon Medical School Musashikosugi Hospital approved this retrospective study (432-30-3).
Endometriosis-related ovarian neoplasms and ovarian endometrioma were compared using the Mann–Whitney U test and Fisher’s exact test. Diagnostic efficiency was calculated as sensitivity multiplied by specificity. A receiver operating characteristics (ROC) curve analysis was conducted to identify optimal cut-off values, and the area under the curve (AUC) was evaluated to assess for a valuable marker. A P-value<0.05 was considered statistically significant in all analyzes. Statistical analyzes were conducted using the Statistical Package for the Social Sciences software for Windows (version 23.0, IBM Corp., Armonk, NY, the USA).
Results
A total of 288 women were included in this study. Among them, five women with ovarian endometrioma were excluded due to lack of any information for tumor markers. Therefore, 21 women with endometriosis-related ovarian neoplasms and 262 women with ovarian endometrioma were analyzed in the study. Of all patients with endometriosis-related ovarian neoplasms (n=21), four patients presented with ovarian clear cell carcinoma; five patients with ovarian endometrioid carcinoma; and 10 patients with seromucinous borderline tumor. A total of 20 patients had stage I endometriosis-related ovarian neoplasms, and the remaining patient had stage IV ovarian endometrioid carcinoma. The median size of endometriosis-related ovarian neoplasms was 79 mm (range; 27–159).
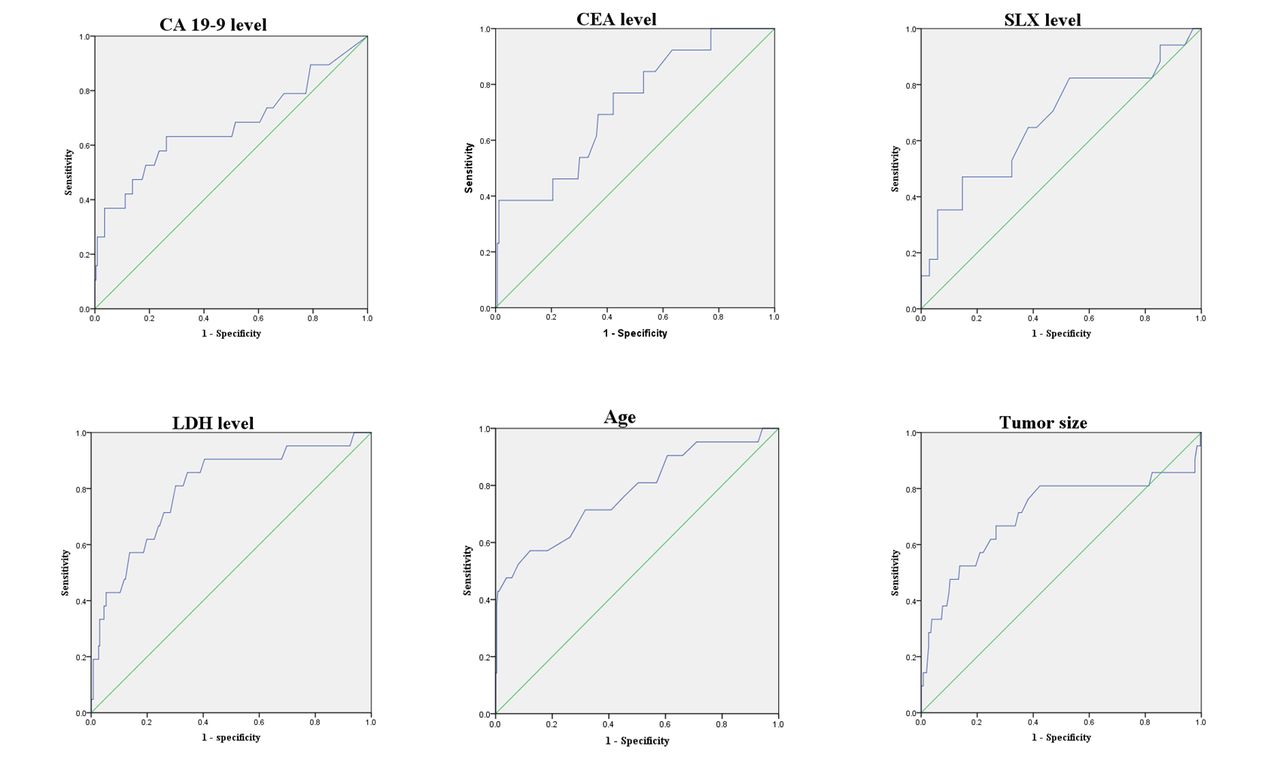
Figure 1 shows the distribution of patients with endometriosis-related ovarian neoplasms and ovarian endometrioma in terms of CA125, CA19-9, CEA, SLX, and LDH levels, age, and tumor size. CA19-9, CEA, SLX, LDH levels, age, maximum tumor diameter, and the presence of mural nodule (except for CA125 levels) were significantly different between the two groups (Table 1). The sensitivity, specificity, and diagnostic efficiency of tumor markers are shown in Table 2. For factors that were significantly different, the ROC curves were obtained to define the optimal cut-off values. The AUC for each factor was as follows: CA19-9 level, 0.67 (95% CI 0.52 to 0.83; P=0.013); CEA level, 0.725 (95% CI 0.583 to 0.866; P=0.007); SLX level, 0.670 (95% CI 0.53 to 0.84; P=0.05); LDH, 0.800 (95% CI 0.70 to 0.90; P<0.001); age, 0.775 (95% CI 0.65 to 0.90; P<0.001); and tumor size, 0.709 (95% CI 0.56 to 0.86; P=0.001) (Figure 2). The ROC curve analysis showed that lactate dehydrogenase level was a better screening marker for endometriosis-related ovarian neoplasms, and age was a better screening marker than CA19-9, CEA, and SLX levels.
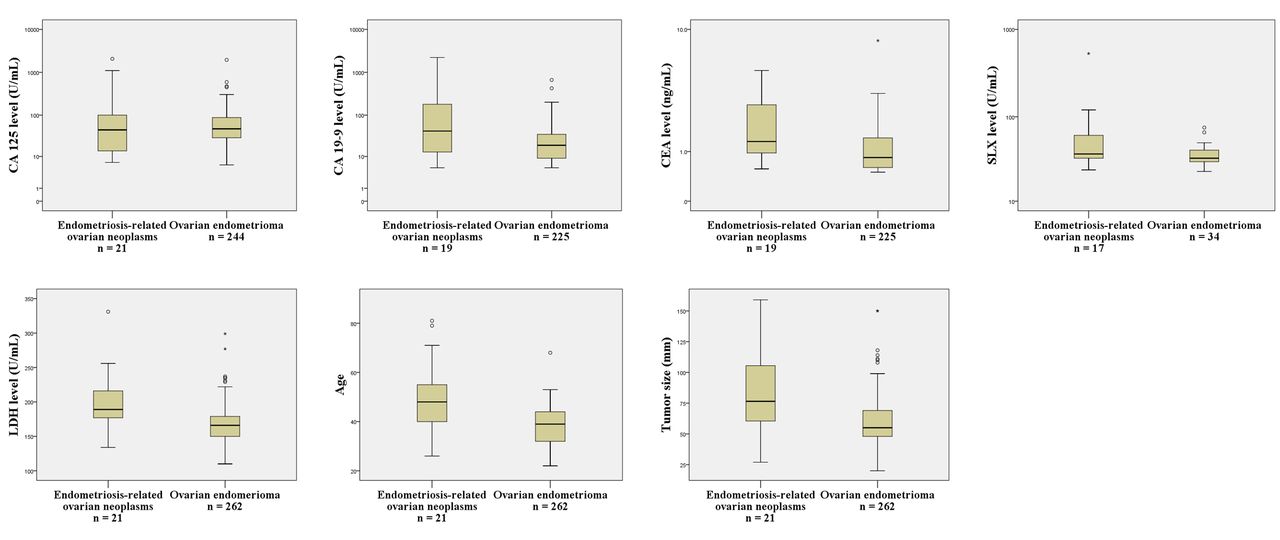
Distribution of patients with endometriosis-related ovarian neoplasms and ovarian endometrioma in terms of clinical characteristics.

{kind=link}
{kind=link}
Results of the receiver operating characteristic curve analysis.
Values of serum tumor markers and tumor characteristics
Sensitivity, specificity, and diagnostic efficiency of the tumor markers
Using the ROC curves, optimal cut-off values were determined, and the sensitivity, specificity, and diagnostic efficiency of each factor were obtained again (Table 3). In every tumor marker, the optimal cut-off values for sensitivity, specificity, and diagnostic efficiency improved, which were as follows: CA19-9 level, 41 U/mL; CEA level, 2.7 ng/mL; SLX level, 32 U/mL; LDH level, 175 U/mL; age, 47 years; and tumor size, 80 mm.
Area under the curve, optimal cut-off value, sensitivity, specificity, and diagnostic efficiency of the tumor markers and clinical characteristics
Discussion
Our study showed that CA19-9, CEA, SLX, and LDH levels were significantly different between patients with endometriosis-related ovarian neoplasms and ovarian endometrioma. The ROC curves showed that LDH level was a better screening marker for endometriosis-related ovarian neoplasms. We also showed that age, tumor size, and the presence of mural nodule were important factors in the preoperative prediction of endometriosis-related ovarian neoplasms. By contrast, in this study, CA125 levels did not significantly differ between the two groups.
Several studies about the use of serum CA125 levels20 21 have been conducted. However, the results were conflicting.25 Two reports have shown no significant difference in terms of CA125 levels between patients with endometriosis-associated ovarian cancers and ovarian endometrioma.26 27 One report has shown that patients with endometriosis-associated ovarian cancer had lower CA125 levels than those with typical epithelial ovarian cancer.28 Previously published results about CA125 for endometriosis-associated ovarian cancers are summarized in Table 4. Serum CA125 combined with transvaginal ultrasound has been commonly applied in the differential diagnosis of adnexal masses.29 According to the IOTA studies, transvaginal ultrasound could be useful in the preoperative diagnosis of epithelial ovarian cancer.18 19 Conversely, serum CA125 may not be very useful for endometriosis-associated ovarian cancers.
Efficacy of CA125 for endometriosis-associated ovarian cancers
In 2008, the United States Food and Drug Administration approved human epididymis protein 4 (HE4) as a tumor maker. Serum HE4 may be a useful biomarker in the differential diagnosis between epithelial ovarian cancer and endometriosis.22 23 Biomarker algorithms combining serum CA125 and HE4, such as the ROMA and, more recently, the Copenhagen Index (CPH-I), were reportedly useful for predicting malignancy in patients with pelvic masses.24 However, a cohort study showed that HE4 had no additional value to the concurrent use of serum CA125 and transvaginal ultrasound in diagnosing ovarian cancer among postmenopausal women with adnexal masses.29 The usefulness of serum HE4 as a tumor marker remains controversial. HE4 is still uncommon in Japan, therefore, we could not include HE4, the ROMA, and the Copenhagen Index in this study because of its retrospective nature.
Unlike benign endometrioma, the treatment of ovarian borderline tumor usually requires oophorectomy. Therefore, it would be of value to diagnose endometriosis-related ovarian borderline tumor preoperatively. However, no study on tumor makers used for the diagnosis of endometriosis-related ovarian borderline tumor has been conducted. Age, tumor size, and the presence of mural nodule were informative factors for the preoperative prediction of endometriosis-related ovarian neoplasms. The presence of mural nodules on MRI is a strong indicator of ovarian malignancy.30 A case-control study on endometriosis-associated ovarian cancer has shown that a solid component in imaging had an independent OR of 23.7 for malignancy. In addition, the tumor size in patients with endometriosis-associated ovarian cancer was larger (14 vs 7.5 cm), and age ≥49 years had high sensitivity (80.6%) and specificity (82.9%) for endometriosis-associated ovarian cancer.16
Our study had some limitations. First, this is a retrospective study, which has a relatively small number of endometriosis-related ovarian neoplasms cases (n=21). In this study, nonsurgical patients and patients with no data for tumor makers were excluded from a control group. Thus, selection bias might have affected the study results. Second, there is a large proportion of patients with seromucinous borderline tumor. In conventional studies in this field, clear cell carcinoma or endometrioid carcinoma is common, thus bias in histological studies could affect outcomes. Third, this study had insufficient data about some of the tumor markers. In clinical practice, we left the selection of tumor markers to the discretion of physicians, thus some data regarding tumor markers could have been missed.
This study showed that CA19-9, CEA, SLX, and LDH levels may be useful in the preoperative diagnosis of endometriosis-related ovarian neoplasms. These tumor markers are conventionally used in Japan. However, only few reports have focused on tumor markers, other than CA125 levels, for the preoperative diagnosis of endometriosis-associated ovarian cancer.
Acknowledgments
The authors would like to thank Enago (www.enago.jp) for the English language review.
References
Footnotes
Twitter @Youhei Tsunoda
Contributors HS and KY wrote the first draft. HS, KY, EH, YT, TF, and TM contributed to data collection. HS, KY, and YT contributed to data analysis. All authors contributed to study design, data interpretation, and the manuscript revision. The corresponding author (HS) took on final responsibility for the decision to submit to this journal.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. Address correspondence and reprint requests to Hiroki Shinmura, MD, Deprtment of Obstetrics and Gynecology, Musashikosugi Hospital, 1-396 Kosugicho, Nakahara-ku, Kawasaki-shi, Kanagawa, Japan. E-mail: h-shimmura@nms.ac.jp.